Define blood pressure and the various mechanisms involved in maintenance of bp ( short, intermediate and long ways) Use as many flowcharts and tabular forms to explain the answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the content and diagrams needed. Let me compile the comprehensive answer.
Blood Pressure - Definition and Mechanisms of Maintenance
1. Definition of Blood Pressure
Blood pressure (BP) is the lateral pressure exerted by the flowing blood on the walls of the blood vessels at any given time. It is the driving force that propels blood through the circulatory system.
The fundamental equation is:
BP = Cardiac Output (CO) × Total Peripheral Resistance (TPR)
| Term | Definition | Normal Value |
|---|---|---|
| Systolic BP | Peak pressure during ventricular systole | 120 mmHg |
| Diastolic BP | Lowest pressure during diastole | 80 mmHg |
| Pulse pressure | Systolic - Diastolic | 40 mmHg |
| Mean Arterial Pressure (MAP) | DBP + 1/3 pulse pressure | ~93 mmHg |
| Normal BP | 120/80 mmHg | - |
| Hypertension | ≥ 130/80 mmHg | (ACC/AHA 2017) |
| Hypotension | < 90/60 mmHg | - |
2. Determinants of Blood Pressure
(Robbins Basic Pathology, Fig. 8.2)
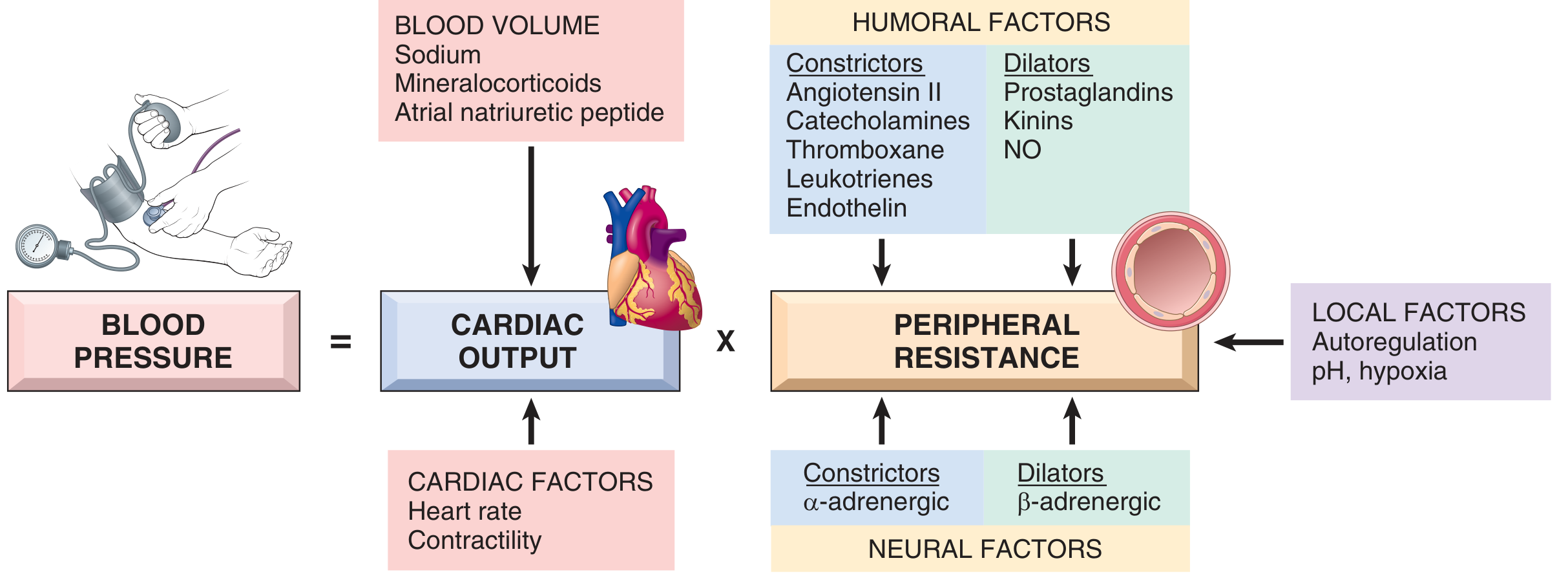
| Determinant | Sub-factors | Effect on BP |
|---|---|---|
| Cardiac Output | Heart rate, Contractility | ↑ CO → ↑ BP |
| Blood Volume | Sodium, Mineralocorticoids, ANP | ↑ Volume → ↑ CO → ↑ BP |
| Peripheral Resistance | Arteriolar tone | ↑ TPR → ↑ BP |
