Intrapapillary hydarade noma
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have everything needed for a comprehensive answer.
Hidradenoma Papilliferum (Intrapapillary Hidradenoma)
Also called hidradenoma papilliferum, papillary hidradenoma, or intrapapillary hidradenoma, this is a benign adnexal adenoma with apocrine/mammary-like differentiation.
Definition and Origin
Hidradenoma papilliferum is an adenoma arising from anogenital mammary-like glands (MLAGs) - specialized glands located in the vulvar and perianal skin that share morphological and immunohistochemical features with breast ductal tissue. This explains its close histological resemblance to mammary intraductal papilloma, which is essentially its breast counterpart.
- Robbins Pathologic Basis of Disease, p. 919
- Fitzpatrick's Dermatology, p. 1865
Epidemiology and Clinical Features
- Occurs almost exclusively in females, in the anogenital region (vulva, labia majora, interlabial folds, perianal skin)
- Rare ectopic cases have been reported on the scalp
- Presents as a firm, flesh-colored to red papule or nodule, typically < 1 cm in diameter
- Covered by normal-appearing skin
- May occasionally ulcerate, which can raise concern for carcinoma clinically, but is benign
- Usually solitary
Pathogenesis / Molecular Features
- Classified as an adenoma of MLAGs, morphologically and molecularly similar to breast ductal papillomas
- Activating mutations in PIK3CA (PI3K pathway) and AKT1 identified - the same mutations found in mammary ductal papillomas, reinforcing the shared biology between these entities
- Fitzpatrick's Dermatology, p. 1865
Histopathology
The histology is characteristic:
