Dead space Full details for md exam answer 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full 10-mark MD exam answer.
Dead Space - Complete MD Exam Answer (10 Marks)
Definition
Dead space is the volume of the respiratory system that does not participate in gas exchange. It encompasses both the conducting airway volume (anatomic dead space) and any additional lung volume rendered non-functional (physiologic dead space).
- Costanzo Physiology 7th Ed, p. 198
Classification
1. Anatomic Dead Space
The volume of gas in the conducting airways (nose/mouth, trachea, bronchi, bronchioles) - but NOT the respiratory bronchioles or alveoli - is called anatomic dead space.
Normal value: ~150 mL in a healthy adult male (roughly 1 mL per pound of ideal body weight or ~2 mL/kg body weight).
- Increases slightly with large inspirations (radial traction from lung parenchyma widens bronchi)
- Slightly larger in men than women due to airway anatomy
- Increases mildly after age 50-60 years
What happens with each breath: At end-expiration, the conducting airways are filled with "stale" alveolar air from the previous breath. On the next inspiration (e.g., 500 mL tidal volume):
- 150 mL remains in the conducting airways (anatomic dead space) and never reaches alveoli
- Only 350 mL of fresh air reaches the alveoli for gas exchange
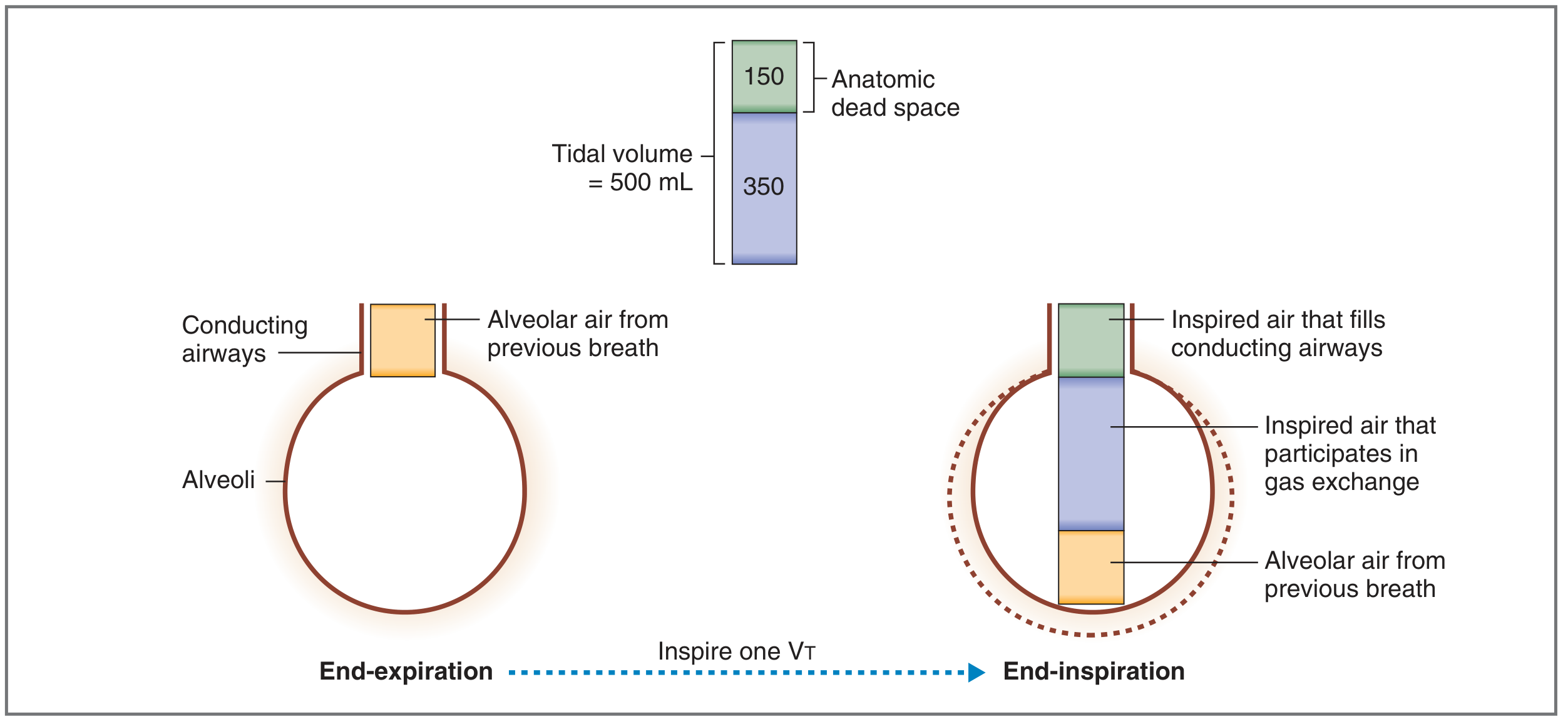
Fig. 5.3 - Anatomic dead space. 150 mL of tidal volume (VT = 500 mL) fills the conducting airways; 350 mL participates in gas exchange. (Costanzo Physiology 7th Ed)
2. Alveolar Dead Space
Ventilated alveoli that receive no blood flow (V/Q = infinity). Gas reaches these alveoli but cannot exchange with pulmonary capillary blood.
