Endocrine pancreas
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
I now have thorough content from multiple authoritative textbooks. Let me compile the full comprehensive answer.
The Endocrine Pancreas
Overview
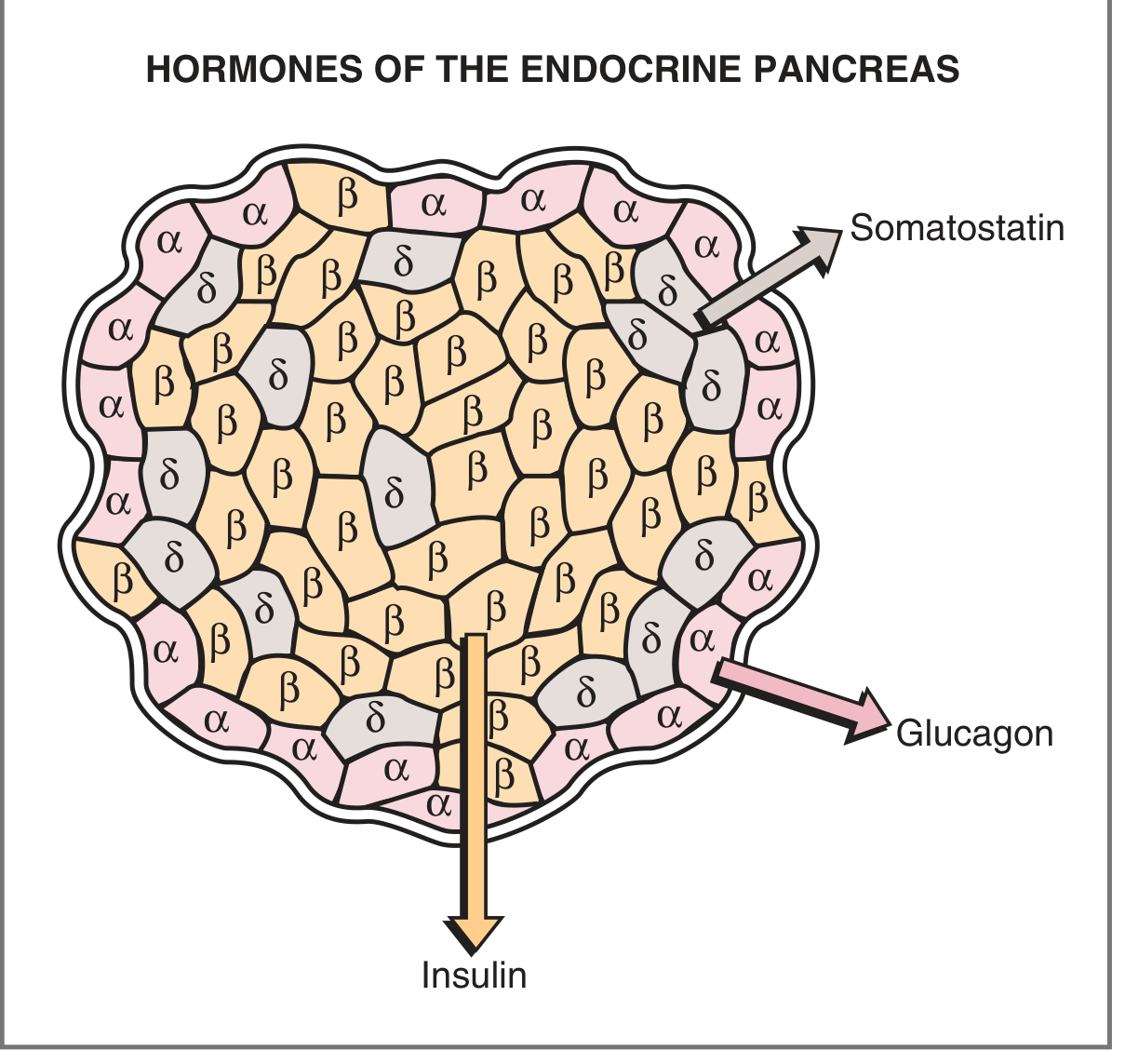
The endocrine pancreas is a diffuse organ scattered within the exocrine gland whose primary function is regulating blood glucose, fatty acid, and amino acid metabolism. It secretes four major hormones: insulin, glucagon, somatostatin, and pancreatic polypeptide (PP).
