Pneumonia
"pneumonia" AND "community-acquired"
Pneumonia - A Comprehensive Overview
Definition
- Goldman-Cecil Medicine, p. 992
Epidemiology
- One of the most common serious health conditions and the leading infectious cause of hospitalization and death in the United States
- Accounts for ~7 health care visits/1000 young adults but 96 visits/1000 adults aged 85+
- Hospitalization rates increase exponentially with age: 1-2/1000 in young adults up to ~40/1000 in those 85+ years old
- ~35% of CAP hospitalizations occur in patients with recent health care exposure; ~25% in immunocompromised patients
- Pneumonia peaks in November through March, coinciding with influenza and other respiratory virus seasons
- During the COVID-19 pandemic, SARS-CoV-2 became the leading cause of pneumonia-related death
- Goldman-Cecil Medicine, p. 990-992
Risk Factors
| Category | Examples |
|---|---|
| Demographics | Male sex, extremes of age |
| Lifestyle | Smoking, poor dental hygiene, alcohol use disorder, crowded/institutional living |
| Comorbidities | Malnutrition, chronic lung disease (COPD, bronchiectasis, cystic fibrosis), neurologic disease, dementia, impaired gag reflex |
| Immunosuppression | HIV/AIDS, hematologic malignancy, transplantation, corticosteroids, chemotherapy |
| Medications | Opioids, proton pump inhibitors, corticosteroids |
| Genetic | Cystic fibrosis, common variable immunodeficiency, WBC production defects |
- Goldman-Cecil Medicine, p. 992
Pathobiology
- Immigration - oropharyngeal colonization, aspiration events, supine position, GERD
- Elimination - ciliary function, cough, mucosal immunity
- Relative reproduction rates - altered by local pH, oxygen tension, surfactant, and host immunity
- Goldman-Cecil Medicine; Murray & Nadel's Respiratory Medicine
Causative Organisms
CAP - Pathogens by Setting (IDSA/ATS Classification)
| Setting | Common Pathogens |
|---|---|
| Outpatient, no comorbidities | S. pneumoniae, M. pneumoniae, C. pneumoniae, H. influenzae, respiratory viruses, Legionella |
| Outpatient, with cardiopulmonary disease | All above + DRSP, enteric Gram-negatives, anaerobes (aspiration) |
