Anatomy of sholder
Reading File
Finding Sources
Searching the Web
shoulder joint anatomy bones muscles ligaments bursae
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is a full, well-structured overview of shoulder anatomy:
Anatomy of the Shoulder
The shoulder is the most mobile joint in the human body, and this mobility comes at the cost of inherent bony stability. It uses 3 bones, 4 joints, and a specialized set of soft tissues (muscles, tendons, ligaments, and bursae) to balance function with support.
1. Bones
Three bones make up the shoulder complex:
- Humerus - the bone of the arm; the rounded head of the humerus forms the "ball" of the ball-and-socket joint
- Scapula - a flat, triangular bone with three bony extensions:
- Glenoid - the shallow socket that articulates with the humeral head
- Acromion - the bony arch that overhangs the joint from above
- Coracoid process - a hook-like projection anteriorly, serving as an attachment point for ligaments and muscles
- Clavicle - the collarbone; connects the shoulder girdle to the axial skeleton via the sternum
Gray's Anatomy for Students - the bones of the shoulder consist of the scapula, clavicle, and proximal end of the humerus.
2. Joints (4 total)
| Joint | Type | Function |
|---|---|---|
| Glenohumeral (GH) | Ball-and-socket | Central axis of shoulder motion; most mobile, least stable joint in the body |
| Acromioclavicular (AC) | Plane/gliding with fibrocartilaginous disc | Suspends and stabilizes the shoulder girdle; rotation contributes to full arm elevation |
