Explain heart sound with images as I'm final yr MBBS student
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have all the content and images needed to write a comprehensive, well-illustrated answer. Let me compile the full explanation.
Heart Sounds - A Complete Guide for Final Year MBBS
Overview: The Cardiac Cycle and Sound Generation
Heart sounds are vibrations produced by valve closures, turbulent blood flow, and vibration of cardiac structures. They are heard by auscultation and can be recorded on a phonocardiogram (PCG). The classic description is "lub-DUB" - the "lub" is S1 and the "DUP" is S2.
Auscultation Areas
Fig. 23.2 (Guyton & Hall) - Chest areas for valve auscultation:
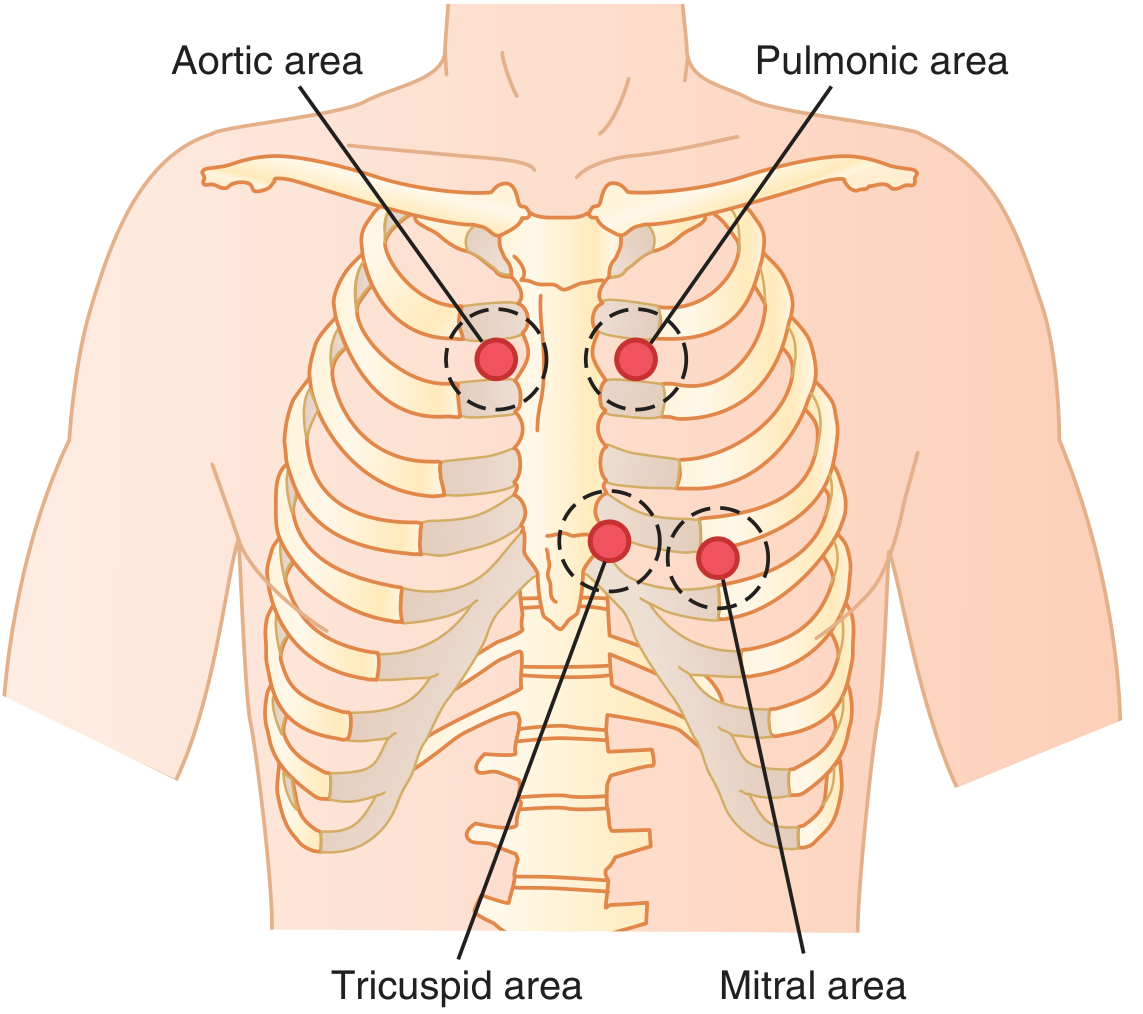
Fig. 2-15 (Fuster's Heart, 15th ed) - Five classic auscultation areas:
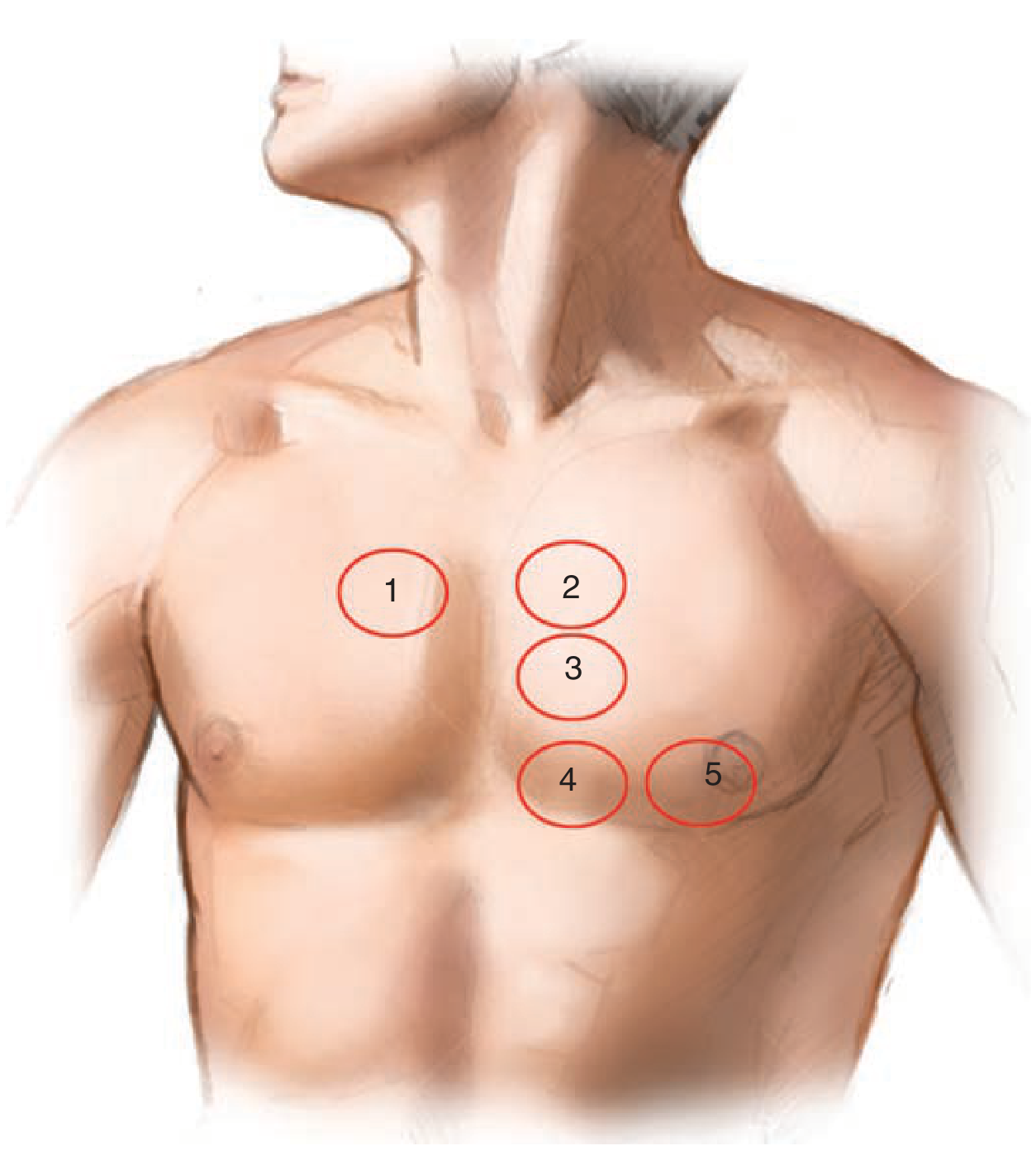
| Area | Location | Best for |
|---|---|---|
| Aortic (1) | 2nd ICS, right parasternal | A2, aortic murmurs |
| Pulmonic (2) | 2nd ICS, left parasternal | P2, pulmonic murmurs |
| Accessory Aortic / Erb's (3) | 3rd ICS, left parasternal | AR murmur, additional aortic sounds |
| Tricuspid (4) | 5th ICS, left parasternal / LLSB | Tricuspid murmurs |
| Mitral (5) | Apex (apical impulse) | S1, S3, S4, mitral murmurs |
Note: The listening areas are NOT directly over the valves. Aortic and pulmonic areas are upstream because sound travels up the great vessels.
