Explain heart failure
Reading File
Finding Sources
Searching PubMed
"heart failure"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have enough rich content to write a comprehensive, authoritative answer. Let me compile the full explanation.
Heart Failure
Definition
Heart failure is a clinical syndrome that results when abnormalities in myocardial structure and function impair cardiac output or decrease filling of the ventricles. The cardinal features are dyspnea, fatigue, impaired exercise performance, and edema. Because congestion is a common but not universal feature, the older term "congestive heart failure" is no longer used. - Goldman-Cecil Medicine, p. 464
Epidemiology
- More than 64 million people worldwide are affected.
- Prevalence is 1-2% of the adult population, with a lifetime risk of 20-45% depending on age, race, and geography.
- It is the leading cause of hospitalization in patients over 65 years.
- Once hospitalized, a patient faces a 25% chance of rehospitalization within 30 days and a 10% risk of 30-day post-discharge mortality.
- Approximately 50% of patients die within 5 years of diagnosis. - Tintinalli's Emergency Medicine, p. 409
Causes / Etiology
Heart failure has numerous causes. In developed countries, coronary artery disease with prior myocardial infarction accounts for nearly 70% of cases. Key causes include: - Goldman-Cecil Medicine, p. 464
| Category | Examples |
|---|---|
| Ischemic | Coronary artery disease, prior MI |
| Pressure/volume overload | Hypertension, valvular stenosis/regurgitation |
| Genetic/familial | Dilated cardiomyopathy, hypertrophic cardiomyopathy, muscular dystrophies |
| Metabolic | Diabetes, obesity, metabolic syndrome |
| Toxic | Chemotherapy (anthracyclines), alcohol, cocaine |
| Infiltrative | Amyloid, sarcoid, hemochromatosis |
| Infectious | Viral myocarditis, Chagas disease (common in South America) |
| Arrhythmia-induced | Tachycardia-mediated cardiomyopathy, PVC-induced cardiomyopathy |