| Sternoclavicular (SC) | Double-gliding with articular disc | Only true joint connecting the upper extremity to the axial skeleton; rotates ~30° with shoulder motion |
| Scapulothoracic | Functional (not true synovial) | Every 1° of scapulothoracic motion allows 2° of glenohumeral motion; essential for full arm elevation |
Tintinalli's Emergency Medicine - "The glenohumeral joint is the most mobile and least stable joint in the body."
3. Stabilizers of the Glenohumeral Joint
Stability is provided by three systems:
a) Glenoid Labrum (Static)
A fibrocartilaginous ring that encircles the rim of the glenoid cavity. It deepens the shallow socket by 50% and acts as a bumper to resist translation. It also anchors the glenohumeral ligaments.
- Anatomic variants: sublabral foramen (anterosuperior) and the Buford complex (absent anterosuperior labrum + cordlike middle GHL)
b) Glenohumeral Ligaments (Static)
Three ligaments reinforce the joint capsule. The capsule itself attaches from the anatomical neck of the humerus to the glenoid rim (humeral head: glenoid surface area ratio is 4:1, contributing to hypermobility):
| Ligament | Function |
|---|---|
| Superior GHL | Restrains external rotation and inferior translation with arm at side |
| Middle GHL (absent in up to 30% of people) | Restrains anterior translation with arm abducted to 45° |
| Inferior GHL - anterior band | Restrains anterior/inferior translation at 90° abduction + external rotation (position of apprehension) |