Frequency Range of Heart Sounds
Fig. 23.1 (Guyton & Hall) - Audibility of heart sounds vs. murmurs:
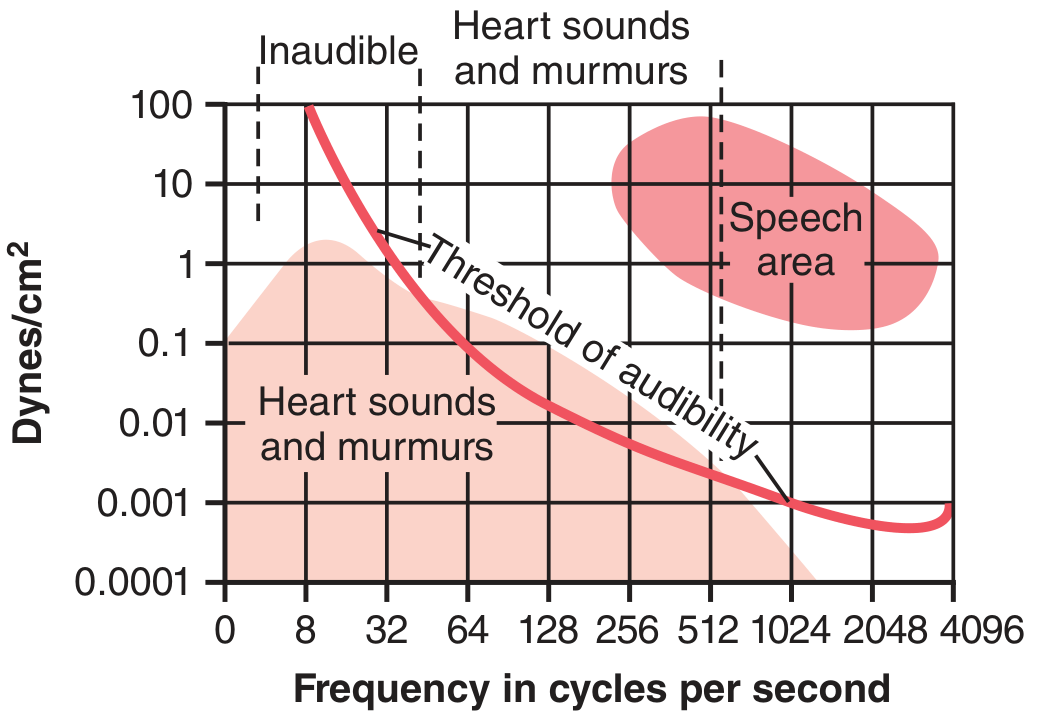
The audible range is 40-520 Hz. Much of the heart sound energy (especially S3, S4) falls below this threshold, which is why:
- S1 and S2 are heard with the diaphragm (high frequency)
- S3 and S4 are heard with the bell (low frequency, applied gently)
S1 - First Heart Sound ("LUB")
Mechanism: Closure of the mitral (M1) and tricuspid (T1) valves at the onset of ventricular systole.
- M1 closes first (left-sided pressure rises first), then T1
- In most patients, they are heard as a single sound
- Duration: ~0.14 seconds
- Best heard: Apex (mitral area)
Splitting of S1: Normally M1 and T1 are very close together. Physiologic splitting can be heard at the LLSB. Wider splitting occurs in RBBB and Ebstein's anomaly (large sail-like T1).