| Humoral vasoconstrictors | Ang II, Catecholamines, Endothelin, Thromboxane | ↑ TPR → ↑ BP |
| Humoral vasodilators | Prostaglandins, Kinins, Nitric Oxide | ↓ TPR → ↓ BP |
| Neural (sympathetic α) | α-adrenergic → vasoconstriction | ↑ TPR → ↑ BP |
| Neural (sympathetic β) | β-adrenergic → vasodilation | ↓ TPR → ↓ BP |
| Local factors | Autoregulation, pH, hypoxia | Variable |
3. Overview: Time-Based Classification of BP Control
MECHANISMS OF BP CONTROL
│
├── SHORT-TERM (Seconds–Minutes)
│ ├── Baroreceptor reflex
│ ├── Chemoreceptor reflex
│ ├── CNS ischemic response
│ └── Atrial & arterial low-pressure reflexes
│
├── INTERMEDIATE (Minutes–Hours)
│ ├── Capillary fluid shift mechanism
│ ├── Stress relaxation of vessel walls
│ └── Renin-Angiotensin System (early activation)
│
└── LONG-TERM (Hours–Days–Lifetime)
├── Renal pressure-natriuresis (most important)
├── RAAS (sustained) + Aldosterone
├── Antidiuretic hormone (ADH/AVP)
└── Atrial Natriuretic Peptide (ANP/BNP)
4. SHORT-TERM Mechanisms (Seconds to Minutes)
These are neurally mediated, rapid reflexes acting through the autonomic nervous system.
4A. Baroreceptor (Pressoreceptor) Reflex
This is the fastest and most important short-term mechanism.
(Costanzo Physiology, Fig. 4.31)
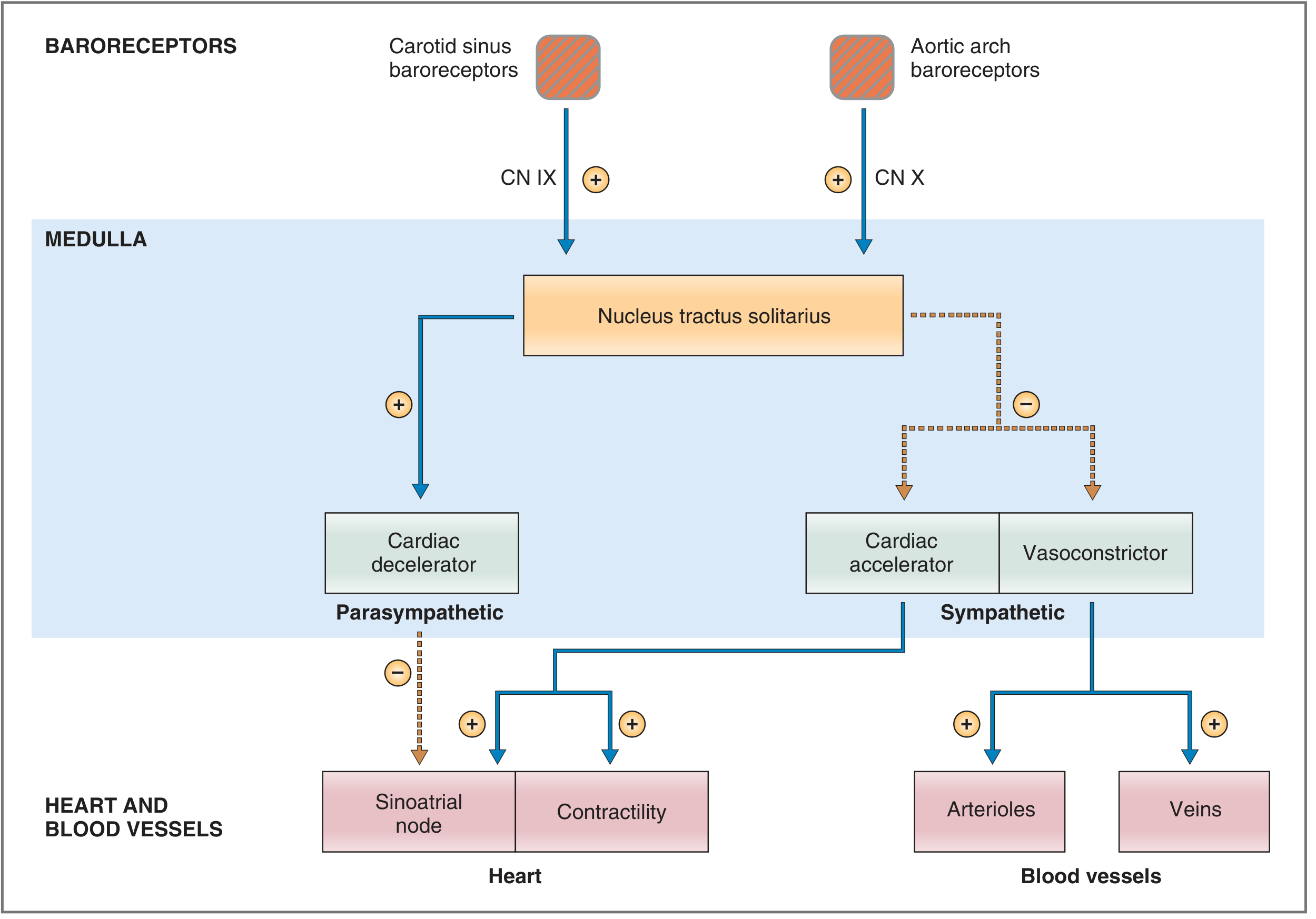
Flowchart - Response to INCREASED BP:
↑ Arterial BP
│
▼
Stretch of baroreceptors
(Carotid sinus via CN IX + Aortic arch via CN X)
│
▼
↑ Firing in afferent nerves
│
▼
Nucleus Tractus Solitarius (NTS) - Medulla
│
├──────────────────────────────────┐
▼ ▼