1. Islets of Langerhans - Structure & Histology
The endocrine cells are organized into clusters called the islets of Langerhans, which make up only 1-2% of total pancreatic mass. There are approximately 1 million islets, each containing about 2,500 cells, most numerous in the tail of the pancreas.
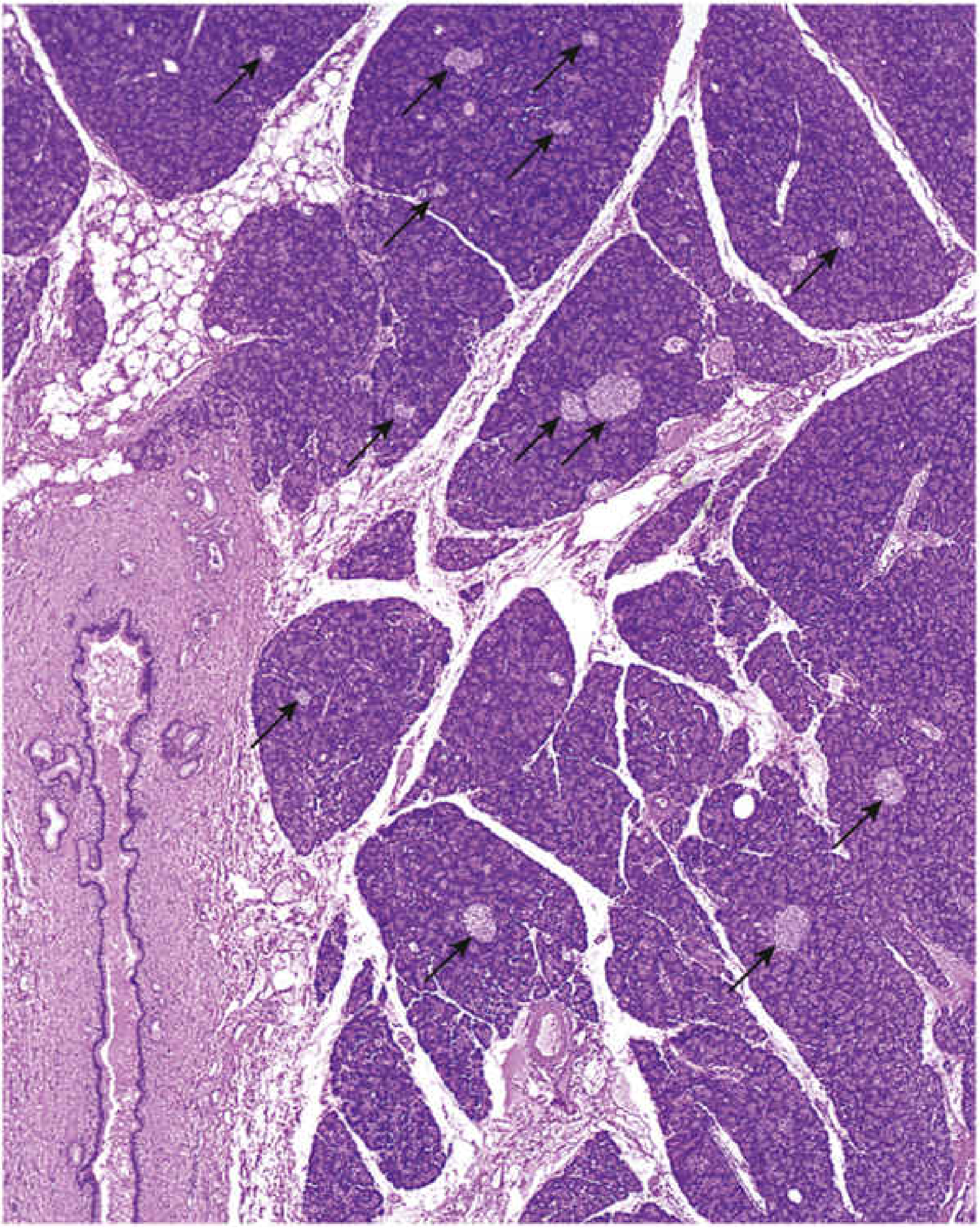
H&E-stained pancreas: islets appear as round, pale-staining profiles (arrows) scattered among more intensely staining exocrine acini. - Histology: A Text and Atlas
Each islet consists of polygonal cells arranged in short, irregular cords, profusely invested with fenestrated capillaries. The cells develop between weeks 9-12 of gestation.