Intensity of S1 - "Loud vs Soft"
| Loud S1 | Soft S1 |
|---|---|
| Short PR interval (tachycardia, pre-excitation) | Prolonged PR interval (1st degree heart block) |
| Mitral stenosis with pliable leaflets | Mitral stenosis with calcified/immobile leaflets |
| Hyperdynamic circulation (fever, anemia, pregnancy) | Poor LV systolic function (cardiomyopathy) |
| Atrial fibrillation (variable - beats with short RR are loud) | Severe MR (early valve closure) |
S2 - Second Heart Sound ("DUB")
Mechanism: Closure of the aortic (A2) and pulmonary (P2) valves at the end of systole.
- A2 closes first (left-sided pressure is higher)
- Duration: ~0.11 seconds (shorter than S1 - semilunar valves are tauter)
- Higher pitch than S1
- Best heard: 2nd ICS left sternal border (pulmonic area)
Splitting of S2 - the most clinically important physical sign in cardiology:
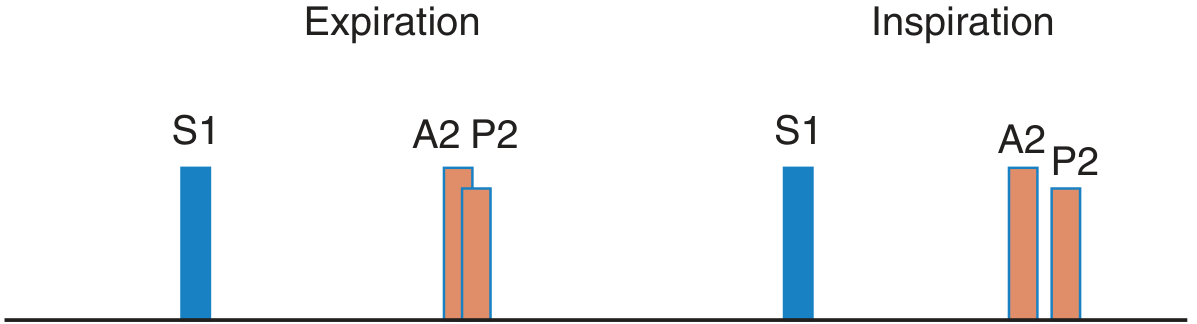
Fig. 2-17 (Fuster's Heart) - Physiologic splitting of S2:
S2 Splitting - Summary Table
| Type | On Expiration | On Inspiration | Causes |
|---|---|---|---|
| Physiologic (normal) | Single (A2=P2) | Split (A2 then P2) | Normal - increased RV filling delays P2 |
| Wide splitting | Split | Wider split | RBBB, pulmonary hypertension, severe PS |
| Fixed splitting | Split | Split (no change) | ASD (ostium secundum) |
| Paradoxical splitting | Split (P2 then A2!) | Single | LBBB, severe AS, HCM, RV pacing |
| Single S2 | Single | Single | Pulmonary hypertension (P2 inaudible), severe AS, one semilunar valve (atresia) |
Key rule for paradoxical splitting: A2 is delayed, so on inspiration when P2 moves later, the two sounds merge rather than separate - the opposite of normal.
S3 - Third Heart Sound (Ventricular Gallop)
Mechanism: Occurs in early diastole (rapid filling phase), when blood rushes from the atrium into a distended ventricle and causes the ventricular walls to vibrate.
- Timing: After S2, at the beginning of the middle third of diastole
- Very low frequency - heard with bell at the apex
- Rhythm sounds like: "Ken-tuck-y" (lub-DUB-ba)
| Context | Significance |
|---|---|
| Children, young adults, athletes, pregnancy | Physiologically normal |
| Adults >40 years | Pathologic - indicates systolic heart failure / volume overload |
| Classic causes | Dilated cardiomyopathy, severe MR, large VSD |
S4 - Fourth Heart Sound (Atrial Gallop / Presystolic Gallop)
Mechanism: Occurs in late diastole (atrial kick), when the atrium contracts forcefully to fill a stiff, non-compliant ventricle.