↑ Parasympathetic (vagal) ↓ Sympathetic outflow
to SA node to heart & vessels
│ │
▼ ▼
↓ Heart rate ↓ HR + ↓ Contractility
↓ CO
↓ Arteriolar tone (vasodilation)
↓ Venous tone → ↑ Venous compliance
│
▼
↓ Cardiac Output + ↓ TPR
│
▼
BP RESTORED TO NORMAL
Flowchart - Response to DECREASED BP (Hemorrhage):
↓ Arterial BP (e.g., hemorrhage)
│
▼
↓ Stretch on baroreceptors
→ ↓ Firing rate of CN IX & X
│
▼
NTS activates:
↓ Parasympathetic outflow
↑ Sympathetic outflow
│
├─────────────────────────────────────┐
▼ ▼
↑ HR + ↑ Contractility ↑ Arteriolar vasoconstriction
→ ↑ Cardiac Output → ↑ TPR
↑ Venous constriction
→ ↑ Venous return (Frank-Starling)
│
▼
↑ Cardiac Output × ↑ TPR
│
▼
BP RESTORED TO NORMAL
| Feature | Baroreceptor Location | Nerve | Sensitive to |
|---|---|---|---|
| Carotid sinus | Bifurcation of common carotid | CN IX (Glossopharyngeal) | Increases AND decreases in BP |
| Aortic arch | Aortic arch | CN X (Vagus) | Primarily increases in BP |
Key fact: Baroreceptors are more sensitive to the rate of change than the absolute level of pressure. In chronic hypertension, they reset to the new higher set-point and no longer oppose it. - Costanzo Physiology, 7th Ed.
4B. Chemoreceptor Reflex
↓ PO₂ / ↑ PCO₂ / ↓ pH
(peripheral carotid & aortic bodies)
│
▼
Peripheral chemoreceptors fire
│
▼
Medullary vasomotor center activated
(positive drive → vasoconstriction)
│
▼
↑ TPR → ↑ BP
Note: Bradycardia occurs only when ventilation is fixed.
When ventilation is normal, tachycardia results instead.