| Immunologic | Immune-mediated myocardial injury |
Classification
Heart failure is classified three complementary ways:
1. By Disease Stage (ACC/AHA, 2022 Guideline)
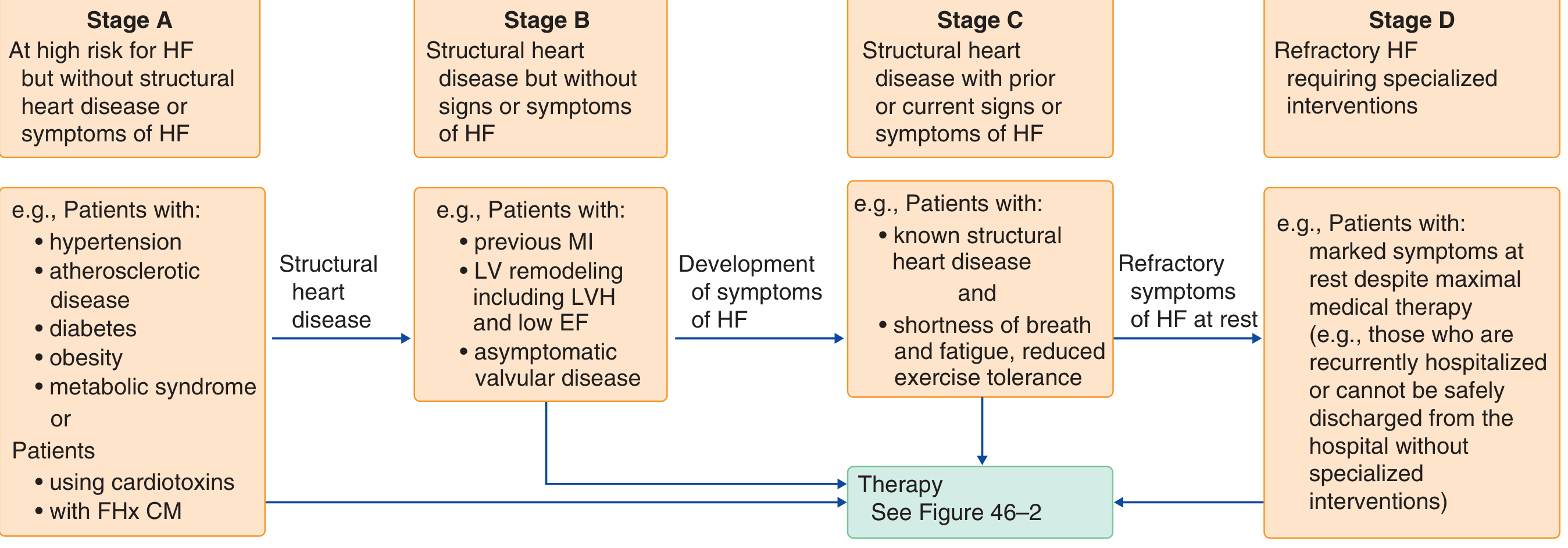
Figure: ACC/AHA Stages A-D of heart failure progression. Modified from the 2022 AHA/ACC/HFSA Guideline. - Goldman-Cecil Medicine
| Stage | Description | Examples |
|---|---|---|
| A | At risk but no structural disease or symptoms | HTN, diabetes, obesity, family history of cardiomyopathy |
| B | Structural disease but no symptoms | Prior MI, LV remodeling, asymptomatic valvular disease |
| C | Structural disease with current or prior symptoms | Dyspnea, fatigue, reduced exercise tolerance |
| D | Refractory HF requiring specialized interventions | Symptoms at rest despite maximal medical therapy |
2. By Ejection Fraction
- HFrEF (Heart failure with Reduced EF): EF <40%
- HFmrEF (Mid-range EF): EF 40-50%
- HFpEF (Preserved EF): EF >50%
Nearly half of all HF patients have a preserved ejection fraction. HFpEF patients tend to be older, more often women, with hypertension and diabetes. Mortality rates are similar between HFrEF and HFpEF. - Goldman-Cecil Medicine, p. 463
3. By Functional Capacity (NYHA Classification)
| Class | Symptoms |
|---|---|
| I | No symptoms with ordinary activity |
| II | Mild symptoms, slight limitation with activity |
| III | Marked limitation; comfortable only at rest |
| IV | Symptoms at rest; any activity causes discomfort |
Pathophysiology
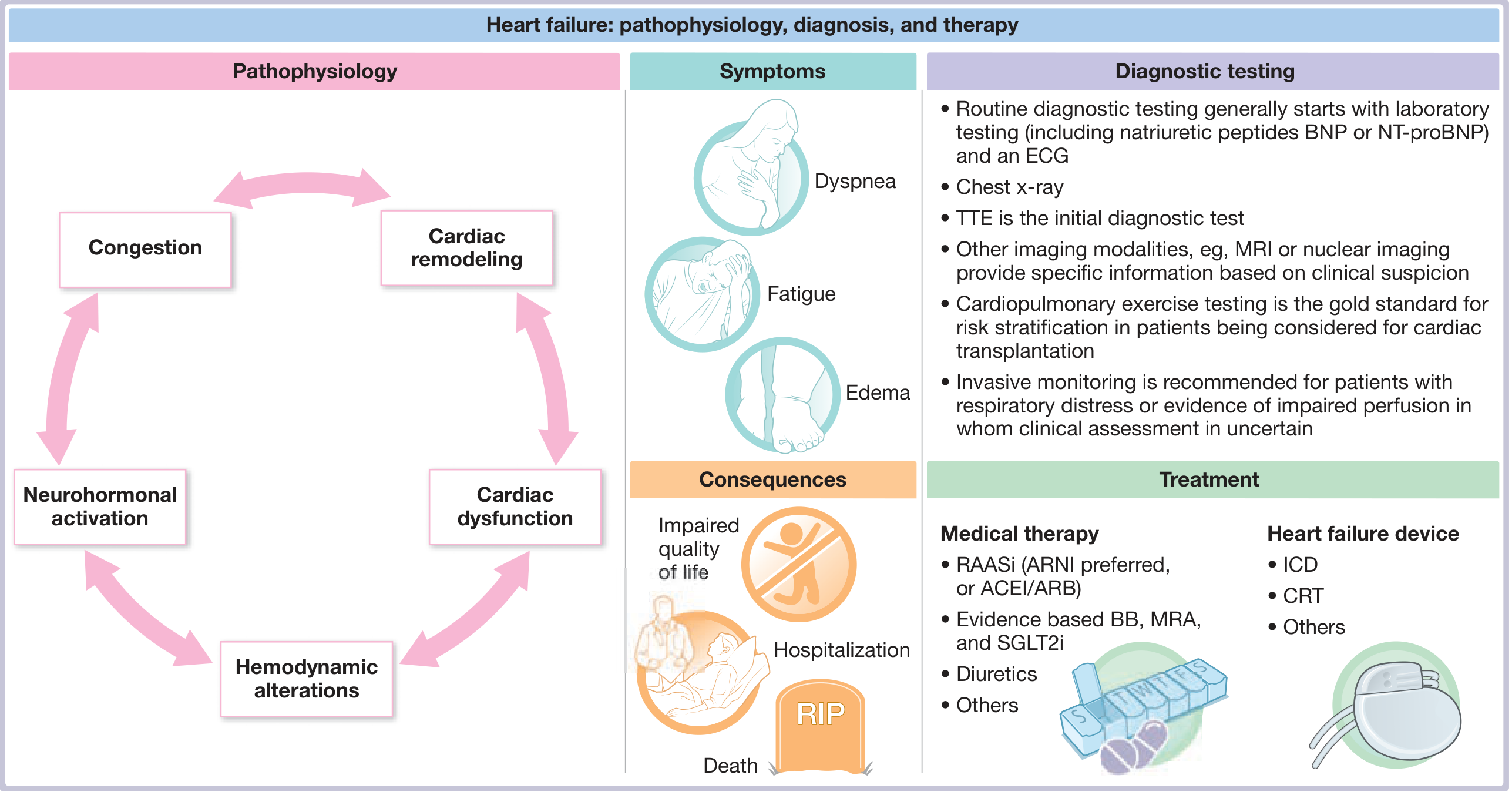
Figure: Comprehensive overview of HF pathophysiology, symptoms, diagnosis and treatment. - Fuster and Hurst's The Heart, 15th Edition
The Core Cascade
When cardiac output drops from myocardial injury or stress, the following sequence occurs:
1. Neurohormonal Activation
- The sympathetic nervous system activates, releasing norepinephrine. Chronically elevated norepinephrine reduces β-adrenergic receptor density on cardiac myocytes, downregulates signaling, and is directly cardiotoxic.
