Great saphenous vein histology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have all the information needed for a comprehensive answer. The histology image of the great saphenous vein (Figure 13.28) is clearly visible. Let me compile the full answer.
Great Saphenous Vein - Histology
The great saphenous vein (GSV) is the longest vein in the body, running subcutaneously from the dorsum of the foot to the saphenofemoral junction just below the inguinal ligament. Histologically, it is classified as a muscular vein - a designation it earns because of an unusually large amount of smooth muscle distributed across all three tunics.
Histological Image (Fig. 13.28, H&E x380)
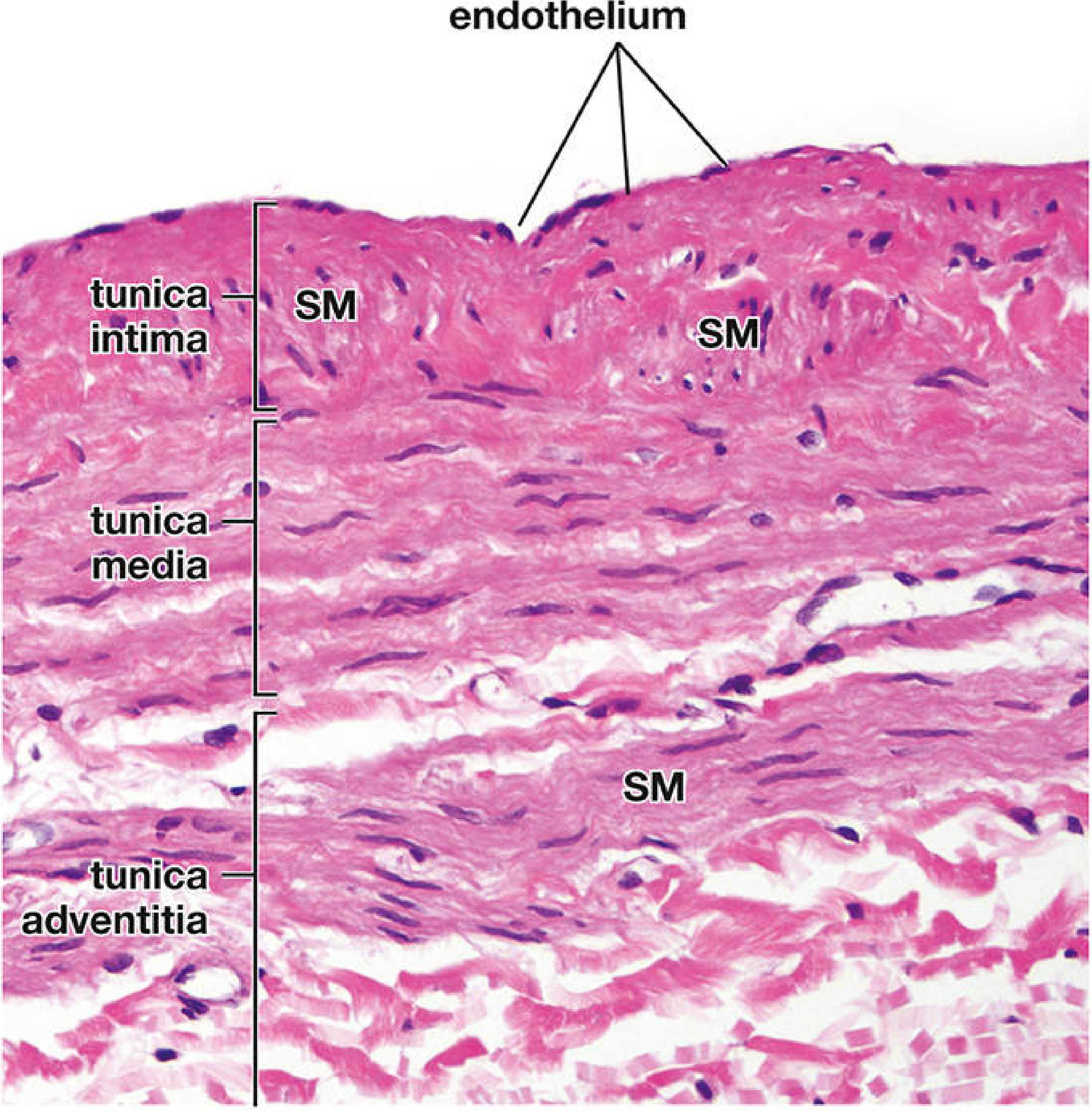
Figure 13.28 - Section through the wall of the great saphenous vein showing all three tunics (H&E x380). SM = smooth muscle bundles. Courtesy of Dr. Joseph J. Maleszewski. (Histology: A Text and Atlas)
Layers in Detail
1. Tunica Intima
- Lined by a single layer of endothelial cells resting on a basal lamina
- Has a thicker subendothelial layer than most other medium-sized veins
- Contains numerous longitudinal smooth muscle bundles separated by connective tissue fibers - this is the most distinctive feature of the GSV compared to typical veins
- A thin, poorly developed internal elastic membrane (often discontinuous) separates the intima from the media
2. Tunica Media
- Contains a thick layer of circularly arranged smooth muscle cells
- Thicker than the tunica media of an ordinary medium vein
- Interspersed with collagen and elastic fibers
3. Tunica Adventitia
- Well-developed and prominent - the thickest layer
- Contains additional smooth muscle fibers arranged in spiral, oblique, and longitudinal bundles
- Also contains collagen fibers, elastic fiber networks, fibroblasts, and vasa vasorum
Key Distinguishing Features (vs. Typical Medium Vein)
| Feature | Typical Medium Vein | Great Saphenous Vein |
|---|---|---|
| Tunica intima | Thin, minimal SM | Thick, with longitudinal SM bundles |
| Tunica media | Few circular SM layers | Thick, prominent circular SM |
| Tunica adventitia | Thickest layer, mainly collagen | Well-developed + spiral/oblique/longitudinal SM |
| Internal elastic membrane | Thin/discontinuous | Poorly developed, thin |
| Classification | Medium vein | Muscular vein |
Clinical Relevance
The GSV is frequently harvested from the lower limb for coronary artery bypass graft (CABG) surgery when arterial grafts (e.g., internal thoracic artery) are unavailable or multiple grafts are needed. The unusual abundance of smooth muscle in all three layers - particularly the longitudinal bundles in the intima and adventitia - gives the GSV structural properties that make it suitable as a conduit, though its venous architecture differs significantly from the native coronary artery wall.