| Inferior GHL - posterior band | Restrains posterior/inferior translation at 90° abduction + internal rotation |
| Coracohumeral ligament | Restrains inferior translation and external rotation with arm adducted |
Miller's Review of Orthopaedics - table of glenohumeral stabilizers
c) Rotator Cuff Muscles (Dynamic)
Four muscles that all originate on the scapula and insert on the proximal humerus, providing 30-50% of power in abduction and 90% of power in external rotation:
4. Rotator Cuff - "SITS"
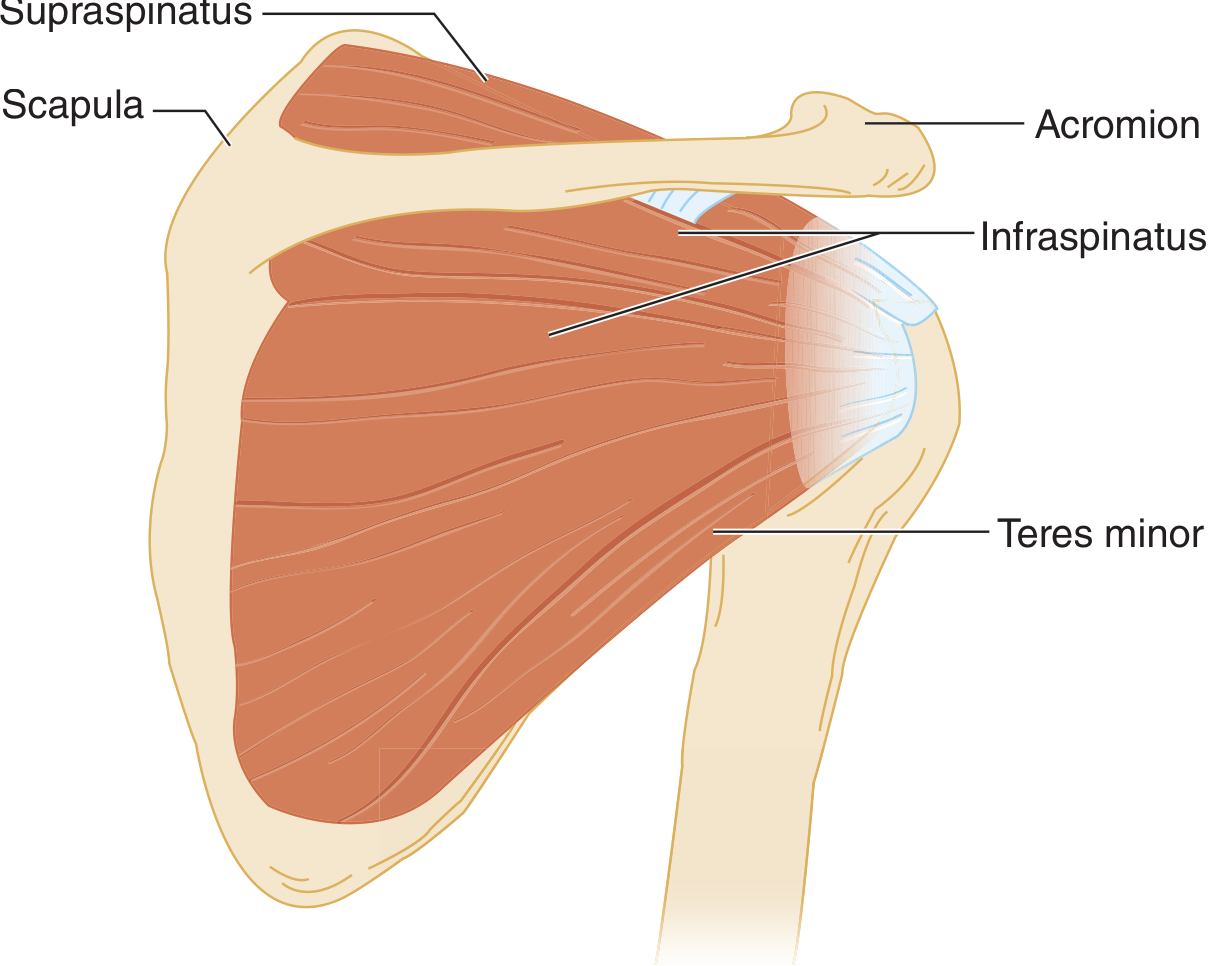
Posterior view of the shoulder - rotator cuff muscles (from Tintinalli's Emergency Medicine)
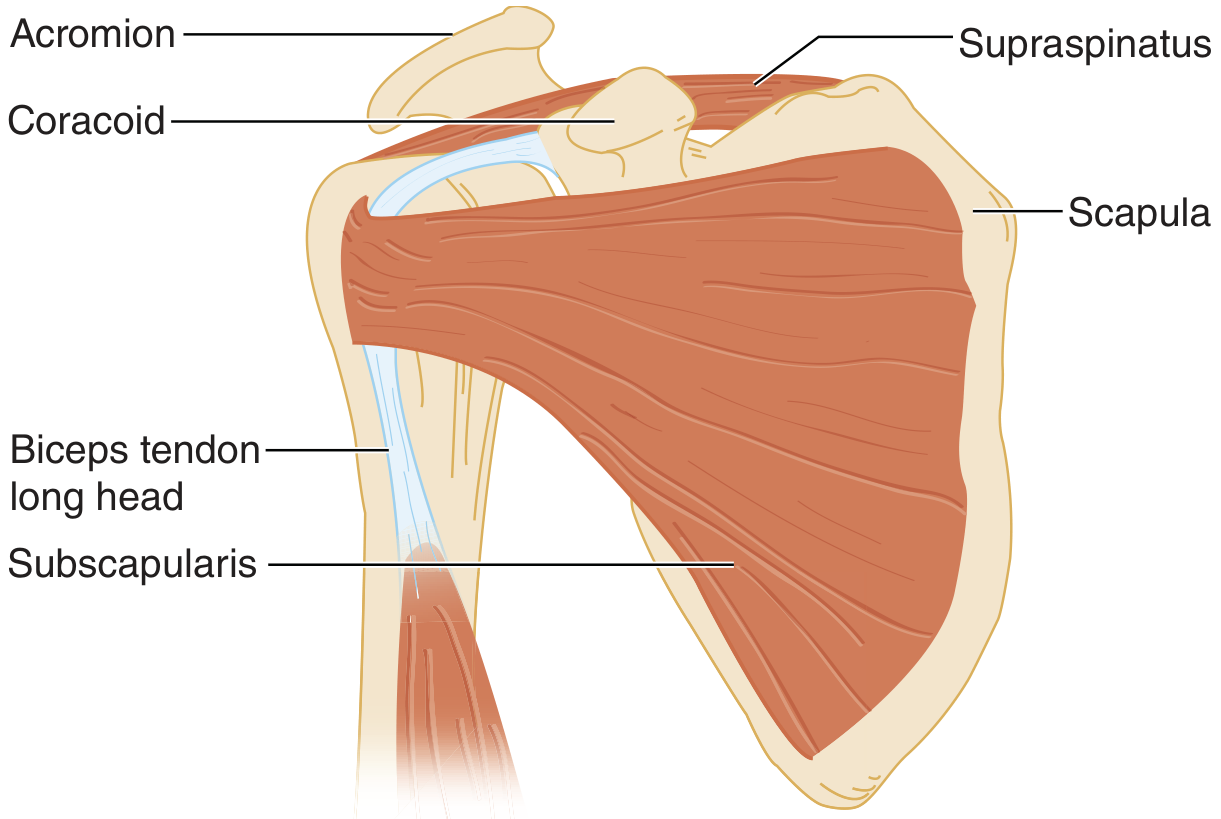
Anterior view - subscapularis and long head of biceps tendon (from Tintinalli's Emergency Medicine)
| Muscle | Origin | Insertion | Action |
|---|---|---|---|
| Supraspinatus | Posterior/superior scapula (supraspinous fossa) | Greater tuberosity (superior facet) | Initiates abduction; keeps humeral head centered against deltoid pull |
| Infraspinatus | Posterior scapula below scapular spine | Greater tuberosity (middle facet) | External rotation |
| Teres minor | Lateral border of scapula (below infraspinatus) | Greater tuberosity (inferior facet) | External rotation (works with infraspinatus) |
| Subscapularis | Anterior surface of scapula (subscapular fossa) | Lesser tuberosity | Internal rotation; only anterior rotator cuff muscle |
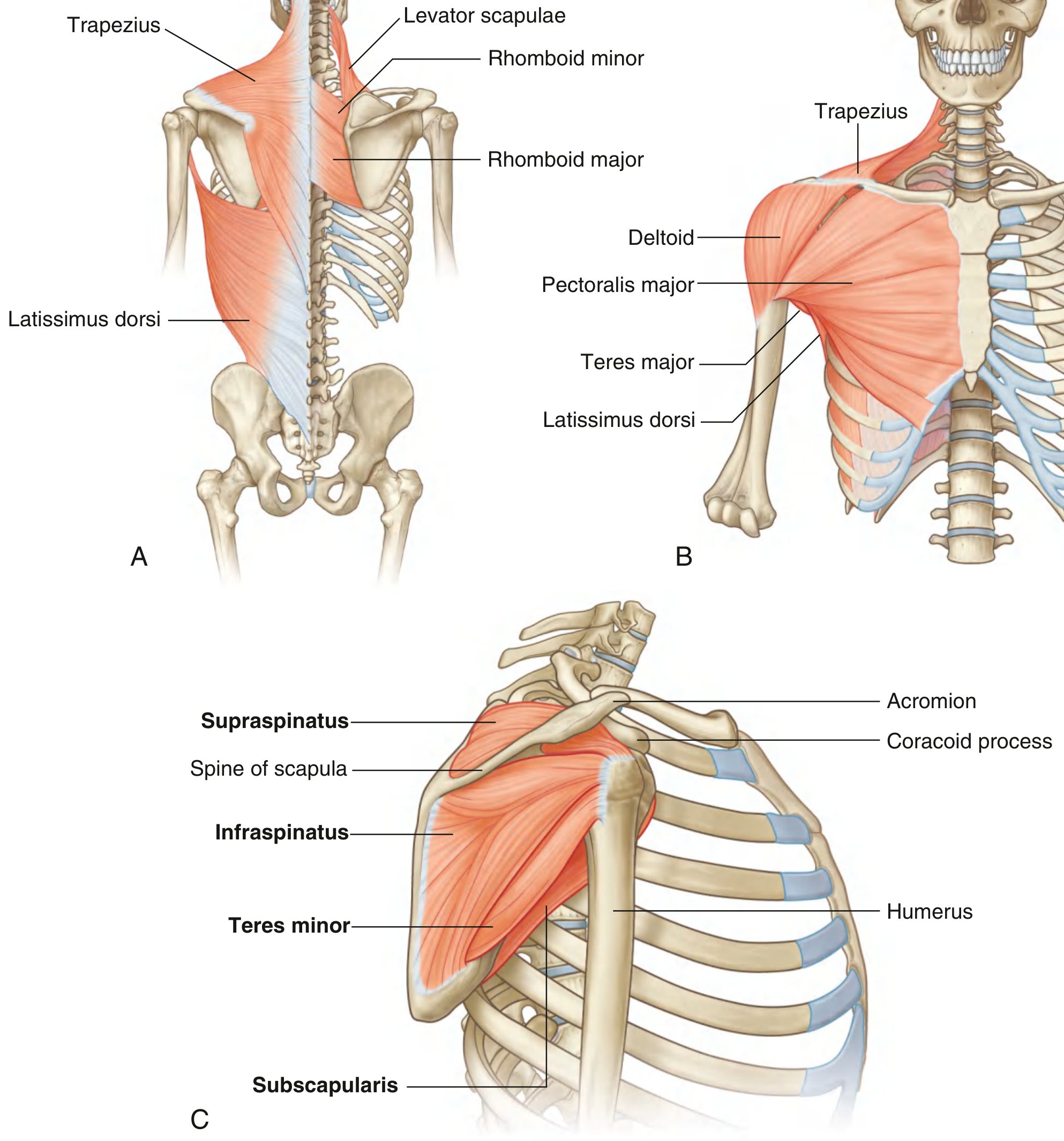
All four rotator cuff muscles with bony context - Gray's Anatomy for Students