4C. CNS Ischemic Response (Cushing Response)
Severe ↓ cerebral blood flow
(MAP < 50 mmHg)
│
▼
CO₂ accumulation in brain → stimulates vasomotor center
│
▼
Massive sympathetic outflow
│
▼
Intense vasoconstriction + ↑ HR + ↑ contractility
│
▼
↑ BP (emergency "last resort" mechanism)
Summary Table: Short-Term Mechanisms
| Mechanism | Sensor | Response Time | Max Effect | Clinical Significance |
|---|---|---|---|---|
| Baroreceptor reflex | Carotid sinus, Aortic arch | Seconds | Moderate | Fainting, orthostatic hypotension |
| Chemoreceptor reflex | Carotid & aortic bodies | Seconds | Moderate | Hypoxia, breath-holding |
| CNS ischemic response | Brain CO₂ levels | Seconds | Very high | Cushing's triad in raised ICP |
| Atrial reflex | Atrial stretch receptors | Seconds | Mild | Volume regulation |
5. INTERMEDIATE Mechanisms (Minutes to Hours)
These act after the baroreceptor reflex and involve redistribution of fluids and vascular reactivity.
5A. Capillary Fluid Shift Mechanism
↑ BP (acute rise)
│
▼
↑ Capillary hydrostatic pressure
│
▼
Net fluid filtration OUT of capillaries
into interstitial space
│
▼
↓ Blood volume (intravascular)
│
▼
↓ Venous return → ↓ CO
│
▼
↓ BP (over 10-30 minutes)
Reverse: ↓ BP → fluid absorbed from interstitium
→ ↑ Blood volume → ↑ BP
- This mechanism can absorb up to 500 mL of fluid from interstitium within 30 minutes.
- Effectiveness: ~70% as powerful as the baroreceptor reflex.
5B. Stress Relaxation of Vessel Walls
Acute ↑ BP
│
▼
Vessel walls stretched
│
▼
Vascular smooth muscle RELAXES over time
(viscoelastic "creep" property)