| Inpatient, with comorbidities | S. pneumoniae (incl. DRSP), H. influenzae, M. pneumoniae, C. pneumoniae, enteric GNRs, Legionella, viruses, anaerobes |
| Severe CAP (ICU), no Pseudomonas risk | S. pneumoniae, Legionella, H. influenzae, enteric GNRs, S. aureus, M. pneumoniae, respiratory viruses |
| Severe CAP (ICU), with Pseudomonas risk | All above + P. aeruginosa |
- Fishman's Pulmonary Diseases, p. 2202
- Typical bacteria (S. pneumoniae, H. influenzae, S. aureus, GNRs) cause up to 30% of cases
- Atypical organisms (Mycoplasma, Chlamydia, Legionella) cause <5% of cases
- Respiratory viruses historically cause 20-30% of cases (dramatically increased during COVID-19)
- No pathogen is confirmed in >50% of cases
Clinical Presentation
- Fever, chills
- Cough (productive or dry)
- Dyspnea
- Pleuritic chest pain
- Sputum production
- Crackles / bronchial breath sounds over consolidation
- Dullness to percussion
- Increased tactile fremitus
- Tachypnea, tachycardia
Severity Assessment
CURB-65 Score
| Criterion | Points |
|---|---|
| Confusion | 1 |
| Urea (BUN >19 mg/dL) | 1 |
| Respiratory rate ≥30/min | 1 |
| Blood pressure (SBP <90 or DBP ≤60 mmHg) | 1 |
| Age 65 or older | 1 |
- Score 0-1: Outpatient management
- Score 2: Short hospitalization or supervised outpatient
- Score 3+: Hospitalization; consider ICU if score ≥4
ATS/IDSA Criteria for Severe CAP (ICU admission)
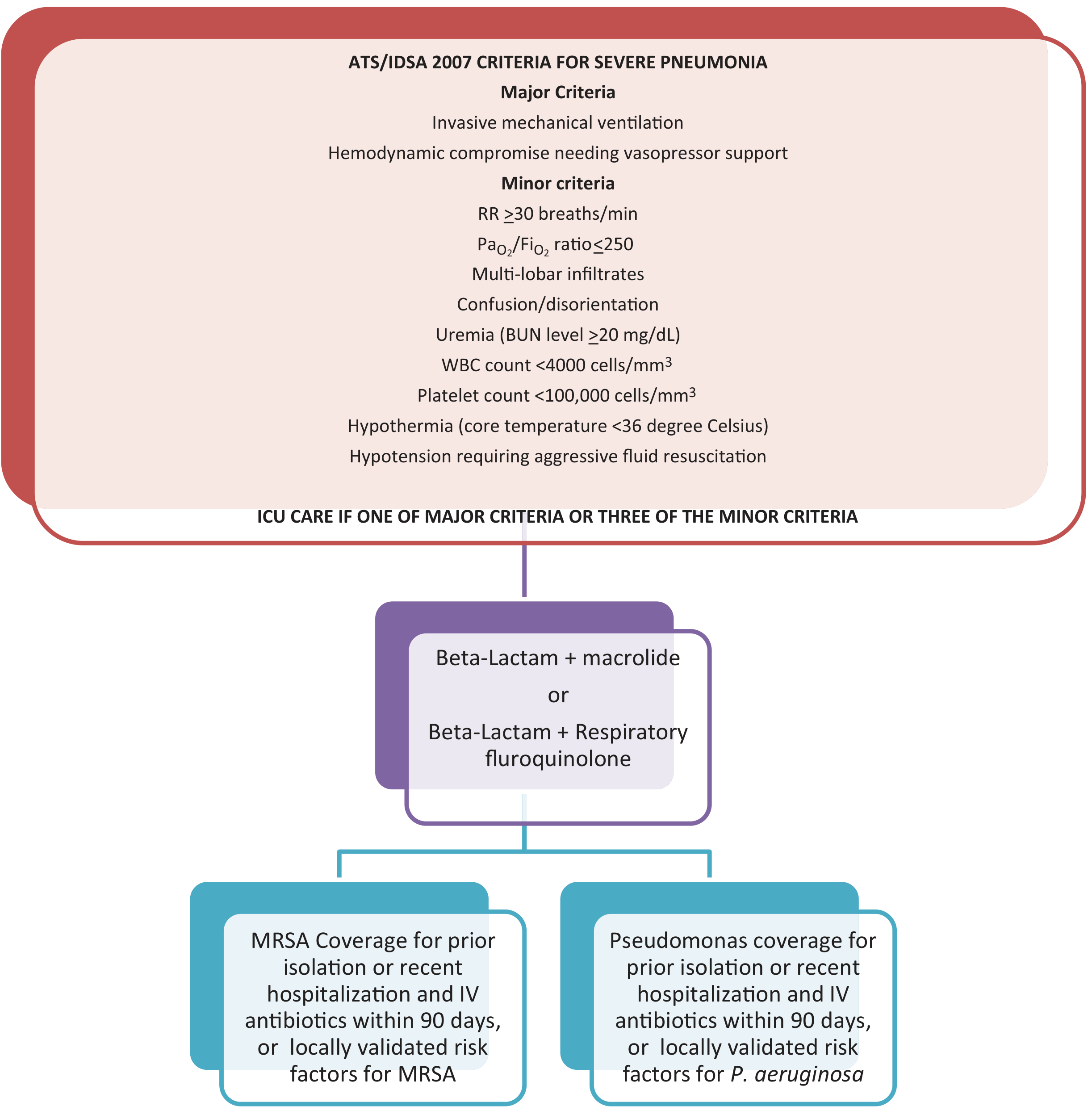
- Invasive mechanical ventilation
- Hemodynamic compromise requiring vasopressor support
-
RR ≥30 breaths/min
-
PaO₂/FiO₂ ratio ≤250
-
Multilobar infiltrates
-
Confusion/disorientation
-
BUN ≥20 mg/dL
-
WBC <4000 cells/mm³
-
Platelet count <100,000 cells/mm³
-
Core temperature <36°C
-
Hypotension requiring aggressive fluid resuscitation
-
Fishman's Pulmonary Diseases, p. 2204
Diagnosis
- Clinical assessment - history and physical examination
- Chest imaging - CXR (lobar consolidation, interstitial infiltrates, pleural effusion); CT chest if CXR equivocal
- Microbiologic studies:
- Blood cultures (before antibiotics in hospitalized patients)
- Sputum Gram stain and culture
- Urine antigen tests (Legionella, S. pneumoniae)
- Multiplex PCR / respiratory panel (including influenza, SARS-CoV-2)