5. Other Key Muscles
- Deltoid - the powerful superficial muscle that drapes the shoulder and forms its contour; primary elevator of the arm along with pectoralis major
- Pectoralis major - anterior chest muscle; adduction, internal rotation, flexion
- Trapezius - moves and stabilizes the scapula
- Serratus anterior - protracts and rotates the scapula (winging if paralyzed)
- Latissimus dorsi - extension, adduction, and internal rotation of the arm
- Long head of biceps tendon - although not part of the rotator cuff, it travels through the bicipital groove (between greater and lesser tuberosities), passes through the rotator interval, and inserts on the superior labrum; during arm elevation, it depresses the humeral head to keep it centered in the glenoid
6. Bursae
There are 8 bursae in the shoulder, but only one is clinically significant:
- Subacromial bursa (also called subdeltoid bursa) - extra-articular; its roof adheres to the undersurface of the deltoid, and its floor to the rotator cuff. Lubricated by synovial fluid and surrounded by peribursal fat. It allows frictionless gliding of the rotator cuff tendons under the acromion.
7. Coracoacromial Arch
Formed by:
- Coracoid process (posteriorly)
- Acromion (anteriorly)
- Coracoacromial ligament (forms the anterior roof)
The rotator cuff tendons, long head of biceps, and subacromial bursa all function within this narrow arch. This is the site of subacromial impingement when there is overhead arm use.