│
▼
↑ Vascular compliance
↓ Vascular resistance
│
▼
↓ BP toward normal
(Works over minutes to hours)
5C. Early Renin-Angiotensin System Activation
The RAAS begins activation within minutes but full effect takes hours. (See also long-term section below.)
6. LONG-TERM Mechanisms (Hours to Days)
These are the most powerful and most sustained mechanisms, primarily involving the kidneys. The kidney is considered the master controller of long-term BP.
(Fuster & Hurst's The Heart, Fig. 5-8)
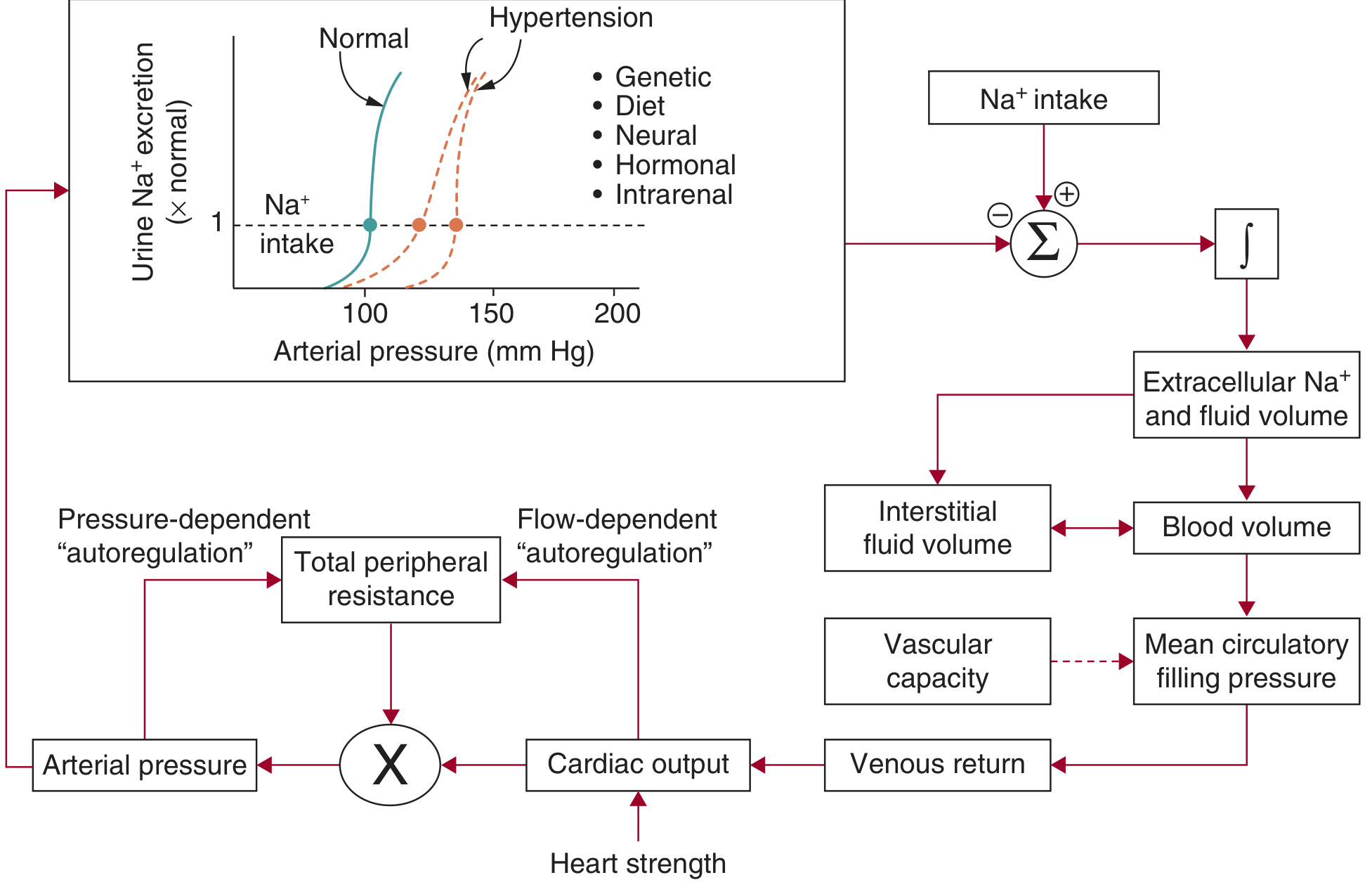
6A. Renal Pressure-Natriuresis (Most Powerful Long-Term Mechanism)
↑ Arterial BP
│
▼
↑ Renal perfusion pressure
│
▼
Kidney excretes MORE Na⁺ and water
(Pressure Natriuresis / Pressure Diuresis)
│
▼
↓ Extracellular fluid volume
↓ Blood volume
│
▼
↓ Venous return → ↓ CO
│
▼
↓ BP returns to normal
Reverse: ↓ BP → kidney retains Na⁺ and water
→ ↑ Blood volume → ↑ BP
"In all types of hypertension studied thus far, there is a shift of pressure natriuresis that sustains hypertension." - Fuster & Hurst's The Heart, 15th Ed.
| Normal Pressure-Natriuresis | In Hypertension |
|---|---|
| Curve shifts right-ward due to genetic/hormonal factors | Kidney requires higher BP to excrete the same Na⁺ |
| Na⁺ balanced at ~100 mmHg MAP | Na⁺ balanced at 130-150 mmHg MAP |
| Diuretics and RAAS blockers reset this curve | Surgery / drugs shift curve back left |
6B. Renin-Angiotensin-Aldosterone System (RAAS)
(Robbins Basic Pathology, Fig. 8.3)
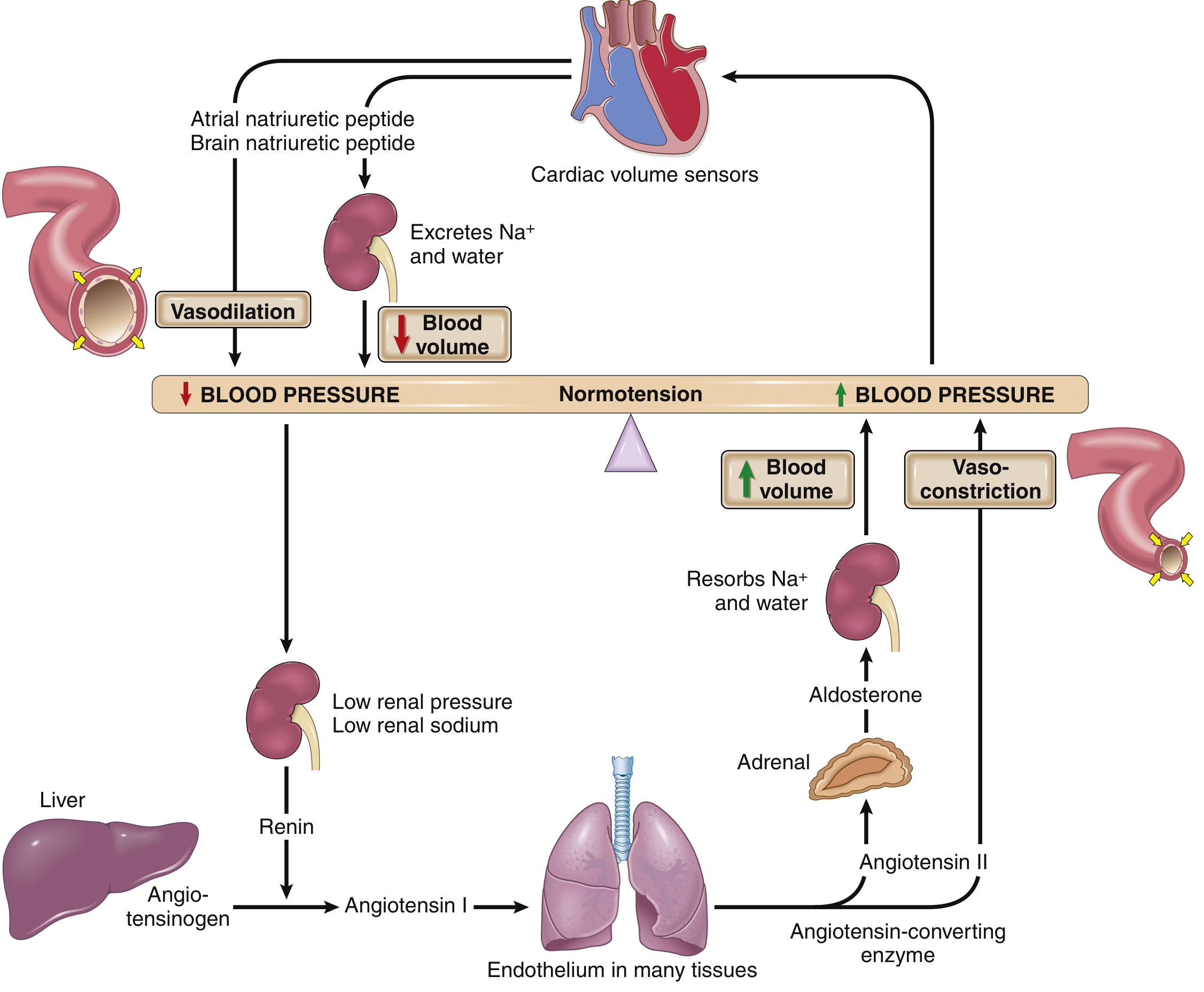
Flowchart:
↓ BP / ↓ Renal perfusion / ↓ Renal Na⁺
│
▼
