Thigh muscles anatomy with diagram
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have excellent diagrams and detailed textbook content. Let me compile the comprehensive answer.
Thigh Muscles Anatomy
The thigh is divided into three compartments by fascial septa, each containing a distinct muscle group with its own nerve supply and function.
Diagrams
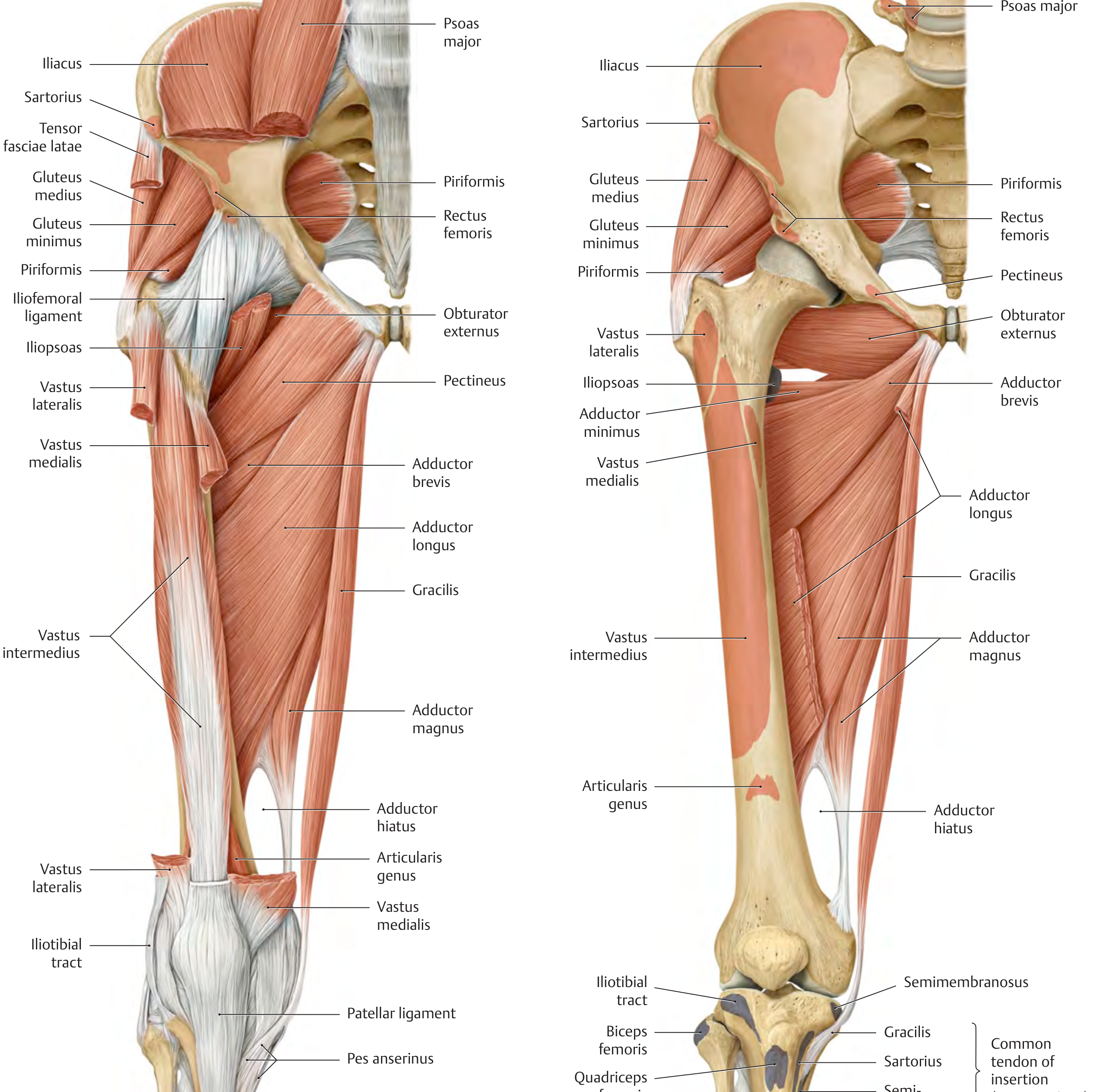
Anterior & Medial View - All Thigh Muscle Groups
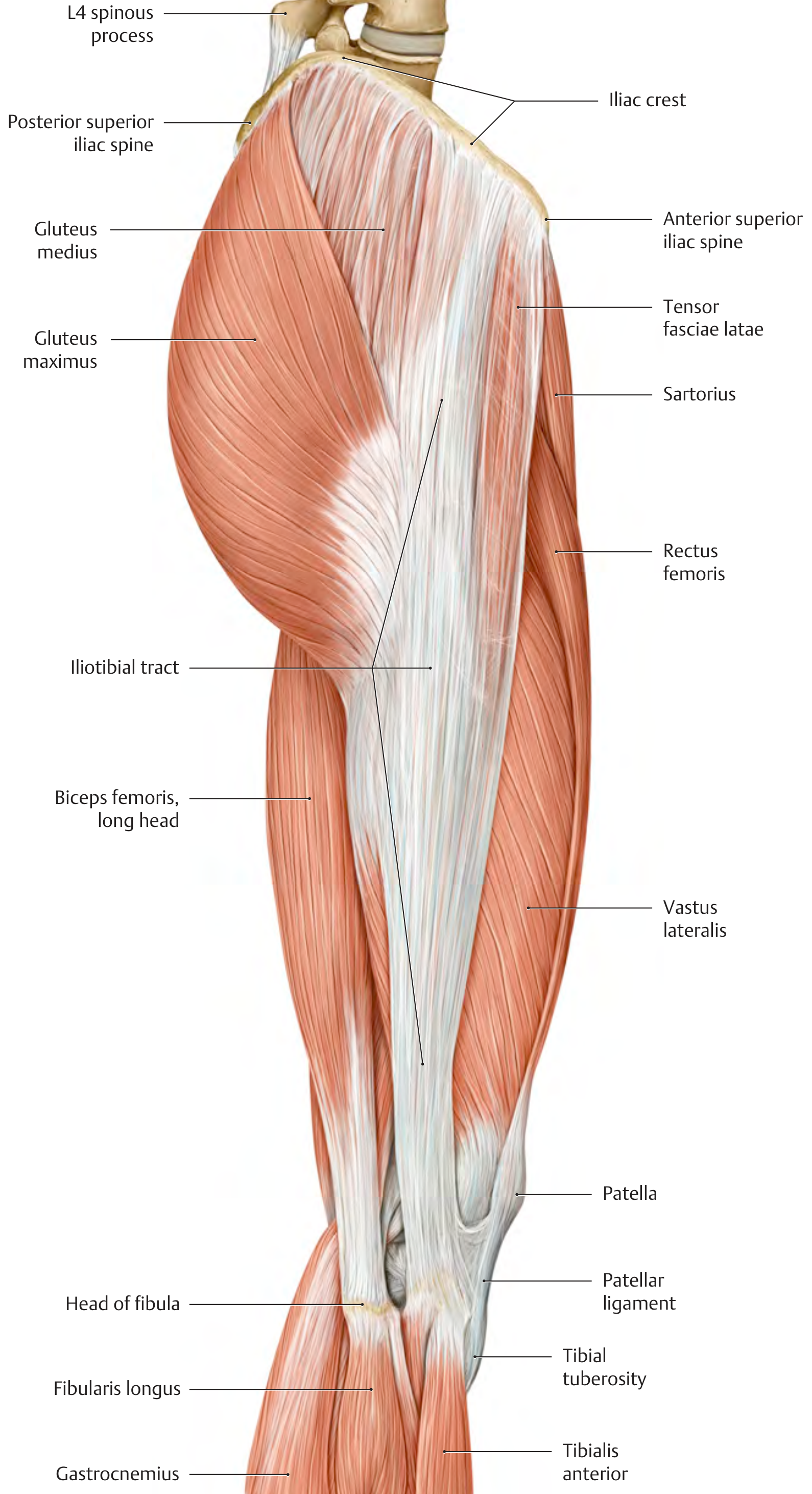
Lateral View - Superficial Thigh Muscles
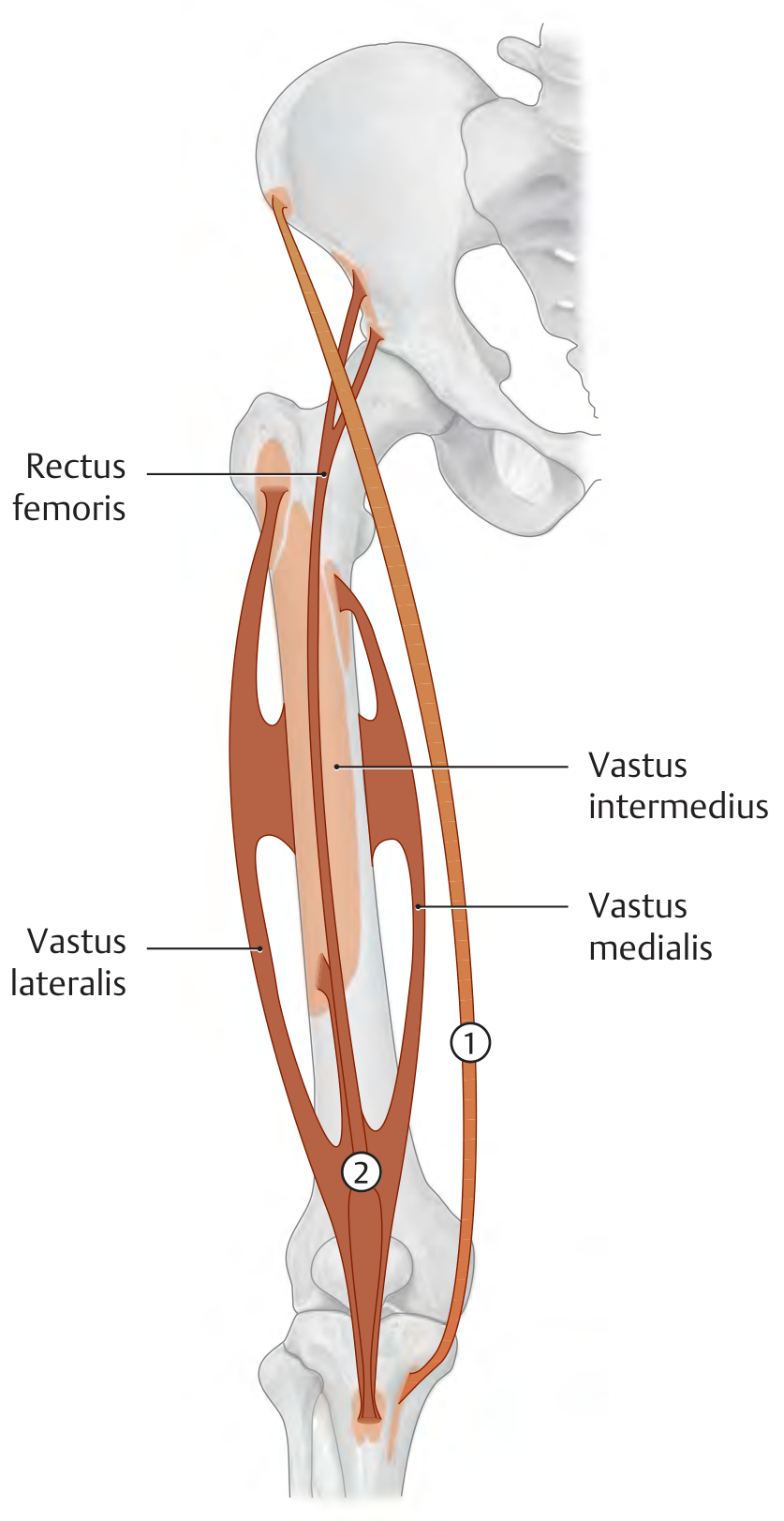