- Timing: Just before S1
- Very low frequency (~20 Hz) - heard with bell at apex
- Rhythm sounds like: "Ten-nes-see" (da-lub-DUB)
- Always pathologic in adults (requires an atrial contraction, so it is absent in AF)
| Cause | Example |
|---|---|
| Reduced LV compliance | LV hypertrophy (hypertension, AS, HCM) |
| Myocardial ischemia/infarction | Acute MI |
| Severe right ventricular overload | PS, pulmonary hypertension |
Pressure Tracings Correlated with Heart Sounds (S1-S4)
Fig. 2-16 (Fuster's Heart, 15th ed) - Heart sounds correlated with LV pressure:
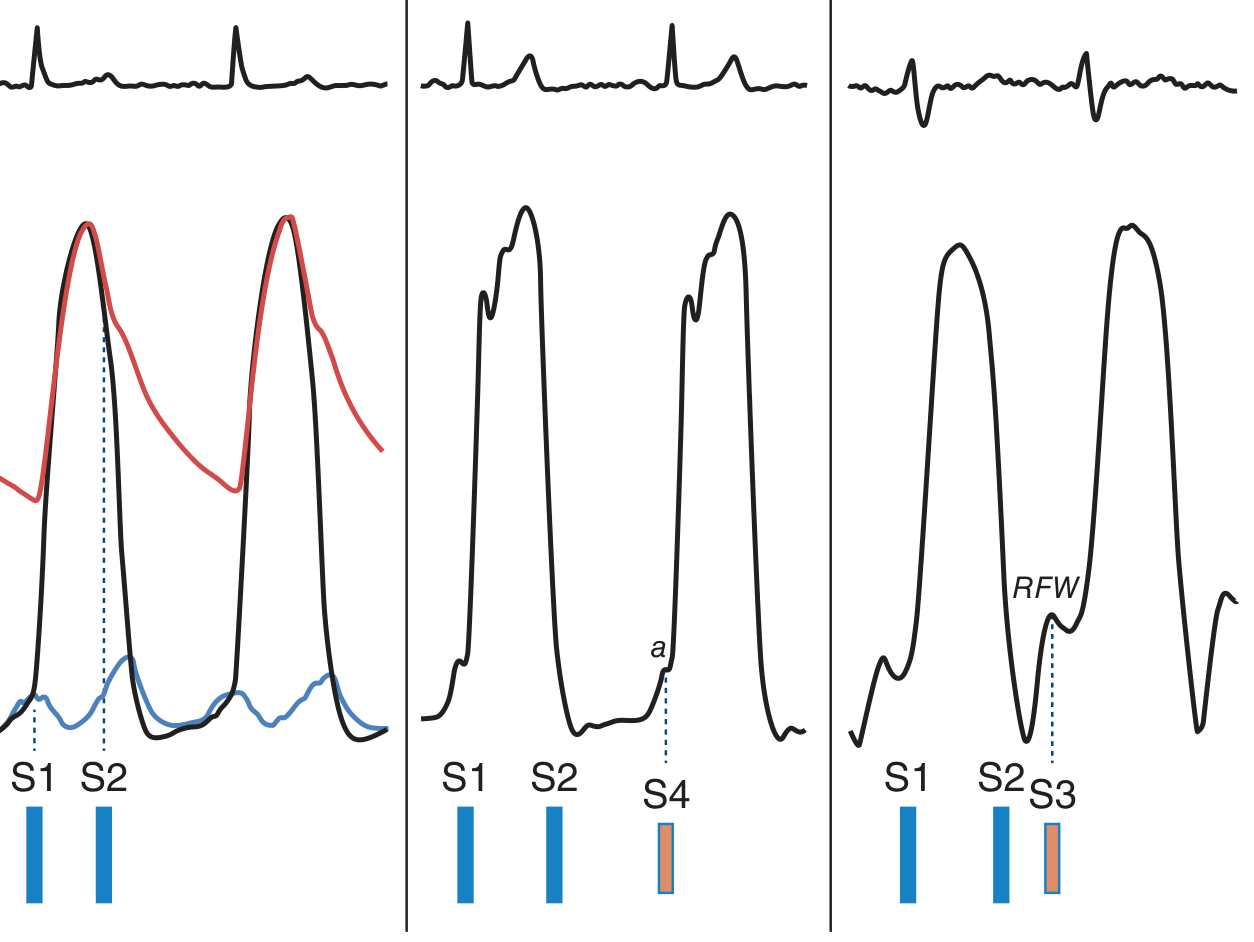
- Left panel: Normal S1 (LV pressure exceeds LA pressure = MV closes) and S2 (LV pressure drops below aortic pressure = AV closes)
- Middle panel: S4 in hypertrophic cardiomyopathy - prominent "a" wave from forceful atrial contraction into stiff LV
- Right panel: S3 in restrictive cardiomyopathy - prominent rapid filling wave (RFW) in early diastole
Phonocardiogram: Normal and Abnormal Patterns
Fig. 23.3 (Guyton & Hall) - Phonocardiograms in various conditions:
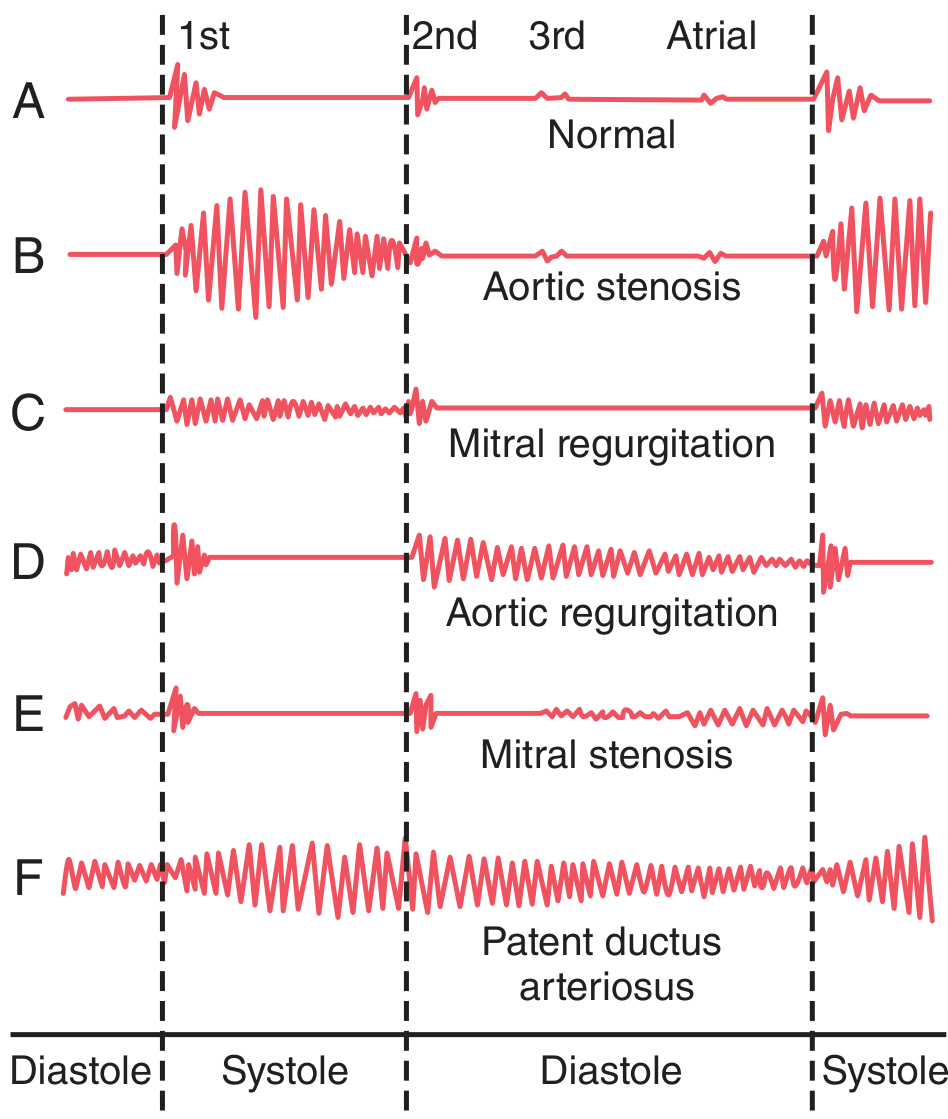
| Condition | Pattern | What you see/hear |
|---|---|---|
| Normal (A) | S1, S2, soft S3, soft atrial sound | Normal intervals |