- Procalcitonin: professional societies recommend against using procalcitonin alone to decide whether to give antibiotics
- Laboratory: CBC, BMP (BUN/creatinine), LFTs, ABG (in severe cases)
Treatment
Outpatient (Low Risk, No Comorbidities)
- Amoxicillin
- Doxycycline
- Azithromycin
Outpatient (With Comorbidities / Risk for Resistant Organisms)
- Respiratory fluoroquinolone monotherapy (levofloxacin or moxifloxacin), OR
- Beta-lactam (amoxicillin-clavulanate, cefpodoxime, or cefuroxime) + macrolide or doxycycline
Inpatient, Non-Severe CAP (No MRSA/Pseudomonas Risk)
- Respiratory fluoroquinolone monotherapy, OR
- Beta-lactam + macrolide or doxycycline
Severe CAP (ICU)
- Beta-lactam + macrolide, OR
- Beta-lactam + respiratory fluoroquinolone
- Monotherapy should not be used in ICU patients
- Add MRSA coverage (vancomycin or linezolid) if: prior MRSA isolation, recent hospitalization with IV antibiotics in past 90 days, or locally validated risk factors
- Add Pseudomonas coverage if: prior isolation, recent hospitalization with IV antibiotics in past 90 days, or locally validated risk factors
CA-MRSA Necrotizing Pneumonia
- Linezolid alone, OR
- Vancomycin + clindamycin (to inhibit exotoxin production)
Viral Pneumonia
- Influenza: antivirals (oseltamivir) + empirical antibacterials for possible bacterial coinfection
- SARS-CoV-2: antivirals/monoclonal antibodies; antibacterials only if bacterial coinfection suspected
- Goldman-Cecil Medicine; Fishman's Pulmonary Diseases, p. 2202-2204
Complications
| Complication | Details |
|---|---|
| Empyema | Most common pulmonary complication; ~3-5% of cases; requires drainage |
| Lung abscess | Especially with aspiration or anaerobic organisms |
| Acute cardiac events | Atrial fibrillation, worsening heart failure, MI - develop in 20-25% of hospitalized patients |
| Respiratory failure / ARDS | In severe/bilateral pneumonia |
| Bacteremia / sepsis | 10-15% with streptococcal; higher with Gram-negatives |
| SIADH / hyponatremia | Pneumonia is a recognized cause |
Prognosis
- Mortality for CAP requiring hospitalization: ~6% during hospitalization, ~15% by 1 month
- Recovery can be slow, particularly in older adults
- Cardiac complications contribute significantly to early mortality
Prevention