Cell Types
| Cell Type | % of Islet | Hormone | Mallory-Azan Stain | TEM Granules |
|---|---|---|---|---|
| B (β) | 60-70% | Insulin | Brownish orange | ~300 nm; dense, crystalline angular core |
| A (α) | 15-20% | Glucagon | Red | ~250 nm; dense eccentric core, light halo |
| D (δ) | 5-10% | Somatostatin | Blue | ~325 nm; homogeneous matrix |
| PP | ~5% | Pancreatic polypeptide | - | Small, irregular granules |
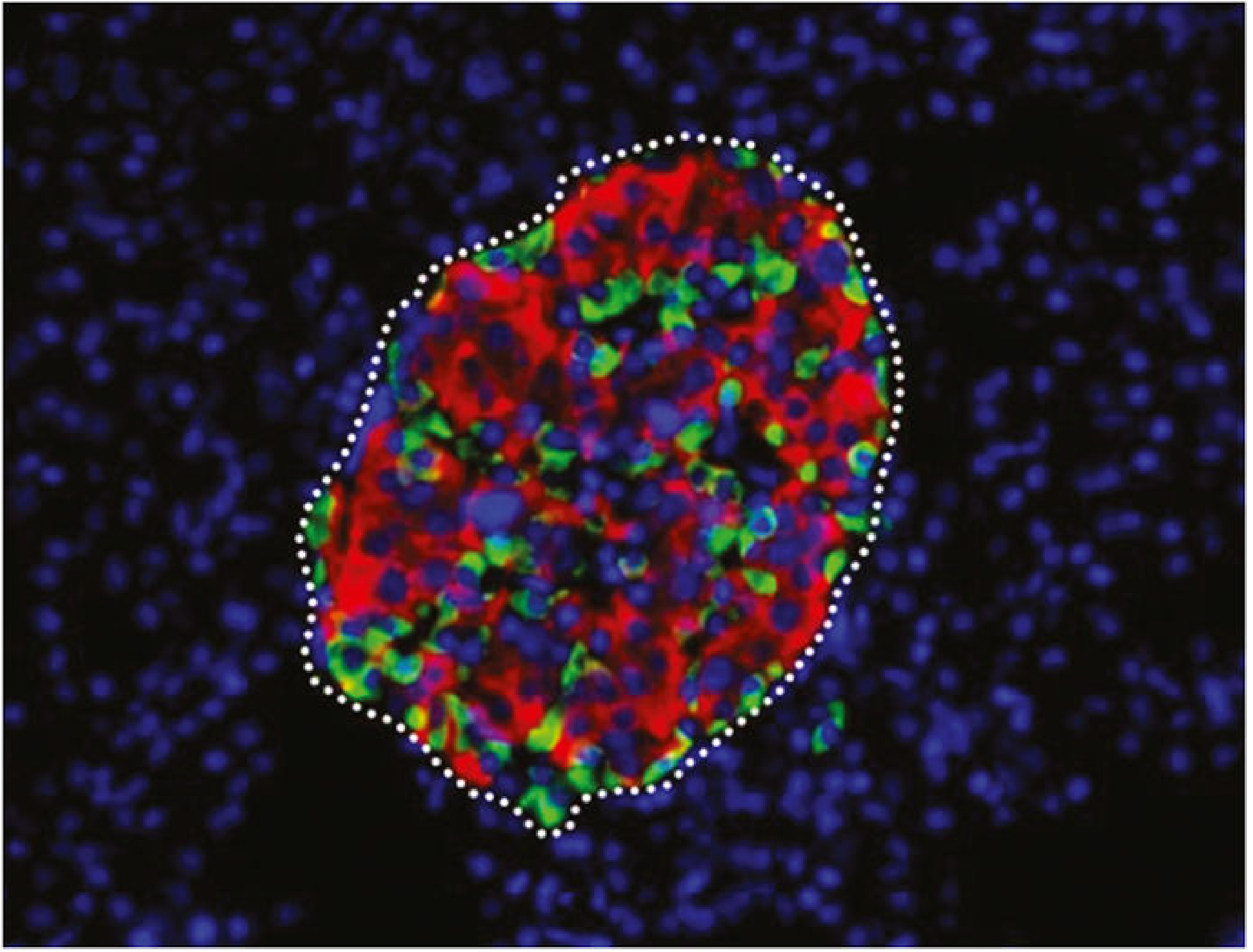
Spatial arrangement: β cells occupy the central core; α cells line the outer rim; δ cells are interposed between α and β cells, allowing paracrine communication.
Intra-islet Communication (Paracrine Mechanisms)
There are three communication pathways between islet cells:
- Gap junctions - connect α-to-α, β-to-β, and α-to-β cells for rapid ionic and molecular transfer
- Blood supply - arteries enter the islet core and flow outward; venous blood from β cells (carrying insulin) bathes α and δ cells before leaving the islet
- Innervation - adrenergic, cholinergic, and peptidergic neurons; δ cells have neuron-like processes extending onto β cells
2. Insulin
Synthesis
Insulin is encoded on chromosome 11. The biosynthetic sequence is:
Preproinsulin → (signal peptide cleaved) → Proinsulin → (C-peptide cleaved) → Insulin + C-peptide
- Insulin = two chains: A chain (21 amino acids) + B chain (30 amino acids), linked by disulfide bridges
- Proinsulin folds in the ER; packaged in Golgi secretory granules; proteases cleave C-peptide during packaging
- Insulin and C-peptide are co-secreted in equimolar amounts - C-peptide measurement reflects endogenous β-cell function (useful in insulin-treated patients)
