Isolated ldl high risks and how to manage
Reading File
Finding Sources
Finding Sources
Searching PubMed
"LDL cholesterol" AND "cardiovascular risk" AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I have comprehensive information to give a thorough, well-structured answer. Let me compile it now.
Isolated High LDL: Risks and Management
What is "Isolated" High LDL?
Isolated LDL-C elevation means the total cholesterol is high primarily because LDL is elevated, while HDL and triglycerides remain normal. It is the most common form of hypercholesterolemia because most circulating cholesterol is carried in LDL particles. As Fuster and Hurst's The Heart (15th Ed.) states: "Because most cholesterol is carried within LDL particles, isolated hypercholesterolemia most often results from elevated LDL-C."
Causes
Primary (Genetic)
- Familial hypercholesterolemia (FH) - heterozygous or homozygous; due to LDL receptor (LDLR) mutations
- Familial defective ApoB - defective ligand for the LDLR
- Autosomal dominant/recessive hypercholesterolemia - other rare monogenic forms
- Polygenic (nonfamilial) hypercholesterolemia - multiple low-effect variants acting together, aggravated by lifestyle
Secondary (Non-Genetic) - Must Always Be Ruled Out First
| Cause | Mechanism |
|---|---|
| Hypothyroidism | Impairs LDL receptor activity |
| Nephrotic syndrome | Increased hepatic lipoprotein synthesis |
| Obstructive liver disease | Reduced bile acid excretion |
| Anorexia nervosa | Impaired LDL catabolism |
| Drugs: cyclosporine, amiodarone, thiazide diuretics, rosiglitazone | Various - often impaired LDL receptor upregulation |
| High saturated/trans fat diet, physical inactivity | Downregulates LDL receptors |
If a secondary cause is found, treat it first. Residual hypercholesterolemia after treating the secondary cause suggests underlying genetic susceptibility.
- Fuster and Hurst's The Heart, 15th Ed., pp. 387-390
Cardiovascular Risks
High LDL-C is the central driver of atherosclerotic cardiovascular disease (ASCVD):
- Accelerated atherosclerosis - LDL particles deposit in areas of endothelial damage and form atherosclerotic plaques. Premature atherosclerosis is the hallmark consequence of high LDL/cholesterol.
- Myocardial infarction (MI) - A clear linear relationship exists between serum cholesterol and MI risk.
- Stroke and peripheral arterial disease - Elevated LDL raises risk across all vascular territories.
- Global disease burden - Total DALYs attributable to high LDL-C were 98.6 million globally (a 41% increase from 1990), reflecting the enormous population-level impact.
- Polyvascular disease amplification - Patients with CHD in 2-3 vascular territories have dramatically higher event rates (up to 119.5 per 1000 person-years vs. ~40 for single-territory disease).
- Cumulative (lifetime) risk - Given the long-term nature of atherogenesis, even mildly elevated LDL sustained over decades significantly raises lifetime ASCVD risk.
A 2024 meta-analysis of 60 RCTs (PMID: 39126771) confirmed that LDL-C reduction translates into cardiovascular risk reduction in a time-dependent manner - the longer the reduction is maintained, the greater the benefit.
LDL-C Targets by Risk Tier
| Risk Category | LDL-C Target |
|---|---|
| Very high risk (ASCVD + recurrent events, or ASCVD + diabetes/CKD/HF) | < 50 mg/dL (< 1.4 mmol/L) |
| High risk (established ASCVD, or LDL > 190, or diabetes) | < 70 mg/dL (< 1.8 mmol/L) |
| Intermediate risk (10-year ASCVD 7.5-20%) | < 100 mg/dL (< 2.6 mmol/L) |
| Low-moderate risk (primary prevention) | < 130 mg/dL (< 3.4 mmol/L) |
Management
Step 1: Lifestyle and Diet (Always First-Line)
- Dietary changes:
- Reduce saturated and trans fats; replace with mono- and polyunsaturated fats
- Add soluble fiber (oats, legumes, psyllium)
- Consider plant sterols/stanols (if sitosterolemia excluded)
- Reduce high glycemic index foods; replace with complex carbohydrates
- Use Mediterranean diet or DASH diet as framework
- A 2025 Cochrane review (PMID: 40326569) confirmed DASH diet reduces cardiovascular risk in both primary and secondary prevention
- Physical activity: Regular aerobic exercise reduces LDL-C
- Weight loss: Beneficial in overweight patients
- Trial period: Low/moderate risk patients get 3-6 months of lifestyle intervention before starting medication; high-risk patients start drugs concurrently with lifestyle changes.