| Vaccine | Target |
|---|---|
| Pneumococcal vaccine (PCV15, PCV20, PPSV23) | S. pneumoniae - all adults 65+, younger patients with comorbidities |
| Influenza vaccine | Annual; all adults >6 months old |
| COVID-19 vaccine | SARS-CoV-2 pneumonia |
Recent Evidence (2024-2026)
- A 2025 Lancet Respiratory Medicine meta-analysis (PMID 39892408) examined adjuvant corticosteroids in CAP, suggesting that only certain subgroups derive benefit - routine steroid use remains investigational
- A 2025 European Respiratory Review systematic review (PMID 40107661) identified risk factors for drug-resistant pathogens in CAP, supporting selective (rather than empiric broad-spectrum) coverage
- A 2024 Pediatric Pulmonology meta-analysis (PMID 39239917) confirmed lung ultrasound has comparable accuracy to chest radiography for diagnosing CAP in children and may be preferred to avoid radiation
Lobular pneumonia and it's stage
Lobular Pneumonia (Bronchopneumonia) and Stages of Pneumonia
Terminology: Lobular vs. Lobar
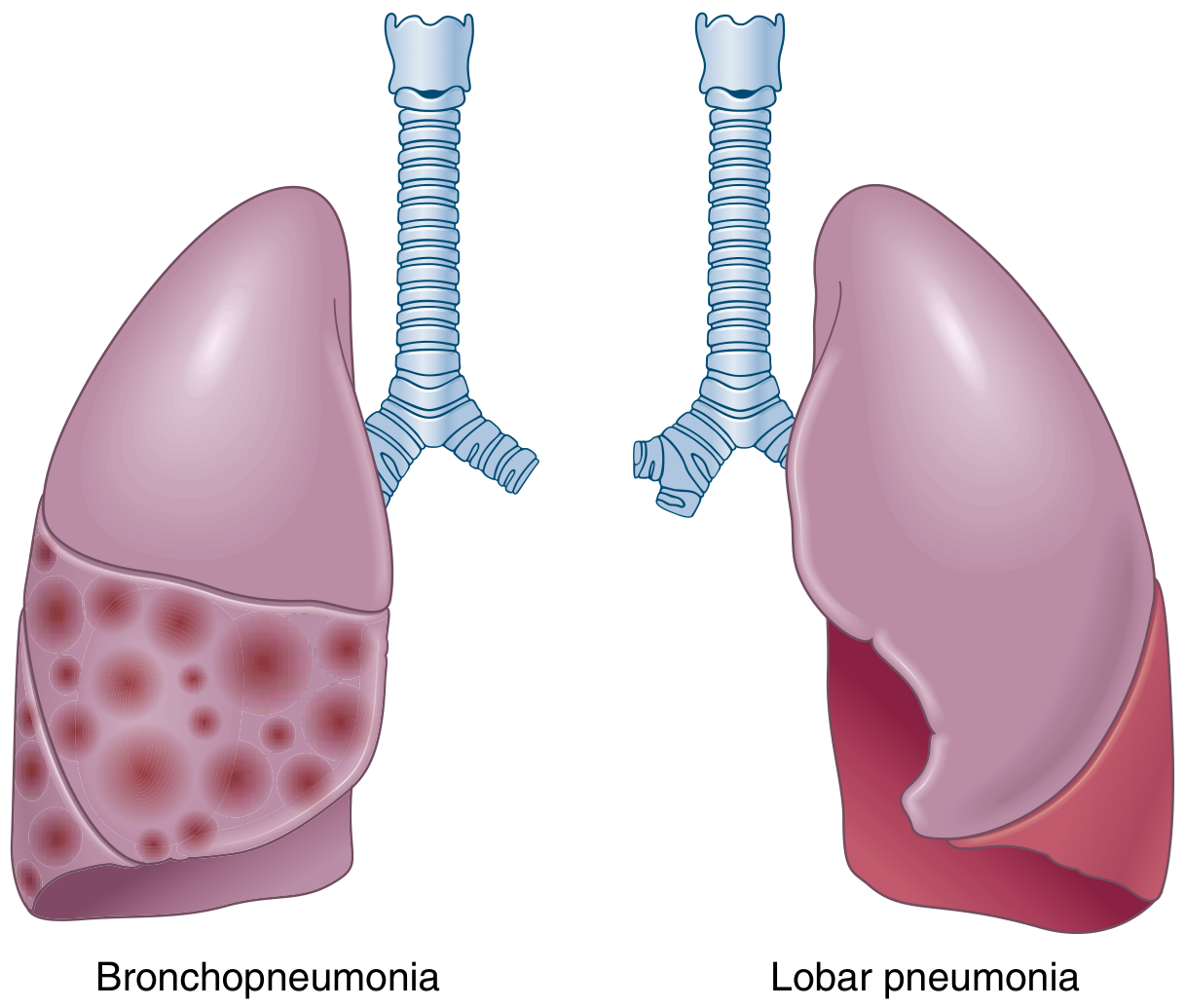
| Feature | Lobular (Broncho)pneumonia | Lobar Pneumonia |
|---|---|---|
| Distribution | Patchy, multifocal, lobular | Entire lobe or large portion of lobe |
| Origin | Bronchioles → surrounding alveoli | Alveoli directly |
| Typical organisms | S. aureus, GNRs, H. influenzae, mixed flora | S. pneumoniae (most common) |
| Laterality | Often bilateral and basal | Usually unilateral |
| Stages | No discrete 4-stage pattern | Classical 4 stages |
| Common setting | Hospital-acquired, aspiration, debilitated patients, elderly, children | Community-acquired in adults |
- Robbins & Kumar Basic Pathology, p. 470; Robbins Cotran & Kumar Pathologic Basis of Disease, p. 662
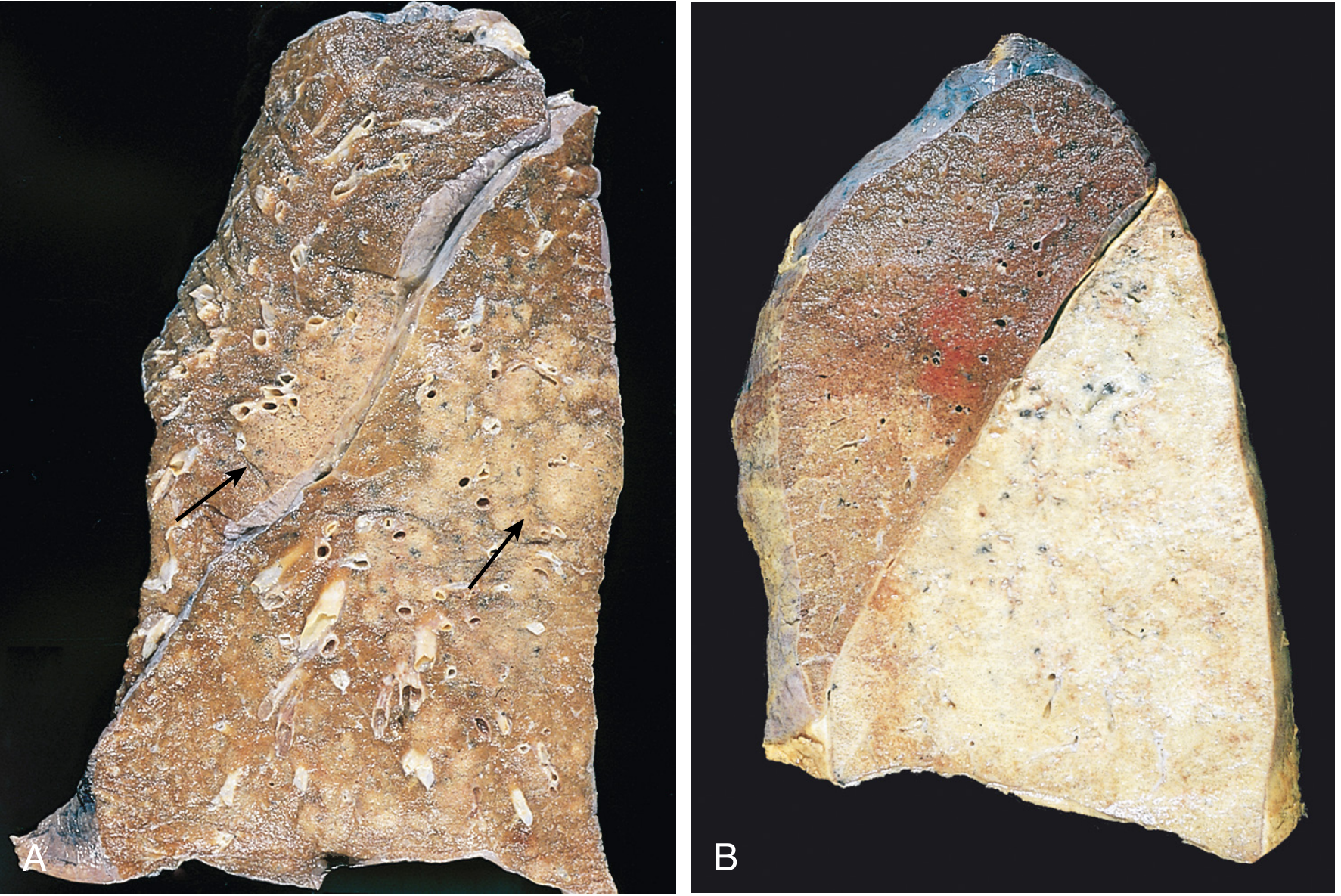
Lobular Bronchopneumonia - Detailed Morphology
Gross Appearance
- Foci of consolidation (acute suppurative inflammation) - often multilobar, bilateral, and basal due to gravitational pooling of secretions
- Lesions are slightly elevated, dry, granular, gray-red to yellow, with poorly defined margins
Microscopic Appearance
- Neutrophil-rich exudate fills the bronchi, bronchioles, and adjacent alveolar spaces