- The renin-angiotensin-aldosterone system (RAAS) activates, causing vasoconstriction and sodium/water retention. This is triggered by renal hypoperfusion, β-adrenergic stimulation, and hyponatremia.
- Additional mediators released: vasopressin, endothelin (potent vasoconstrictor), and TNF-alpha. Elevated levels of these hormones correlate with higher mortality.
2. Hemodynamic Effects
- Sodium and water retention + increased systemic vascular resistance maintain blood pressure and perfusion short-term.
- Long-term, these raise myocardial workload, wall tension, and oxygen demand - worsening dysfunction.
3. Cardiac Remodeling
- The heart undergoes structural changes including hypertrophy, dilation, fibrosis, and altered chamber geometry.
- Alterations in cardiac extracellular matrix and replacement fibrosis impair both systolic and diastolic function.
- Regulatory mediators of fibrosis include aldosterone, matrix metalloproteinases, TNF-alpha, and ST2.
- This remodeling creates a vicious cycle: dysfunction → neurohormonal activation → remodeling → further dysfunction.
4. Counterregulatory Response: Natriuretic Peptides
- ANP (atrial) and BNP (ventricular) are released in response to volume/pressure overload.
- They produce vasodilation, natriuresis, suppress RAAS, and inhibit sympathetic activity.
- BNP is synthesized as NT-proBNP, cleaved into inactive NT-proBNP (half-life ~2 hours) and physiologically active BNP (half-life ~20 minutes). Both are clinically measured. - Tintinalli's Emergency Medicine, p. 409
Left-Sided vs. Right-Sided Heart Failure
- Left-sided HF causes pulmonary venous congestion: dyspnea, orthopnea, paroxysmal nocturnal dyspnea, pulmonary edema.
- Right-sided HF (often secondary to left-sided HF or pulmonary hypertension) causes systemic venous congestion: peripheral edema, hepatomegaly, ascites, jugular venous distension.