Step 2: Pharmacotherapy
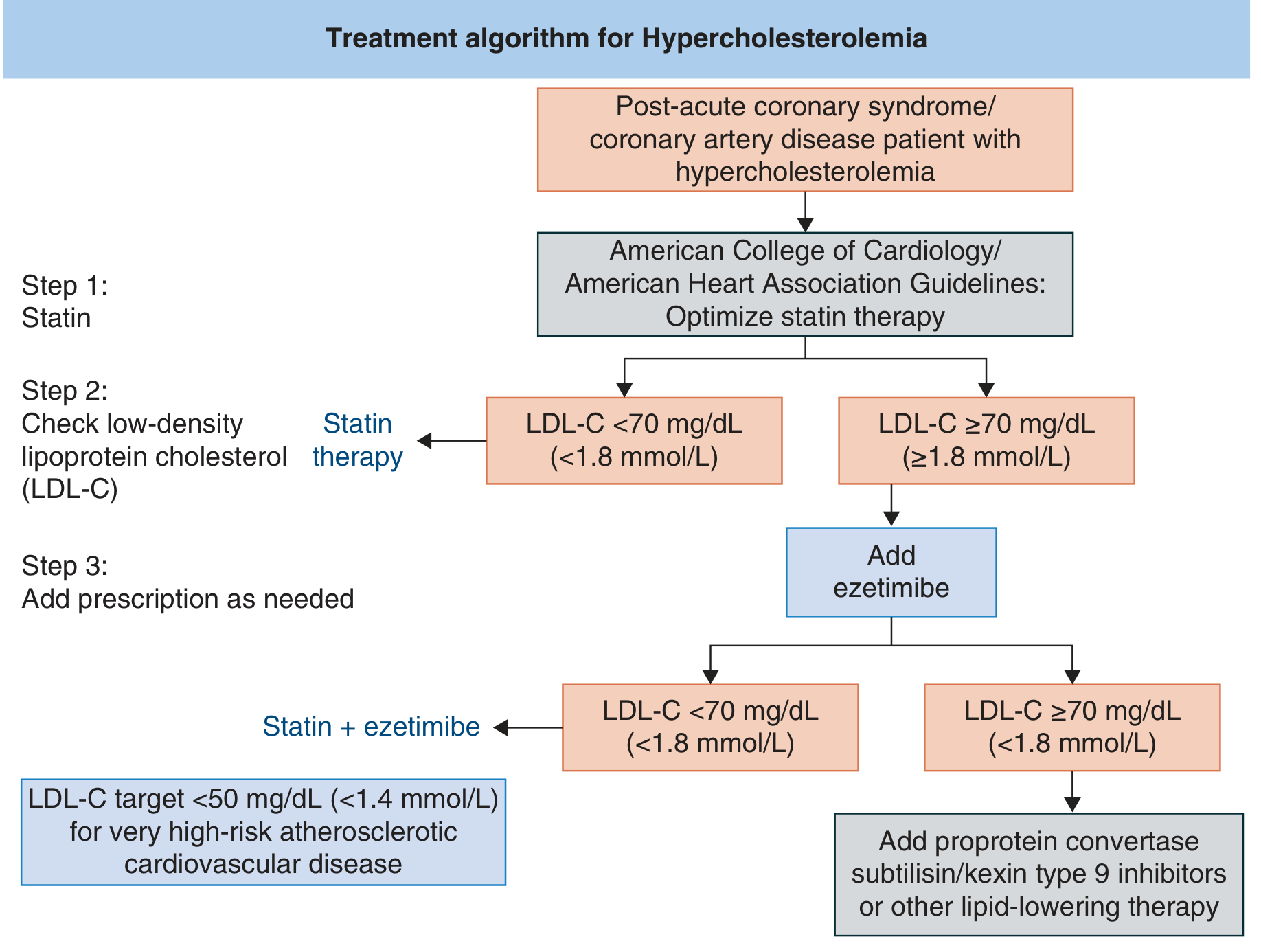
Figure: Clinical algorithm for managing LDL-C (ACC/AHA guidelines) - Fuster and Hurst's The Heart, 15th Ed.