Quadriceps Femoris Schematic (Anterior Compartment)
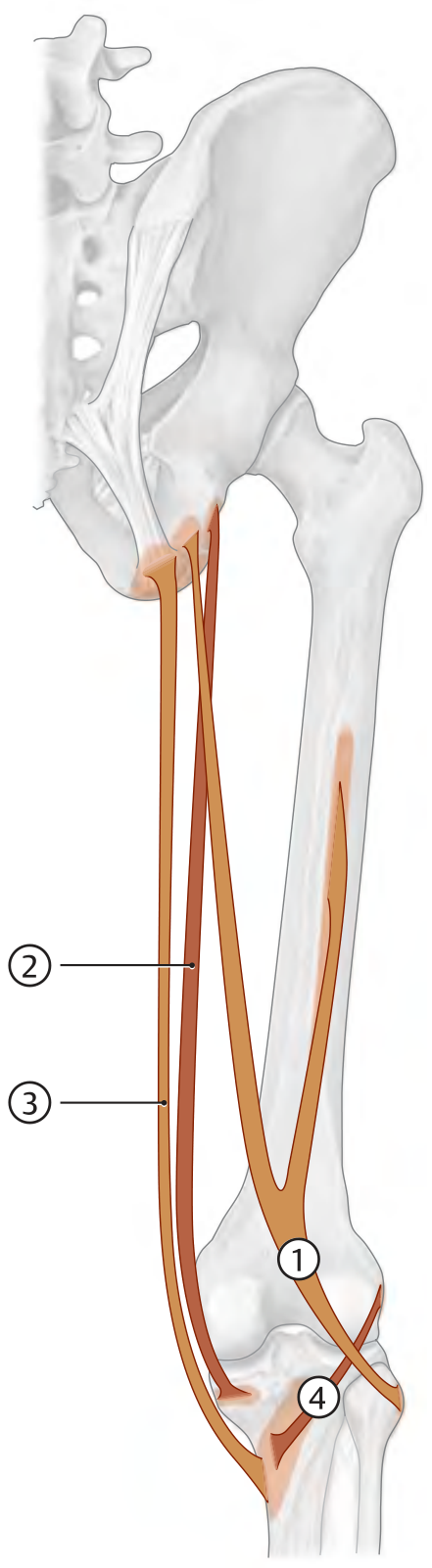
Posterior Thigh (Hamstrings) Schematic
1. Anterior Compartment (Extensors)
Innervated by the femoral nerve (L2-L4).
Sartorius
| Origin | Anterior superior iliac spine (ASIS) |
| Insertion | Medial tibial tuberosity (pes anserinus, with gracilis + semitendinosus) |
| Action | Hip: flexion, abduction, external rotation; Knee: flexion + internal rotation |
| Nerve | Femoral nerve (L1-L4) |
The sartorius is the longest muscle in the body. It crosses both the hip and knee, acting as a biarticular muscle. At the knee level, it migrates posteriorly to contribute to the pes anserinus ("goose foot").
Quadriceps Femoris (4 heads + articularis genus)
All four heads converge onto the tibial tuberosity via the patellar ligament. The patella is a sesamoid bone embedded in the quadriceps tendon.
| Head | Origin |
|---|---|
| Rectus femoris | Anterior inferior iliac spine (straight head); acetabular roof (reflected head) |
| Vastus medialis | Medial lip of linea aspera; distal intertrochanteric line |
| Vastus lateralis | Lateral lip of linea aspera; lateral surface of greater trochanter |
| Vastus intermedius | Anterior femoral shaft |
| Articularis genus | Distal femoral shaft (tightens suprapatellar recess during extension) |
- Insertion (all): Tibial tuberosity via patellar ligament; medial/lateral patellar retinacula
- Action: Knee extension (all 4); hip flexion (rectus femoris only)
- Nerve: Femoral nerve (L2-L4)
Clinical note: Quadriceps weakness or paralysis prevents active knee extension. The patient compensates by hyperextending the knee so the line of gravity shifts anterior to the joint axis, allowing passive stability through posterior capsule and ligaments.