The vein is also predisposed to varicose vein formation when valvular incompetence leads to venous hypertension; the muscular wall undergoes fibrosis and dilatation over time.
Source: Histology: A Text and Atlas With Correlated Cell and Molecular Biology (Pawlina & Ross), pp. 1122-1123
Description
Asking for Preferences
Description of great saphenous vein
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed. Here is a comprehensive description of the great saphenous vein.
Great Saphenous Vein - Description
Overview
The great saphenous vein (GSV) is the longest vein in the body. It is a superficial vein of the lower limb, lying above the deep fascia (fascia lata) but deep to the saphenous fascia, within the so-called saphenous "envelope." It belongs to the superficial venous system, which also includes the small saphenous vein (SSV).
Course
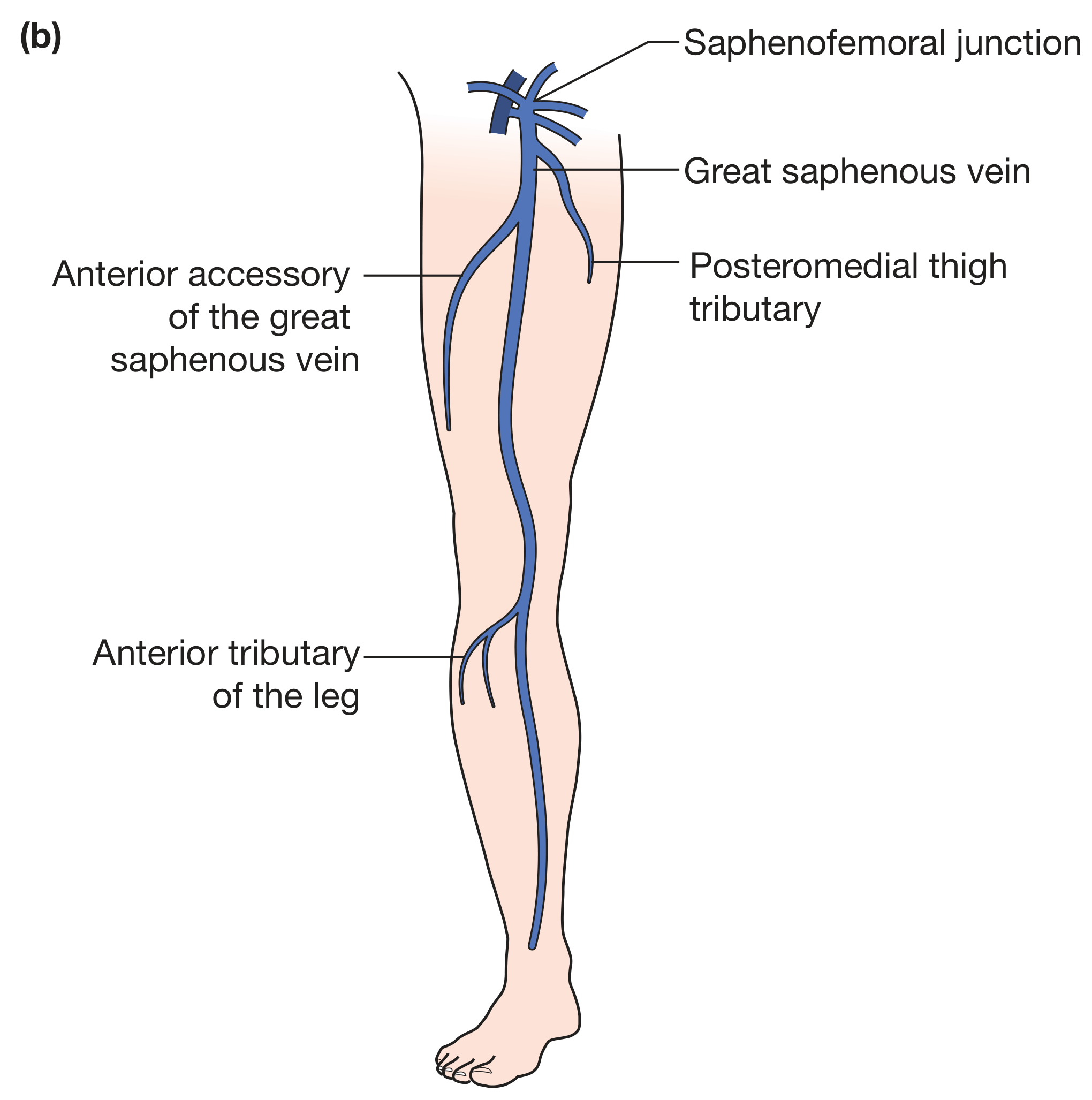
Figure: Anatomy of the superficial venous system (great saphenous axis) - Bailey & Love's Short Practice of Surgery, 28th Ed.