Juxtaglomerular cells (renal afferent arteriole)
→ release RENIN
│
▼
Renin cleaves ANGIOTENSINOGEN (liver)
→ ANGIOTENSIN I
│
▼
ACE (lung endothelium + vascular endothelium)
→ ANGIOTENSIN II
│
├──────────────────────────────────────────────┐
│ │
▼ ▼
Direct vasoconstriction Adrenal cortex → ALDOSTERONE
(↑ TPR → ↑ BP) │
▼
↑ Na⁺ reabsorption (DCT & collecting duct)
↑ K⁺ excretion
↑ Water retention
│
▼
↑ Blood volume → ↑ CO → ↑ BP
│
└──────────────────────────────────────────────┘
↑ BP (feedback complete)
| Component | Site of Production | Stimulus | Effect |
|---|---|---|---|
| Renin | JGA cells (kidney) | ↓ BP, ↓ Na⁺, ↑ sympathetic | Cleaves angiotensinogen |
| Angiotensin I | Plasma (from liver substrate) | Renin action | Inactive precursor |
| Angiotensin II | Lung, vascular endothelium (ACE) | Ang I conversion | Vasoconstriction, stimulates aldosterone |
| Aldosterone | Adrenal cortex (zona glomerulosa) | Ang II, ↑ K⁺ | ↑ ENaC in collecting duct → Na⁺/water retention |
| ACE inhibitors | - | Drug | Block Ang II formation → ↓ BP |
| ARBs | - | Drug | Block AT1 receptor → ↓ BP |
6C. Antidiuretic Hormone (ADH / Vasopressin)
↓ BP / ↑ Plasma osmolarity
│
▼
Hypothalamic osmoreceptors + Baroreceptors
→ Posterior pituitary releases ADH
│
├─────────────────────────────────┐
▼ ▼
↑ Water reabsorption (V2 receptor) Vasoconstriction (V1 receptor)
in collecting duct → ↑ TPR
│ │
▼ ▼
↑ Blood volume → ↑ CO → ↑ BP Direct pressor effect
6D. Atrial Natriuretic Peptide (ANP) and Brain Natriuretic Peptide (BNP)
These act counter-regulatory to RAAS - they reduce BP when it is too high.
