Hemangioma of left oral mucosa
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
hemangioma oral mucosa treatment
Reading File
Searching PubMed
oral hemangioma vascular malformation management
Loading Image
Searching the Web
hemangioma oral mucosa clinical features treatment 2024
I now have comprehensive information to provide a thorough answer. Let me compile everything.
Hemangioma of the Left Oral Mucosa
Definition & Overview
A hemangioma of the oral mucosa is a benign vascular neoplasm characterized by abnormal proliferation of blood vessels lined by endothelial cells. It is the most common benign vascular tumor of the head and neck region. Oral cavity hemangiomas account for approximately 14% of all hemangiomas of the head and neck.
- Cummings Otolaryngology Head and Neck Surgery, Ch. 90
Classification
Hemangiomas are classified under the ISSVA (International Society for the Study of Vascular Anomalies) framework, distinguishing them from true vascular malformations:
| Type | Features |
|---|---|
| Infantile hemangioma | Absent/small at birth, rapid proliferative phase (age 1-6 months), then involutes over 1-12 years |
| Congenital hemangioma | Fully formed at birth; includes RICH (rapidly involuting), NICH (non-involuting), and PICH (partially involuting) |
| Capillary hemangioma | Small, thin-walled capillaries; common superficial type |
| Cavernous hemangioma | Large, dilated vascular channels; deeper, more common in adults |
Epidemiology & Site Predilection
- Infantile hemangiomas occur in up to 10% of all births; female predominance
- The lip is the most frequent site of hemangioma in the oral cavity, followed by tongue, buccal mucosa, and floor of mouth
- Usually present at birth or become evident in the first few weeks/months of life; can occasionally become evident later
Associated Syndromes
Oral/head-neck hemangiomas may be associated with:
- Sturge-Weber-Dimitri syndrome (facial port-wine stain, leptomeningeal angiomatosis, glaucoma)
- Von Hippel-Lindau syndrome (hemangioblastomas + visceral lesions)
- Multiple cutaneous lesions are not uncommon alongside parotid/salivary gland hemangiomas
Clinical Features
| Feature | Description |
|---|---|
| Appearance | Soft, painless mass; red or blue in color (blanches with pressure/diascopy) |
| Size | Typically < 2 cm; can become extensive, involving the tongue or oropharynx |
| Consistency | Soft, compressible |
| Symptoms | Usually asymptomatic; large lesions can cause functional problems (speech, swallowing, aesthetics) |
| Behavior | Tend to spontaneously regress over years; involution may be incomplete; fibrosis can develop |
Histopathology
Microscopically, hemangiomas comprise capillaries lined by proliferative endothelial cells with uniform vessel size. Mitoses are frequent but are not indicators of malignant behavior.
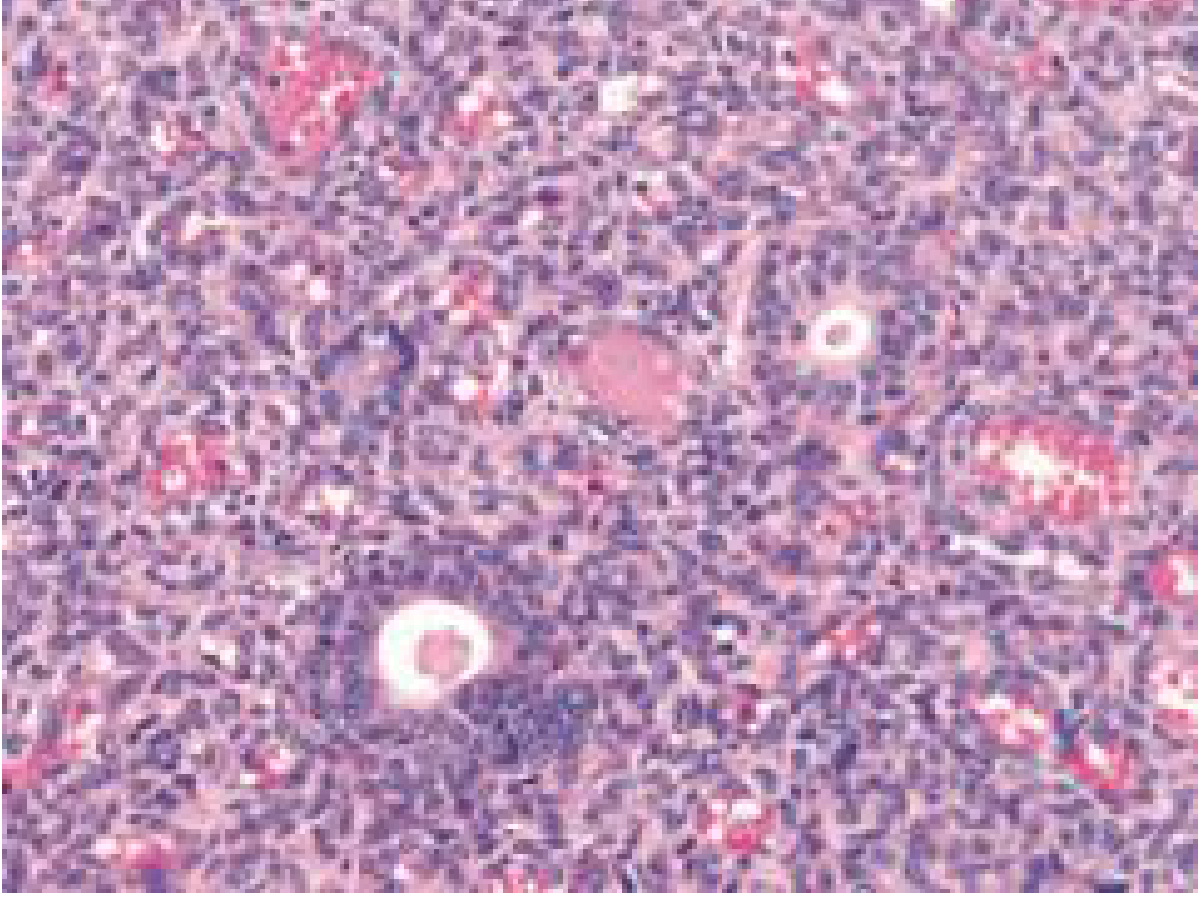