2. Medial Compartment (Adductors)
Innervated primarily by the obturator nerve (L2-L4). The adductor magnus has dual supply (obturator + tibial nerve).
| Muscle | Origin | Insertion | Action |
|---|---|---|---|
| Adductor longus | Anterior pubis | Middle third of linea aspera | Adduction, flexion |
| Adductor brevis | Body/inferior ramus of pubis | Upper linea aspera | Adduction |
| Adductor magnus | Inferior pubic ramus to ischial tuberosity | Linea aspera (adductor part) + adductor tubercle (hamstring part) | Adduction; hamstring part = hip extension |
| Adductor minimus | Inferior pubic ramus | Linea aspera (proximal) | Adduction |
| Pectineus | Pectineal line of pubis | Pectineal line of femur | Adduction, flexion |
| Gracilis | Body/inferior ramus of pubis | Medial tibial tuberosity (pes anserinus) | Adduction; knee flexion + internal rotation |
Key facts:
- The adductor magnus is the largest adductor - it makes up ~27% of total thigh muscle mass and ~60% of adductor mass.
- The adductor hiatus is a gap in the adductor magnus where the femoral artery and vein pass from the anterior thigh into the popliteal fossa.
- The adductors' primary functions are adduction, some extension, and medial rotation; together with lower abdominal muscles they stabilize the pelvis during activity.
- Among athletes, adductor longus is the most commonly injured adductor muscle.
3. Posterior Compartment (Hamstrings / Flexors)
Innervated by the tibial nerve (L5-S2), except the short head of biceps femoris (common fibular nerve, L5-S2). All originate from the ischial tuberosity (except the short head of biceps).
| Muscle | Origin | Insertion | Action |
|---|---|---|---|
| Biceps femoris (long head) | Ischial tuberosity + sacrotuberous ligament | Head of fibula | Hip extension/adduction; knee flexion + external rotation |
| Biceps femoris (short head) | Lateral lip of linea aspera (middle third) | Head of fibula | Knee flexion + external rotation |
| Semimembranosus | Ischial tuberosity | Medial tibial condyle; oblique popliteal ligament | Hip extension/adduction; knee flexion + internal rotation |
| Semitendinosus | Ischial tuberosity + sacrotuberous ligament | Medial tibial tuberosity (pes anserinus) | Hip extension/adduction; knee flexion + internal rotation |
Key facts:
- The hamstrings are biarticular - they cross both the hip and knee. This creates two types of muscle insufficiency:
- Passive insufficiency: with knee extended, hamstrings are too short to allow full hip flexion (tight hamstrings in straight leg raise)
- Active insufficiency: with hip extended, hamstrings cannot shorten enough for maximal knee flexion
- Semitendinosus and semimembranosus produce internal rotation at the knee; biceps femoris produces external rotation.
- Among professional soccer players, the hamstrings are the second most commonly injured muscle group (28%), after quadriceps (32%).
Compartment Summary
| Compartment | Muscles | Nerve | Primary Action |
|---|---|---|---|
| Anterior | Sartorius, Quadriceps femoris (x4 + articularis genus) | Femoral nerve | Knee extension; hip flexion |
| Medial | Adductor longus/brevis/magnus, Pectineus, Gracilis, Adductor minimus | Obturator nerve (+ tibial for adductor magnus) | Hip adduction |
| Posterior | Biceps femoris, Semimembranosus, Semitendinosus | Tibial nerve (sciatic) | Knee flexion; hip extension |
Sources: General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy; Imaging Anatomy Text and Atlas Vol. 3, Bones, Joints, Vessels and Nerves
This is a shared conversation. Sign in to Orris to start your own chat.