↑ BP → Volume overload
→ Atrial/ventricular wall stretch
│
▼
Cardiomyocytes release ANP (atria) / BNP (ventricles)
│
├─────────────────────────────────┐
▼ ▼
↓ Na⁺ reabsorption in DCT Systemic vasodilation
(inhibit ENaC) → ↓ TPR
→ Natriuresis + diuresis
→ ↓ Blood volume
│
▼
↓ CO + ↓ TPR → ↓ BP
Summary Table: All Three Tiers
| Tier | Mechanism | Onset | Duration | Potency | Key Mediator |
|---|---|---|---|---|---|
| SHORT | Baroreceptor reflex | Seconds | Minutes | High (acute) | Autonomic NS |
| SHORT | Chemoreceptor reflex | Seconds | Minutes | Moderate | CN IX/X |
| SHORT | CNS ischemic response | Seconds | Minutes | Very high | CO₂ |
| INTERMEDIATE | Capillary fluid shift | 10-30 min | 1-4 hrs | ~70% of baro | Hydrostatic pressure |
| INTERMEDIATE | Stress relaxation | Min-hrs | Hrs | Moderate | Vascular smooth muscle |
| INTERMEDIATE | Early RAAS | 20-30 min | Hrs | Moderate | Angiotensin II |
| LONG | Pressure natriuresis | Hrs | Days-lifetime | Infinite gain | Renal Na⁺ excretion |
| LONG | Aldosterone | Hrs-days | Days | High | Aldosterone-ENaC |
| LONG | ADH/Vasopressin | Min-hrs | Hrs-days | Moderate | V1/V2 receptors |
| LONG | ANP/BNP | Min-hrs | Hrs | Moderate | Guanylate cyclase |
7. Master Integrative Flowchart
BLOOD PRESSURE
= Cardiac Output × TPR
│
┌───────────────────┴────────────────────┐
│ │
CARDIAC OUTPUT TOTAL PERIPHERAL
(HR × Stroke Volume) RESISTANCE
│ │
┌──────┴──────┐ ┌─────────────┴──────────┐
│ │ │ │ │
Heart rate Contractility Arteriolar tone Blood Neural
Parasym.↓ Sympathetic↑ RAAS, Catechol. Volume Control
Sympathetic↑ Inotropes NO, PG, Kinins (RAAS) (SNS)
Autoregulation ADH/ANP
8. Key Clinical Correlations
| Clinical Scenario | Mechanism Disrupted | Consequence |
|---|---|---|
| Chronic hypertension | Baroreceptor reset + RAAS | Maintained elevation; end-organ damage |
| Hemorrhagic shock | Loss of volume → baroreceptor + RAAS | Compensatory tachycardia, vasoconstriction |
| Spinal cord injury | Loss of sympathetic outflow | Neurogenic hypotension |
| Heart failure | RAAS activation (maladaptive) | Volume overload; treated with ACEi + aldosterone antagonists |
| Cushing's reflex | ICP-induced ischemic response | Hypertension + bradycardia + irregular respirations |
| Primary hyperaldosteronism (Conn's) | Excess aldosterone → Na⁺ retention | Hypertension + hypokalemia |
Sources:
- Robbins & Kumar Basic Pathology (10th Ed.), Fig. 8.2, 8.3, pp. 309-310
- Costanzo Physiology (7th Ed.), pp. 169-171 - baroreceptor reflex
- Fuster & Hurst's The Heart (15th Ed.), Fig. 5-8 - renal-body fluid feedback
- Medical Physiology (Boron & Boulpaep), p. 796 - chemoreceptor control
This is a shared conversation. Sign in to Orris to start your own chat.