- Metabolized in liver and kidney by disulfide-cleaving enzymes
Regulation of Insulin Secretion
Mechanism (glucose-stimulated):
- Glucose enters β cell via GLUT2 transporter
- Phosphorylated to glucose-6-phosphate by glucokinase (rate-limiting step)
- Oxidative metabolism generates ATP
- ↑ ATP/ADP ratio closes ATP-sensitive K⁺ channels (K_ATP)
- Membrane depolarization opens voltage-gated Ca²⁺ channels
- ↑ Intracellular Ca²⁺ triggers exocytosis of insulin granules
| Stimulatory Factors | Inhibitory Factors |
|---|---|
| ↑ Blood glucose | ↓ Blood glucose / fasting |
| ↑ Amino acids | Somatostatin |
| ↑ Fatty acids & ketoacids | α-Adrenergic agonists |
| Glucagon | Diazoxide |
| Cortisol | Exercise |
| GIP (incretin) | - |
| Vagal stimulation / acetylcholine | - |
| Sulfonylurea drugs (close K_ATP) | - |
| Obesity | - |
Actions of Insulin ("Hormone of the Fed State")
Insulin acts on liver, muscle, and adipose tissue via its tyrosine kinase receptor:
Carbohydrate metabolism:
- ↑ GLUT4 insertion in muscle and adipose → ↑ glucose uptake → ↓ blood glucose
- ↑ Glycogen synthesis (liver and muscle)
- ↓ Glycogenolysis
- ↓ Gluconeogenesis (via ↑ fructose-2,6-bisphosphate → ↑ phosphofructokinase)
Fat metabolism:
- ↑ Fat deposition; ↓ lipolysis in adipose
- ↓ Ketoacid (β-hydroxybutyrate, acetoacetate) formation in liver
Protein metabolism (anabolic):
- ↑ Amino acid uptake into cells; ↑ protein synthesis; ↓ protein degradation
Other:
- ↑ Na⁺-K⁺ ATPase activity → ↑ K⁺ uptake into cells → ↓ serum K⁺
- Growth-promoting effects
3. Glucagon
Synthesis & Secretion
Glucagon is a 29-amino acid peptide secreted by α cells. It is the hormone of starvation/fasting, counter-regulatory to insulin.