| Aortic stenosis (B) | Loud systolic ejection murmur | Spindle-shaped (diamond) systolic vibrations |
| Mitral regurgitation (C) | Pansystolic murmur | Uniform systolic vibrations from S1 to S2 |
| Aortic regurgitation (D) | Diastolic decrescendo | Vibrations starting at S2 into diastole |
| Mitral stenosis (E) | Mid-diastolic rumble + opening snap | Opening snap after S2, then rumble |
| PDA (F) | Continuous machinery murmur | Vibrations in both systole and diastole |
Added Sounds - Systolic and Diastolic
Fig. 39-5 (Goldman-Cecil Medicine) - Timing of added heart sounds:
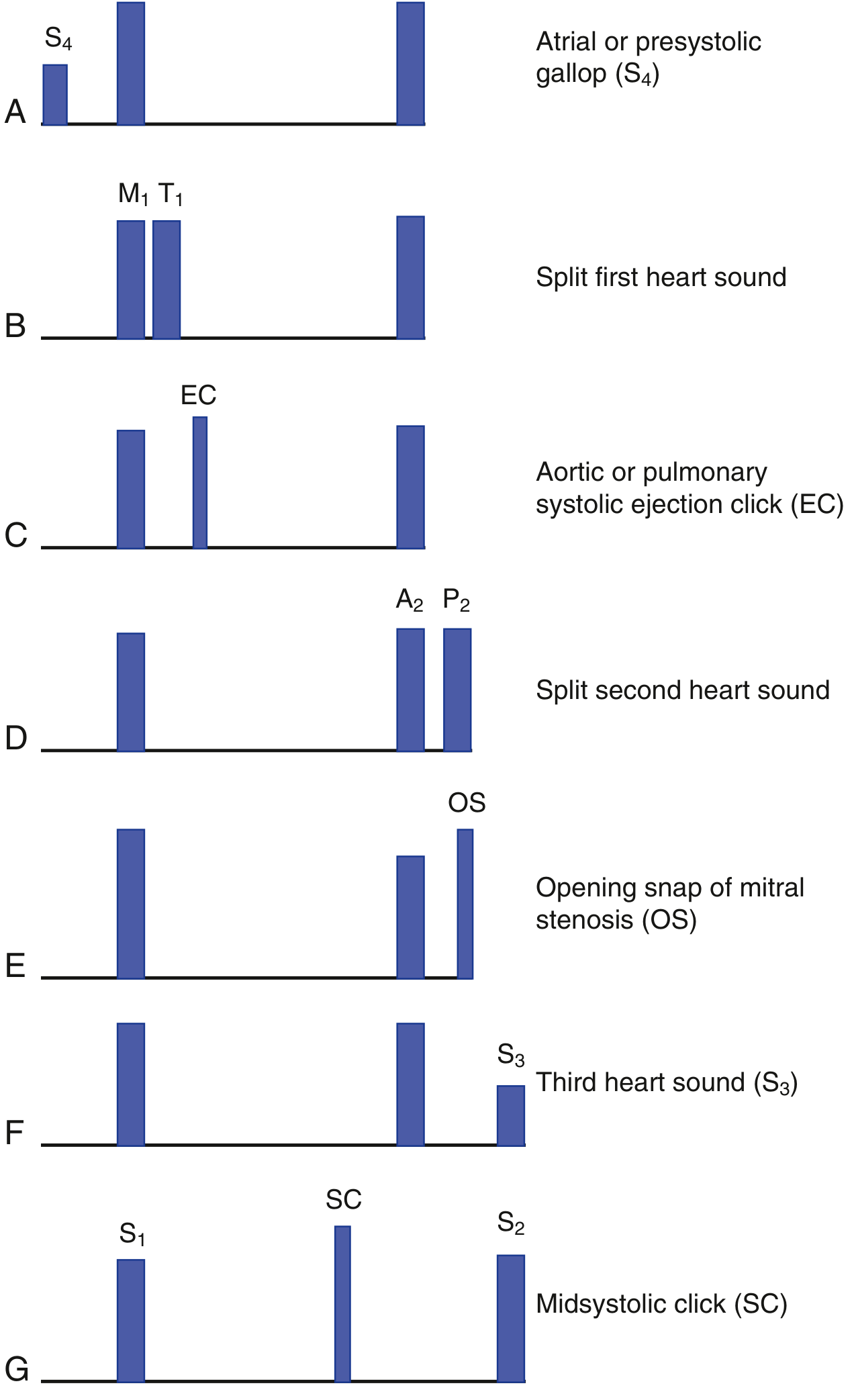
Systolic Added Sounds
| Sound | Timing | Cause | Where Heard |
|---|---|---|---|
| Ejection Click (EC) | Early systole (just after S1) | Stenosis of semilunar valves (AS, PS); dilated great arteries | Aortic/pulmonic areas |
| Midsystolic Click (SC) | Mid-systole | Mitral valve prolapse | Apex |
- In mitral valve prolapse: click moves earlier with standing/Valsalva (less LV volume); moves later with squatting/leg raise (more LV volume)
Diastolic Added Sounds
| Sound | Timing | Cause |
|---|---|---|
| Opening Snap (OS) | Early diastole (after S2) | Mitral stenosis (pliable leaflets snapping open) |