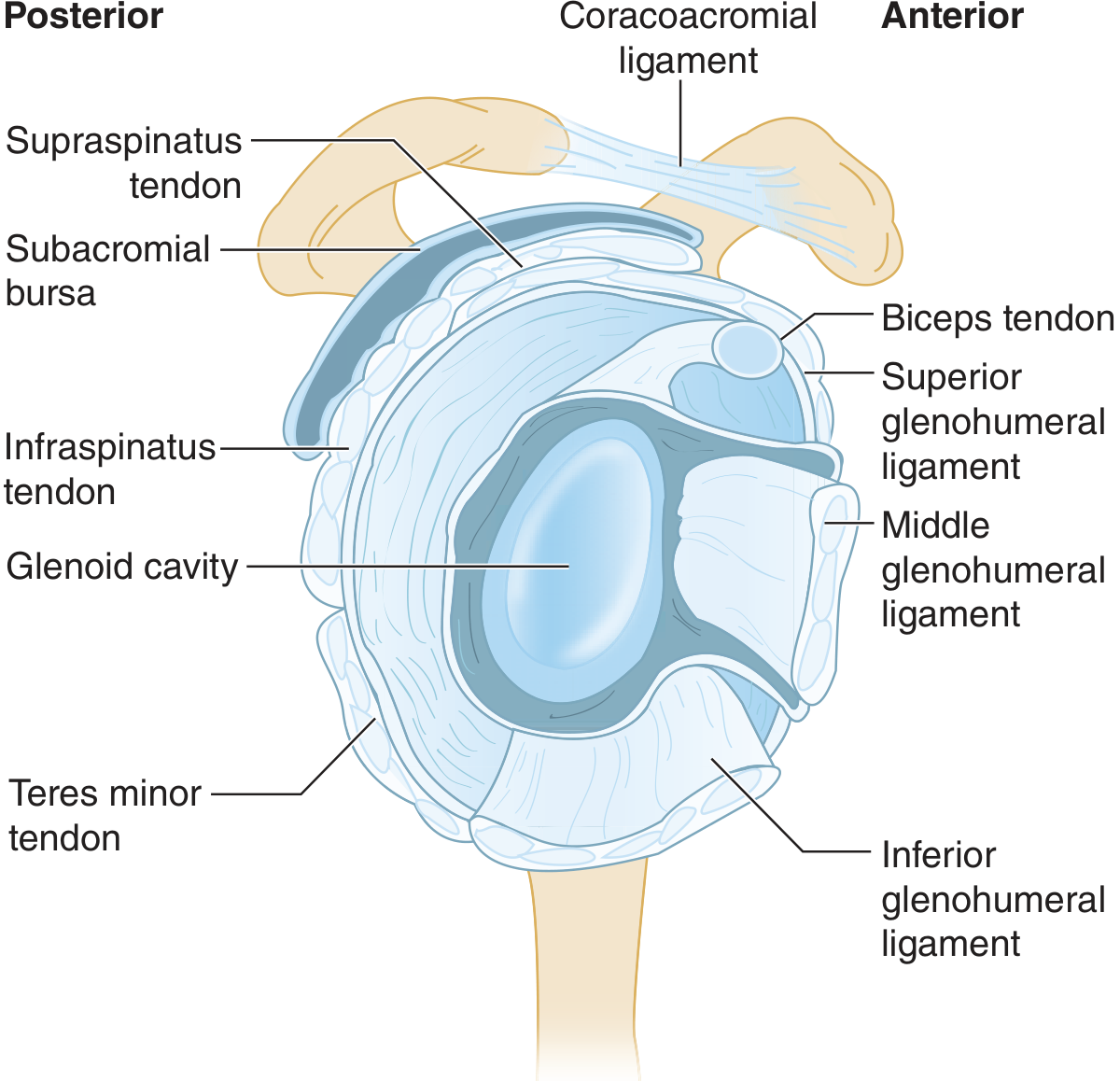
Lateral view of the glenohumeral joint showing ligaments, subacromial bursa, and the coracoacromial arch (from Tintinalli's Emergency Medicine)
8. Nerve Supply
- Axillary nerve (C5, C6) - supplies the deltoid and teres minor; wraps around the surgical neck of the humerus (at risk in proximal humerus fractures and shoulder dislocations)
- Suprascapular nerve (C5, C6) - supplies supraspinatus and infraspinatus
- Subscapular nerves (C5, C6) - upper and lower subscapular nerves supply subscapularis; the lower also supplies teres major
- Musculocutaneous nerve (C5-C7) - supplies the anterior arm (biceps, coracobrachialis, brachialis)
- Long thoracic nerve (C5-C7) - supplies serratus anterior (injury causes winging of the scapula)
9. Blood Supply
- Anterior and posterior circumflex humeral arteries - branches of the axillary artery; anastomose around the surgical neck of the humerus
- Suprascapular artery and circumflex scapular artery - supply the posterior musculature
Summary: Key Clinical Points
| Feature | Relevance |
|---|---|
| Most mobile joint in the body | High dislocation risk (anterior dislocation most common, ~95%) |
| Supraspinatus passes under acromion | Most vulnerable to impingement and tears (watershed zone of poor vascularity) |
| Axillary nerve wraps surgical neck | At risk with anterior shoulder dislocation and proximal humerus fractures |
| Glenoid labrum acts as a bumper | Bankart lesion (anteroinferior labral tear) is the "essential lesion" of anterior instability |
| Scapulothoracic rhythm | 2:1 ratio - for every 3° of shoulder abduction, 2° is GH motion and 1° is scapulothoracic rotation |
Sources: Tintinalli's Emergency Medicine (9th ed.), Gray's Anatomy for Students, Miller's Review of Orthopaedics (9th ed.), THIEME Atlas of General Anatomy and Musculoskeletal System
This is a shared conversation. Sign in to Orris to start your own chat.