- Centered on bronchioles, spreading outward into surrounding alveoli
- Patchy areas separated by relatively normal lung parenchyma
Key Point
The 4 Classical Stages of Lobar Pneumonia
Stage 1 - Congestion (Days 1-2)
| Feature | Details |
|---|---|
| Gross | Lung is heavy, boggy, and red |
| Micro | Vascular engorgement; intraalveolar edema fluid with few neutrophils |
| Bacteria | Often numerous bacteria present |
| Mechanism | Initial vascular response - the lung fills with protein-rich edema |
Stage 2 - Red Hepatization (Days 2-4)
| Feature | Details |
|---|---|
| Gross | Lobe is red, firm, and airless - liver-like consistency (hence "hepatization") |
| Micro | Massive confluent exudate: neutrophils + red cells + fibrin fill alveolar spaces |
| Bacteria | Still visible |
| Mechanism | Capillary engorgement + RBC diapedesis + fibrin deposition - the erythrocytes give it the red color |
Stage 3 - Gray Hepatization (Days 4-8)
| Feature | Details |
|---|---|
| Gross | Lobe is grayish-brown, still firm |
| Micro | Progressive disintegration of red cells (lysed and degraded); fibrinopurpurative exudate persists; neutrophils dominate |
| Bacteria | Disappear (infection being contained) |
| Mechanism | RBCs are hemolyzed - color changes from red to gray. This stage corresponds to successful containment of infection and improvement in gas exchange |
Stage 4 - Resolution (Days 8 onward)
| Feature | Details |
|---|---|
| Gross | Lung returns toward normal |
| Micro | Exudate undergoes enzymatic digestion → granular, semifluid debris |
| Dominant cell | Macrophages replace neutrophils |
| Fate of debris | Resorbed, ingested by macrophages, expectorated, or organized by fibroblasts |
| Pleura | Fibrinous pleuritis may resolve or leave fibrous thickening/adhesions |
Visual Summary of the 4 Stages
Stage 1: Congestion Stage 2: Red Hepatization
┌─────────────────────┐ ┌─────────────────────────┐
│ Heavy, boggy, RED │ → │ Firm, airless, RED │
│ Vascular engorgement│ │ Neutrophils + RBCs + │
│ Few neutrophils │ │ Fibrin in alveoli │
│ Many bacteria │ │ Liver-like consistency │
└─────────────────────┘ └─────────────────────────┘
Stage 3: Gray Hepatization Stage 4: Resolution
┌─────────────────────┐ ┌─────────────────────────┐