The GSV follows a predictable but variable course from foot to groin:
-
Origin - Arises from the medial end of the dorsal venous arch of the foot (from the medial marginal vein). Because the sole of the foot is under significant pressure, most venous drainage runs dorsally.
-
Ankle - Passes anterior to the medial malleolus, accompanied by the saphenous nerve (a branch of the femoral nerve, L3-L4). This is a consistent and important anatomical landmark.
-
Leg (calf) - Ascends along the medial aspect of the leg, running superficial to the medial surface of the tibia, with the saphenous nerve in close proximity.
-
Knee - Loops posteriorly around the medial condyle of the femur before continuing up the medial thigh.
-
Thigh - Ascends along the medial aspect of the thigh in the superficial tissues, anterior and medial throughout.
-
Groin (termination) - Passes through the saphenous opening (also called the fossa ovalis or cribriform fascia), located approximately 2.5 cm below and lateral to the pubic tubercle. It terminates by draining into the common femoral vein (CFV) at the saphenofemoral junction (SFJ).
Tributaries
Just before piercing the cribriform fascia, the GSV receives several named tributaries that correspond to the branches of the common femoral artery:
- Superficial epigastric vein
- Superficial circumflex iliac vein
- Superficial external pudendal vein
- Deep external pudendal vein
Along its course, the GSV also unites with variable superficial tributaries, the most clinically important being:
- Anterior accessory of the great saphenous vein (AAGSV) - originates around the lateral border of the knee and usually drains into the GSV in the thigh or at the SFJ. It is commonly mistaken for the GSV itself on duplex ultrasound (a true duplicate GSV is rare).
- Posteromedial thigh tributary
- Anterior tributary of the leg
- Giacomini vein - a communicating vessel from the SSV system that occasionally connects to the GSV
Perforating Veins
Throughout the calf and thigh, valved perforating (communicating) veins connect the GSV to the deep venous system. They normally allow one-way flow from superficial to deep. The most clinically important perforators are:
- Dodd veins (mid-thigh)
- Boyd vein (upper medial calf / knee)
- Cockett veins (medial lower calf) - also called the ankle perforators, these drain into the posterior tibial veins
Valves
The GSV contains multiple bicuspid valves throughout its length (typically 10-20) that direct blood centrally (toward the heart) and prevent reflux. The most important is the valve at the saphenofemoral junction itself. Incompetence of these valves is the primary cause of varicose veins.
Important Relations
| Region | Relation |
|---|---|
| Ankle | Anterior to medial malleolus; saphenous nerve runs with it |
| Leg | Medial border of tibia; saphenous nerve |
| Knee | Posterior to medial femoral condyle |
| Thigh | Medial aspect; saphenous nerve diverges in mid-thigh |
| Groin | Passes through saphenous opening; ~2.5 cm inferolateral to pubic tubercle |
Clinical Significance
- Varicose veins - The GSV is the most frequently affected vein by superficial venous incompetence. Valvular failure leads to reflux, venous hypertension, tortuous dilatation, and symptoms of chronic venous disease.
- CABG graft - The GSV is commonly harvested for use as a conduit in coronary artery bypass graft surgery when arterial grafts are insufficient.
- Venous cutdown / IV access - The constant position anterior to the medial malleolus makes it a reliable site for emergency venous cutdown.
- Saphenous nerve injury - The intimate relationship with the saphenous nerve means that GSV stripping or ablation can cause medial leg numbness.
- Great saphenous vein stripping / endovenous ablation - Used surgically for varicose vein treatment.
Sources: Bailey & Love's Short Practice of Surgery (28th ed.), p. 1047; Harrison's Principles of Internal Medicine (22nd ed.), p. 2223; Gray's Anatomy for Students, p. 706; Histology: A Text and Atlas (Pawlina & Ross), pp. 1122-1123
This is a shared conversation. Sign in to Orris to start your own chat.