Drug Options with LDL-C Reduction
| Drug | Class | Mechanism | Dose | LDL-C Reduction |
|---|---|---|---|---|
| Atorvastatin | Statin | HMG-CoA reductase inhibition | 10-80 mg/day | 35-50% |
| Rosuvastatin | Statin | HMG-CoA reductase inhibition | 20-80 mg/day | 37-52% |
| Simvastatin | Statin | HMG-CoA reductase inhibition | 5-80 mg/day | 32-46% |
| Ezetimibe | Cholesterol absorption inhibitor | Blocks NPC1L1 transporter | 10 mg/day | 18-25% |
| Evolocumab | PCSK9 inhibitor | Prevents LDL receptor degradation | 140 mg SC q2w or 420 mg SC monthly | 50-70% |
| Alirocumab | PCSK9 inhibitor | Prevents LDL receptor degradation | 75-150 mg SC q2w | 50-70% |
| Cholestyramine | Bile acid sequestrant | Depletes hepatic cholesterol | 4-8 g 1-2x/day | 18-20% |
| Colesevelam | Bile acid sequestrant | Depletes hepatic cholesterol | 625 mg 2-3x/day | 7-18% |
- Fuster and Hurst's The Heart, 15th Ed., Table 10-11
Treatment Algorithm (ACC/AHA approach):
- Step 1 - Start high-intensity statin (atorvastatin 40-80 mg or rosuvastatin 20-40 mg). Check LDL-C response in ~8 weeks.
- If LDL-C still ≥ 70 mg/dL - Add ezetimibe 10 mg/day (adds ~18-25% additional reduction).
- If LDL-C still ≥ 70 mg/dL - Add a PCSK9 inhibitor (evolocumab or alirocumab) - these are the most potent agents, achieving 50-70% additional reduction.
- For very high-risk patients - Target LDL-C < 50 mg/dL.
- Bile acid sequestrants - Useful in statin-intolerant patients or for additive therapy.
- Emerging therapies: Inclisiran (siRNA against PCSK9, given twice yearly SC), bempedoic acid, evinacumab (for homozygous FH).
Special Cases:
- FH (heterozygous): Usually requires statin + ezetimibe combination; many need a PCSK9 inhibitor to reach targets.
- FH (homozygous): Standard of care is lipoprotein apheresis; evinacumab (anti-ANGPTL3) is now approved.
- Statin myopathy: Try alternate-day dosing or switch statin before abandoning the class entirely.
Key Points Summary
-
Isolated high LDL is most often polygenic (lifestyle-aggravated) or FH
-
Always rule out secondary causes before initiating lipid-lowering drugs
-
The primary treatment goal is LDL-C reduction to target, guided by the patient's ASCVD risk tier
-
Statins are the cornerstone; ezetimibe and PCSK9 inhibitors are added if targets are not met
-
Every 1 mmol/L (~39 mg/dL) reduction in LDL-C reduces major cardiovascular events by ~22% (Cholesterol Treatment Trialists' meta-analyses)
-
Lifestyle changes alone rarely achieve guideline targets in FH - early pharmacotherapy is usually needed
-
Fuster and Hurst's The Heart, 15th Ed., Chapter 10 (Hypercholesterolemia)
-
Henry's Clinical Diagnosis and Management by Laboratory Methods, Chapter: Lipids, Lipoproteins, and Disease
This is a shared conversation. Sign in to Orris to start your own chat.