| S3 gallop | Early-mid diastole | Volume overload / systolic HF |
| Pericardial knock | Early diastole (like S3) | Constrictive pericarditis (abrupt cessation of ventricular filling) |
| Tumor plop | Mid-diastole | Left atrial myxoma |
S2-OS interval in mitral stenosis: The shorter the interval, the more severe the MS (higher LA pressure forces MV to open earlier).
Gallop Rhythms - Quick Summary
| Gallop | Sounds | Rhythm Word | Timing | Significance |
|---|---|---|---|---|
| Ventricular (S3) | S1 + S2 + S3 | "Ken-tuck-y" | S3 in early diastole | Systolic HF, volume overload |
| Atrial (S4) | S4 + S1 + S2 | "Ten-nes-see" | S4 in late diastole | Diastolic dysfunction, stiff ventricle |
| Summation gallop | S3 + S4 fused | Single loud sound | In tachycardia diastole shortens | Severe HF |
Murmur Grading (Levine Scale)
| Grade | Description |
|---|---|
| I | Barely audible, requires concentration |
| II | Soft but immediately audible |
| III | Moderately loud; no thrill |
| IV | Loud; associated with a thrill |
| V | Very loud; audible with stethoscope barely touching chest; thrill present |
| VI | Audible with stethoscope off the chest |