Architectural features:
- Well-circumscribed, unencapsulated, solid-cystic dermal nodule - no connection to the overlying epidermis (rare exception)
- Complex pattern of interconnected tubules and glands in a labyrinth-like arrangement
- Prominent papillary projections extending into cyst-like cavities lined by "villi"
- The tumour lies wholly within the dermis
Cytology:
- Bilayered epithelium - the hallmark:
- Luminal layer: cuboidal to columnar secretory cells, with decapitation (apocrine) secretion
- Outer layer: flat myoepithelial cells
- Oxyphilic (oncocytic) metaplasia is not uncommon
- Mitotic figures may be seen; proliferative index is variable
- Adjacent remnants of MLAGs in ~1/3 of cases
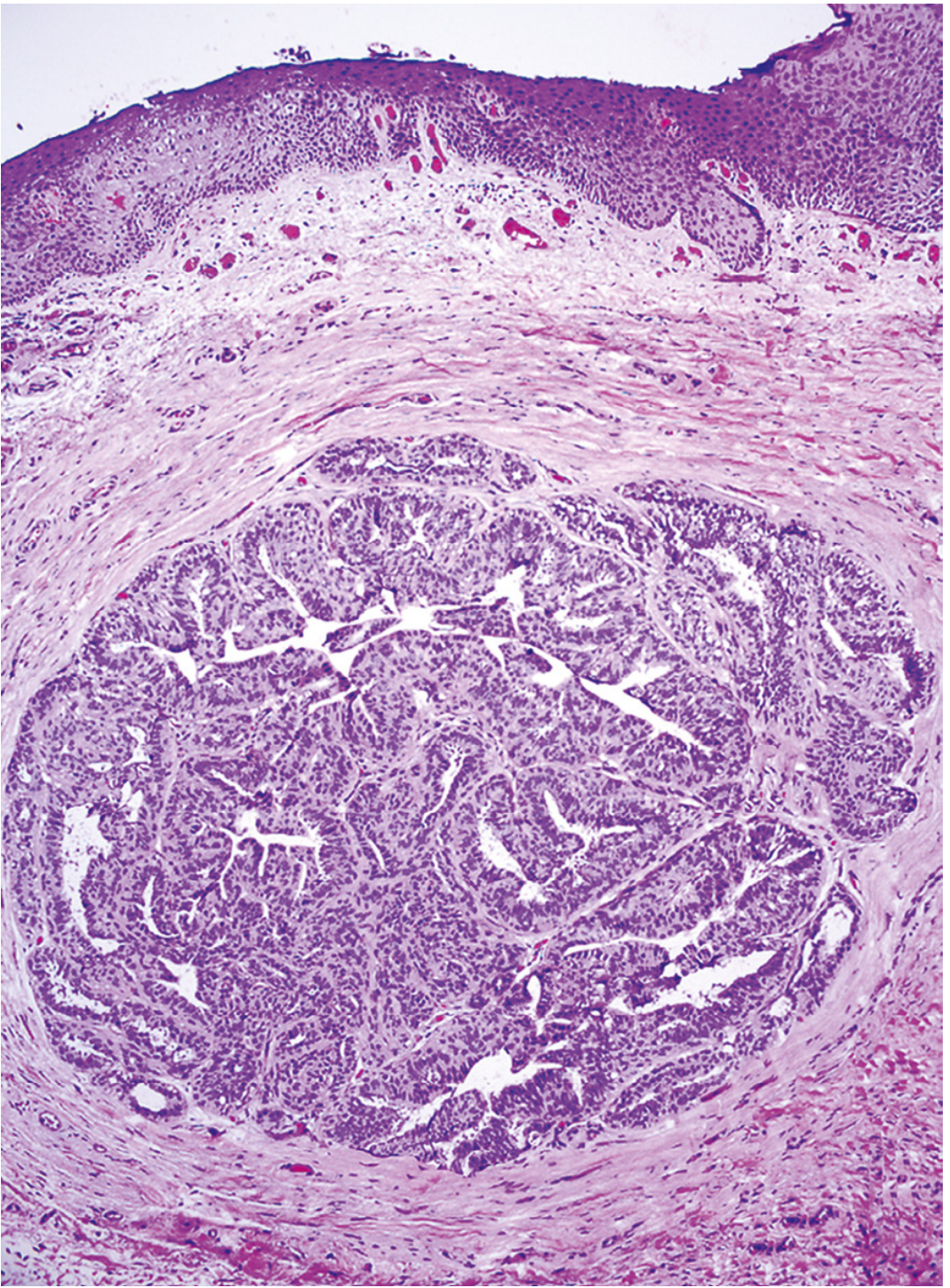
Fig. 22.9 (Robbins) - Papillary hidradenoma of the vulva: well-circumscribed tumor with benign papillary projections covered by columnar secretory epithelium and underlying myoepithelial cells.
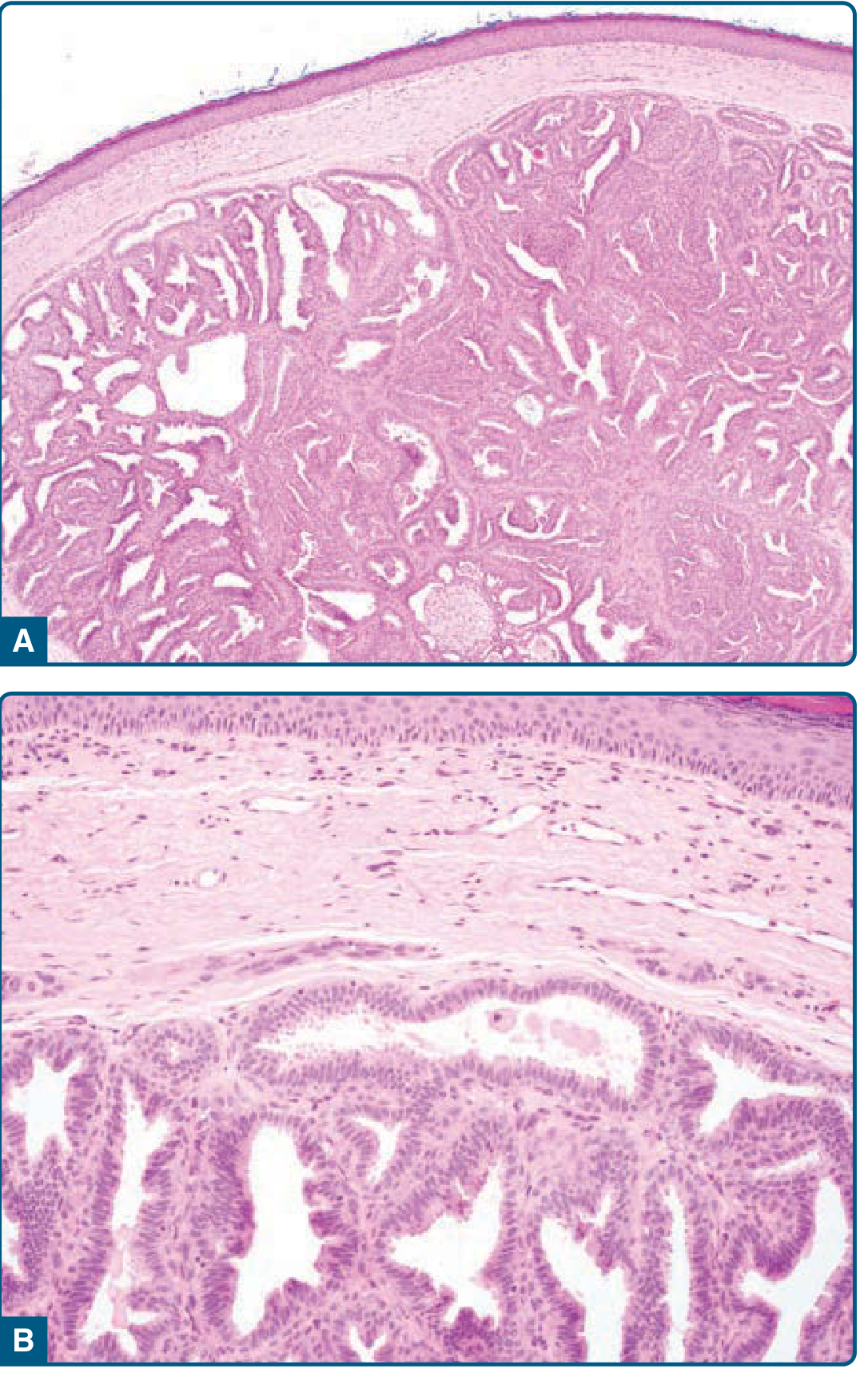
Fig. 109-10 (Fitzpatrick's) - A: well-circumscribed solid-cystic nodule with interconnected glands in a labyrinth-like arrangement; B: bilayered projections with columnar/cuboidal cells showing decapitation secretion and basal myoepithelial layer.
Immunohistochemistry
| Cell type | Markers |
|---|---|
| Luminal epithelial cells | CK5/6, AE1/AE3, GCDFP-15, Estrogen receptors |
| Myoepithelial cells | S100, smooth muscle actin (SMA), calponin, p63 |
The myoepithelial layer is a key diagnostic and prognostic marker - its loss signals malignant transformation.
Differential Diagnosis
| Condition | Distinguishing feature |
|---|---|
| Epidermal/dermoid cyst | No papillary glandular architecture |