| Stimulatory | Inhibitory |
|---|---|
| Fasting / ↓ blood glucose | Insulin |
| ↑ Amino acids (arginine, alanine) | Somatostatin |
| CCK (fat/protein ingestion) | ↑ Fatty acids & ketoacids |
| β-Adrenergic agonists | - |
| Acetylcholine | - |
Key point: Insulin modulates glucagon release - in type 1 DM (no insulin), the glucagon response to hypoglycemia is exaggerated. Amino acids stimulate glucagon (but this effect is blunted by simultaneous glucose - opposite to insulin, which is stimulated by both).
Mechanism of Action
Glucagon binds its receptor → Gs protein → adenylyl cyclase → ↑ cAMP → PKA → phosphorylation of enzymes
Actions of Glucagon (primarily on liver)
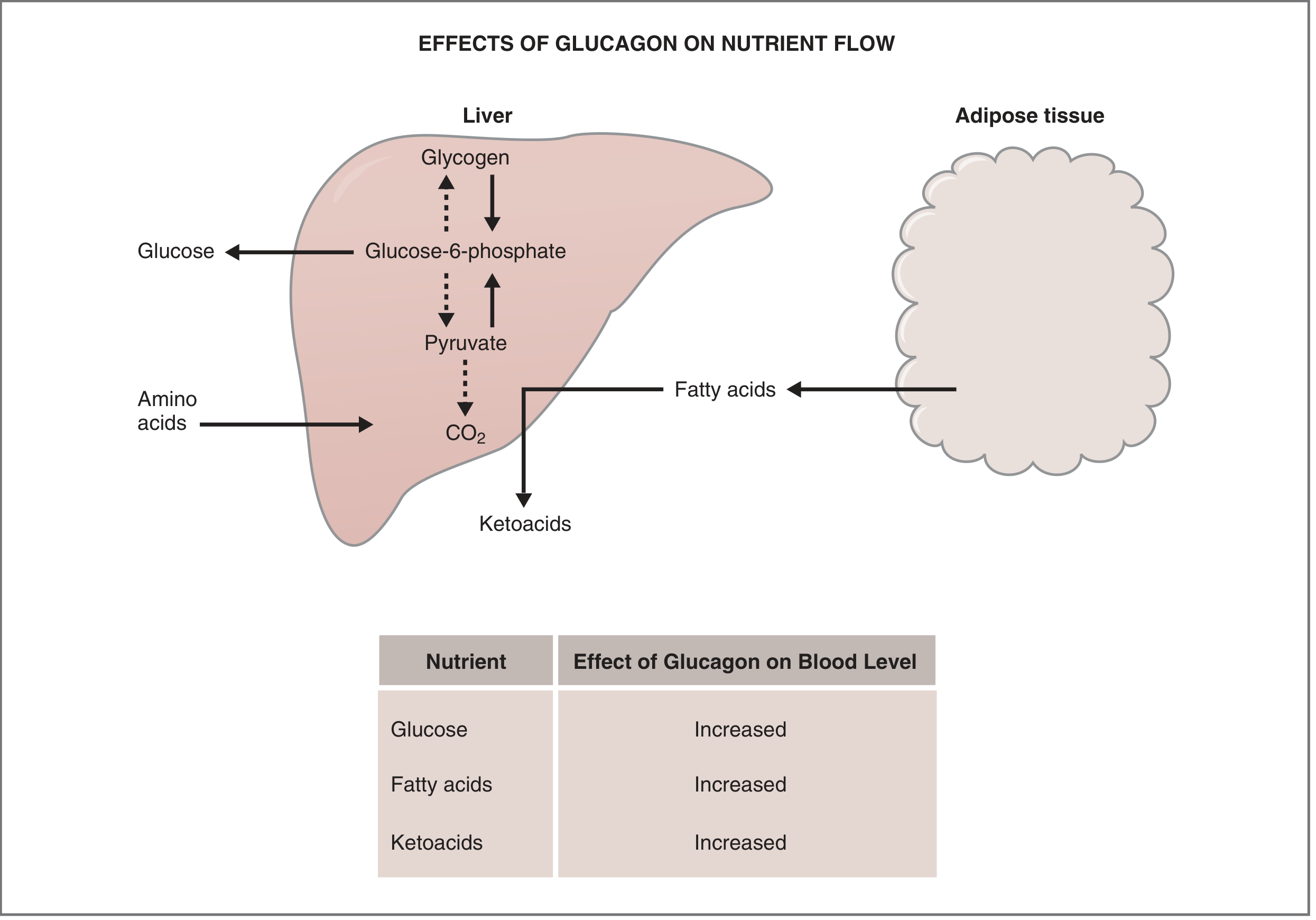
| Action | Effect on Blood Level |
|---|---|
| ↑ Glycogenolysis (liver) | ↑ Glucose |
| ↑ Gluconeogenesis | ↑ Glucose |
| ↑ Lipolysis (adipose) | ↑ Fatty acids |
| ↑ Ketoacid formation | ↑ Ketoacids |
4. Somatostatin (δ cells)
- Suppresses both insulin and glucagon release (paracrine inhibition)
- Has "neuronal" cytology - δ cells send dendrite-like processes onto β cells
- Inhibited by: low blood glucose, certain nutrients
- Also inhibits GI motility and other GI secretions
5. Pancreatic Polypeptide (PP cells, ~5%)
- Stimulates gastric and intestinal enzyme secretion