Grades I-III: no thrill. Grades IV-VI: thrill present. For clinical reports, write as a fraction: e.g., "2/6 systolic murmur."
Quick Reference: Summary Table
| Sound | Timing | Valve(s) | Auscultation Site | Clinical Significance |
|---|---|---|---|---|
| S1 | Onset of systole | Mitral + Tricuspid (closure) | Apex | Loud in MS (pliable), short PR; Soft in calcified MS, 1st deg HB |
| S2 | End of systole | Aortic + Pulmonary (closure) | LUSB (2nd ICS L) | Splitting abnormalities indicate cardiac pathology |
| S3 | Early diastole | - | Apex (bell) | Normal in young; pathologic HF/volume overload in adults |
| S4 | Late diastole (presystolic) | - | Apex (bell) | Always pathologic; reduced ventricular compliance |
| Ejection Click | Early systole | Semilunar | Base | AS, PS, dilated great vessels |
| Midsystolic Click | Mid-systole | Mitral (prolapse) | Apex | MVP |
| Opening Snap | Early diastole | Mitral (stenosis) | LLSB/apex | MS; shorter S2-OS = more severe |
Sources: Guyton and Hall Textbook of Medical Physiology; Fuster and Hurst's The Heart, 15th Edition; Goldman-Cecil Medicine; The Harriet Lane Handbook, 23rd Edition
This is a shared conversation. Sign in to Orris to start your own chat.