- Normal alveolar dead space is negligible
- Becomes significant in pulmonary embolism, severe hypotension, etc.
3. Physiologic Dead Space (Total Dead Space)
Physiologic dead space = Anatomic dead space + Alveolar dead space
It is the total volume of the lungs that does not participate in gas exchange.
- In healthy persons: physiologic dead space ≈ anatomic dead space (alveolar dead space is near zero)
- In disease: physiologic dead space >> anatomic dead space
- Can reach 1-2 liters in severe disease (up to 10x the anatomic dead space)
- Normal VD/VT ratio = ~0.3 (i.e., 30% of each breath is "wasted")
4. Apparatus/Mechanical Dead Space
Additional dead space introduced by breathing circuits, endotracheal tubes, or face masks - clinically relevant in ventilated patients and anesthesia. Not a natural compartment but increases total wasted ventilation.
Measurement Methods
(A) Bohr Equation - Measures Physiologic Dead Space
The Bohr equation uses CO2 as a marker gas, based on three assumptions:
- All expired CO2 comes from functioning (ventilated + perfused) alveoli
- Inspired air has essentially zero CO2
- Dead space gas contributes no CO2 to expiration
$$V_D = V_T \times \frac{PaCO_2 - PE_{CO_2}}{PaCO_2}$$
Where:
- VD = physiologic dead space (mL)
- VT = tidal volume (mL)
- PaCO2 = arterial blood PCO2 (reflects alveolar PCO2 in normal lungs) (mmHg)
- PECO2 = PCO2 of mixed expired air (mmHg)
Worked example:
- VT = 550 mL, PaCO2 = 40 mmHg, PECO2 = 30 mmHg
- VD = 550 × (40 - 30)/40 = 550 × 0.25 = 137.5 mL
- VD/VT ratio = 137.5/550 = 0.25 (25% wasted)
Interpretation of extremes:
-
If dead space = 0: PECO2 = PaCO2 → fraction = 0 → VD = 0
-
If dead space = entire VT (no gas exchange at all): PECO2 = 0 → fraction = 1.0 → VD = VT
-
Murray & Nadel's Textbook of Respiratory Medicine, p. 221; Fishman's Pulmonary Diseases, p. (block7)
(B) Fowler's Method (Single-Breath Nitrogen Washout) - Measures Anatomic Dead Space
The patient inhales a single breath of 100% O2 and then exhales while expired N2 concentration is continuously measured. Four phases are identified:
| Phase | Gas expired | N2 concentration |
|---|---|---|
| Phase I | Pure dead space gas (O2) | 0% N2 |
| Phase II | Mixture of dead space + alveolar gas | Rising |
| Phase III | Pure alveolar gas ("alveolar plateau") | Stable elevated level |
| Phase IV | Airway closure in lower lobes begins | Rising further |
Dead space = volume expired from peak inspiration to the midpoint of Phase II
The closing volume (CV) marks the start of Phase IV - the lung volume above RV where dependent airway closure begins.