- Inhibits intestinal motility
- Released after protein meals and fasting
6. Clinical Relevance
Diabetes Mellitus (most important endocrine pancreas disease)
A group of metabolic disorders characterized by hyperglycemia due to defects in insulin secretion, insulin action, or both.
ADA/WHO Diagnostic Criteria (any one, confirmed on separate day):
- Fasting plasma glucose ≥ 126 mg/dL
- Random plasma glucose ≥ 200 mg/dL (with symptoms)
- 2-hour glucose ≥ 200 mg/dL on 75 g OGTT
- HbA1c ≥ 6.5%
Prediabetes: FPG 100-125 mg/dL or HbA1c 5.7-6.4%
| Type 1 DM | Type 2 DM | |
|---|---|---|
| Mechanism | Autoimmune β-cell destruction | Insulin resistance + relative β-cell failure |
| Insulin | Absent | Relative deficiency |
| Prevalence | Minority | Vast majority (>90%) |
| Key feature | Prone to DKA | Prone to hyperosmolar state |
Chronic hyperglycemia causes damage to kidneys (leading cause of ESRD), eyes (leading cause of adult-onset blindness), nerves, and blood vessels. In the US, diabetes affects >37 million people (~11% of population).
Sources:
- Costanzo Physiology, 7th Edition, pp. 444-452
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, pp. 1718-1722
- Robbins & Kumar Basic Pathology (Robbins Pathology), pp. 742-743
This is a shared conversation. Sign in to Orris to start your own chat.