Clinical Features
Symptoms:
- Dyspnea (exertional, at rest, orthopnea, PND)
- Fatigue and weakness
- Peripheral edema
- Reduced exercise tolerance
- Cough (especially nocturnal)
- In severe cases: cyanosis, weight loss (cardiac cachexia)
Signs:
- Elevated JVP (jugular venous pressure)
- S3 gallop (pathognomonic of systolic dysfunction)
- Displaced apex beat
- Bibasal crackles (pulmonary edema)
- Peripheral pitting edema
- Hepatomegaly, ascites (right HF)
- Cool peripheries, reduced pulse pressure (low output states)
Diagnosis
Initial workup: - Fuster & Hurst's The Heart, 15th Edition
| Test | Purpose |
|---|---|
| BNP / NT-proBNP | Rule in/out HF; elevated in volume overload |
| ECG | Ischemia, arrhythmias, LVH, bundle branch block |
| Chest X-ray | Cardiomegaly, pulmonary congestion, pleural effusions |
| Transthoracic Echo (TTE) | Primary imaging test - EF, wall motion, valves |
| Blood tests | CBC, renal/electrolytes, LFTs, thyroid, iron studies |
| Cardiopulmonary exercise test | Gold standard for risk stratification before transplant |
| MRI / Nuclear imaging | Myocardial fibrosis, viability, infiltrative disease |
| Right heart catheterization | Invasive monitoring for refractory HF or pre-transplant |
BNP >100 pg/mL or NT-proBNP >300 pg/mL raise concern for HF; very low values (<100 pg/mL BNP) have excellent negative predictive value.
Management
Chronic HF (HFrEF) - Disease-Modifying Therapies
The four pillars of guideline-directed medical therapy (GDMT) for HFrEF:
| Drug Class | Examples | Mechanism |
|---|---|---|
| ARNI (preferred over ACEi/ARB) | Sacubitril/valsartan | Blocks RAAS + enhances natriuretic peptides |
| ACEi / ARB | Enalapril, ramipril / Losartan | RAAS blockade |
| Beta-blockers (evidence-based) | Carvedilol, metoprolol succinate, bisoprolol | Reduces adrenergic toxicity, remodeling |
| MRA (mineralocorticoid receptor antagonist) | Spironolactone, eplerenone | Aldosterone blockade |
| SGLT2 inhibitors | Dapagliflozin, empagliflozin | Cardiorenal protection, reduces HF hospitalizations |
Diuretics (furosemide, torasemide) - relieve congestion but do NOT improve survival.
Device Therapy
- ICD (Implantable Cardioverter-Defibrillator): For EF ≤35% with NYHA Class II-III despite GDMT, to prevent sudden cardiac death.
- CRT (Cardiac Resynchronization Therapy): For EF ≤35% with LBBB and QRS ≥150ms; resynchronizes ventricular contraction.
- LVAD (Left Ventricular Assist Device): For Stage D HF as bridge to transplant or destination therapy.
Acute Decompensated HF
Treatment focuses on rapid symptom relief: - Tintinalli's Emergency Medicine, p. 409
- IV loop diuretics (furosemide) - for decongestion
- Nitrates (IV nitroglycerin) - vasodilation, reduce preload/afterload
- Non-invasive positive pressure ventilation (CPAP/BiPAP) - for respiratory failure
- Oxygen, upright positioning
- Identify and treat the precipitant (e.g., arrhythmia, ACS, infection, medication non-adherence)
Stage D / Refractory HF
- Continuous IV inotropes (dobutamine, milrinone) as palliative or bridge
- LVAD implantation
- Heart transplantation (gold standard for end-stage HF)
- Palliative care when appropriate
Prognosis
Prognosis remains poor. About 50% of patients die within 5 years of diagnosis. Hospitalization marks an inflection point - those hospitalized have significantly higher mortality than matched non-hospitalized patients. Functional class (NYHA) correlates well with prognosis. - Tintinalli's Emergency Medicine
Sources: Goldman-Cecil Medicine International Edition (26th Ed.) | Braunwald's Heart Disease (12th Ed.) | Fuster and Hurst's The Heart (15th Ed.) | Tintinalli's Emergency Medicine | Robbins & Cotran Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.