- Ganong's Review of Medical Physiology 26th Ed
Effect of Dead Space on Alveolar Ventilation
$$\dot{V}_A = (V_T - V_D) \times \text{Respiratory rate}$$
- Normal: VA = (500 - 150) × 12 = 4,200 mL/min
Critical point - Shallow vs. Deep Breathing (same minute ventilation = 6 L/min):
| Rate | Tidal Volume | Minute Volume | Alveolar Ventilation |
|---|---|---|---|
| 30/min | 200 mL | 6 L | (200-150) × 30 = 1,500 mL/min |
| 10/min | 600 mL | 6 L | (600-150) × 10 = 4,500 mL/min |
Conclusion: Rapid shallow breathing dramatically reduces alveolar ventilation with the same minute ventilation, because dead space comprises a larger fraction of each small tidal volume. This is a clinically dangerous pattern (e.g., in respiratory fatigue).
- Ganong's Review of Medical Physiology 26th Ed, Table 34-1; Guyton & Hall, p. 499
Physiologic Dead Space and V/Q Mismatch
- V/Q > 1 (high V/Q) → excess ventilation relative to perfusion → alveolar dead space
- V/Q = infinity → completely unperfused alveolus → pure dead space unit
- Physiologic dead space is the functional measure of V/Q inequality - it quantifies all "wasted ventilation"
- VD/VT > 0.3 is abnormal; VD/VT > 0.6 is associated with ventilatory failure
Clinical Consequences of Increased Dead Space
| Effect | Mechanism |
|---|---|
| Hypercapnia | Wasted ventilation → CO2 retention; does NOT occur until VD > 50% of total lung volume due to compensatory hyperventilation |
| Hypoxemia | High V/Q areas cannot offload O2 to blood; generally responds well to supplemental O2 (unlike shunt) |
| Increased work of breathing | Must increase minute ventilation to maintain adequate alveolar ventilation |
| Ventilatory failure | When respiratory muscles fatigue and cannot compensate for large dead space |
Local compensatory mechanism: In pathologic dead space, local bronchoconstriction occurs to normalize the V/Q ratio (reduces ventilation to match low perfusion).
Causes of Increased Physiologic Dead Space
Increased alveolar dead space (reduced pulmonary perfusion):
- Pulmonary embolism (most classic cause - obstructs blood flow to ventilated alveoli)
- Severe hypotension / cardiogenic shock (global decrease in pulmonary capillary perfusion)
- ARDS / COPD / emphysema (destruction of alveolar walls and capillary bed; bleb formation)
- Mechanical ventilation with high PEEP (overdistension compresses alveolar capillaries)
- Hypovolemia
Increased anatomic dead space:
- Rapid shallow breathing (dead space/VT ratio increases)
- Tracheostomy/endotracheal intubation bypasses upper airway dead space (reduces dead space)
- Bronchodilation (e.g., beta-2 agonists slightly increase anatomic dead space)
- Apparatus dead space from ventilator circuits
Summary Table
| Feature | Anatomic Dead Space | Alveolar Dead Space | Physiologic Dead Space |
|---|---|---|---|
| Definition | Volume of conducting airways | Ventilated but unperfused alveoli | Anatomic + Alveolar |
| Normal value | ~150 mL (1 mL/lb IBW) | ~0 mL | ~150 mL |
| V/Q ratio | N/A | Infinity | - |
| Measured by | Fowler's method (N2 washout) | Bohr - Fowler difference | Bohr equation |
| Clinical significance | Baseline "wasted" ventilation | Increases in disease | Gold standard for dead space assessment |
Key Numbers to Remember for Exam
- Normal anatomic dead space: 150 mL (= 1 mL/lb body weight)
- Normal tidal volume: 500 mL
- Normal VD/VT ratio: 0.3 (30%)
- Normal alveolar ventilation: 4,200 mL/min (12 breaths × 350 mL)
- Hypercapnia from dead space develops when VD/VT exceeds ~0.5
- Physiologic dead space = 10x anatomic dead space possible in severe disease (up to 1-2 L)
Sources: Costanzo Physiology 7th Ed | Guyton & Hall Textbook of Medical Physiology | Ganong's Review of Medical Physiology 26th Ed | Murray & Nadel's Textbook of Respiratory Medicine | Fishman's Pulmonary Diseases & Disorders | Frameworks for Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.