Histology: Juvenile lobular hemangioma showing dense vascular proliferation with proliferative endothelial cells - Cummings Otolaryngology
Diagnosis
- Clinical diagnosis in most straightforward cases (blanching on pressure is pathognomonic)
- MRI is the imaging modality of choice to determine extent - important before treatment, as extensive spread may not be evident clinically
- Biopsy if diagnosis is in doubt (risk of bleeding; use with caution)
- Distinguish from vascular malformations (low-flow vs. high-flow), pyogenic granuloma, and lymphangioma
Treatment
The treatment approach depends on lesion behavior (proliferating vs. involuting) and functional impact:
Conservative / Observation
- The majority will involute spontaneously over time; watchful waiting is appropriate for small, asymptomatic lesions
- Indicated for non-problematic infantile hemangiomas in proliferative or involuting phases
Medical Therapy
| Agent | Notes |
|---|---|
| Propranolol (beta-blocker) | First-line for infantile hemangiomas; dose 2-3 mg/kg/day in 3 divided doses; mechanism - inhibits proangiogenic factor secretion and endothelial growth; rapid and excellent results |
| Corticosteroids (local and systemic) | Older mainstay; both local injection and systemic use described |
| Interferon | Used for refractory cases; systemic side effects limit use |
| Vincristine | Used in refractory/large lesions |
Surgical / Invasive Therapy
| Modality | Notes |
|---|---|
| Conservative surgical excision | For lesions limiting oral form and function; recurrence/persistence is not unusual |
| Sclerotherapy (intralesional sclerosing agents) | Effective for localized lesions; agents include sodium tetradecyl sulfate, bleomycin |
| Laser therapy | CO2, Nd:YAG, KTP lasers used; good hemostasis; useful for mucosal lesions |
| Embolization | For high-flow or extensive lesions; often adjunctive |
| Radiation | Rarely used; adjunctive in refractory cases |
For adults with cavernous hemangiomas (the common adult type in salivary glands), surgical excision is the primary treatment.
Key Points for Left Oral Mucosa Hemangioma
- Most are benign with favorable natural history - spontaneous involution is common
- Lip is the most common site, but buccal mucosa, tongue, and floor of mouth are also frequently involved
- Get MRI to define extent before any intervention
- For infantile/pediatric: propranolol is now first-line medical therapy
- Surgical excision is reserved for lesions that are functionally limiting or fail to involute
- Recurrence after excision is known - counsel the patient
- Always differentiate from vascular malformation (malformations do not involute, require different management)
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Ch. 90 (Oral Cavity Tumors) and Ch. 84 (Salivary Gland Tumors)
- Medical management of vascular anomalies - J Oral Pathol Med 2022 (PMID 35668029)
- StatPearls: Oral Hemangiomas - Lyssy et al., 2023
This is a shared conversation. Sign in to Orris to start your own chat.