| Syringocystadenoma papilliferum | Connection to overlying epidermis; plasma cell-rich stroma; apocrine not MLAG origin |
| Intraductal papilloma of breast | Identical histology but intramammary location |
| Carcinoma (clinical DDx) | Ulceration mimics malignancy, but histology is benign; absence of true invasion |
- Fitzpatrick's Dermatology, p. 1865
- Andrews' Diseases of the Skin, p. 769
Clinical Course, Prognosis, and Management
- Benign in the vast majority of cases
- Rare reports of ductal carcinoma in situ arising within hidradenoma papilliferum (manifested by increased cellularity, nuclear atypia, abnormal mitoses)
- Adenocarcinoma (hidradenocarcinoma papilliferum) arising in this lesion is a controversial but recognized diagnosis
- Loss of the myoepithelial cell layer suggests malignant transformation
- Treatment: Excisional biopsy - both diagnostic and curative
- Andrews' Diseases of the Skin, p. 769; Fitzpatrick's Dermatology, p. 1865
Summary Table
| Feature | Detail |
|---|---|
| Nature | Benign adnexal adenoma |
| Origin | Anogenital mammary-like glands (MLAGs) |
| Location | Vulva/labia majora (almost exclusively female, anogenital) |
| Size | Usually < 1 cm |
| Architecture | Well-circumscribed, intradermal, labyrinthine glands with papillae |
| Epithelium | Bilayered: luminal columnar cells + myoepithelial layer |
| IHC | GCDFP-15+, ER+; myoepithelium: S100, p63, calponin+ |
| Molecular | PIK3CA and AKT1 mutations |
| Breast analogue | Intraductal papilloma |
| Treatment | Excisional biopsy |
| Malignant risk | Rare (DCIS or adenocarcinoma in situ reported) |
This is a shared conversation. Sign in to Orris to start your own chat.