│ Grayish-brown, firm │ → │ Lung re-aerates │
│ RBCs disintegrate │ │ Macrophages dominant │
│ Neutrophils persist │ │ Exudate resorbed or │
│ Bacteria disappear │ │ expelled │
│ Infection contained │ │ ± Pleural adhesions │
└─────────────────────┘ └─────────────────────────┘
Why the 4 Stages Matter Clinically
- Stage 1 (congestion): Radiograph may be normal or show early haziness; patient appears sick but CXR "lags"
- Stage 2 (red hepatization): Classic dense lobar consolidation on CXR; maximum clinical severity
- Stage 3 (gray hepatization): Patient may begin improving clinically; consolidation persists on imaging
- Stage 4 (resolution): Radiographic clearance lags behind clinical recovery by days to weeks - especially in elderly
Important caveat from Harrison's (22e): This 4-stage pattern applies best to lobar pneumococcal pneumonia and may not apply to all etiologies. In ventilator-associated pneumonia (VAP), respiratory bronchiolitis often precedes visible infiltrates. The bronchopneumonia pattern predominates in nosocomial infections, while lobar pattern is more common in bacterial CAP.
Complications (Both Types)
- Lung abscess - tissue destruction and necrosis
- Empyema - spread to pleural cavity → fibrinopurulent intrapleural reaction
- Bacteremic dissemination - seeding of heart valves (endocarditis), brain (meningitis/abscess), joints (septic arthritis), kidneys, pericardium
Aetiopathogenesis of it in diagramatic form
A detailed medical educational diagram titled "Aetiopathogenesis of Lobular (Broncho)pneumonia" showing the complete pathway from etiology to tissue damage. Top section - "PREDISPOSING FACTORS / ETIOLOGY" box with two columns: Left: Host Factors: Extremes of age (infants, elderly), Debilitating illness (COPD, diabetes, malnutrition), Impaired consciousness (seizures, alcohol, anaesthesia), Impaired cough reflex, Ciliary dysfunction (smoking, viral infection), Immunosuppression (chemotherapy, HIV), Post-operative state Right: Causative Organisms: Bacteria: S. aureus, Klebsiella, H. influenzae, Pseudomonas, Streptococcus pyogenes, E. coli; Viruses (precede bacterial infection); Aspiration of gastric/oropharyngeal flora Middle section - "ROUTE OF INFECTION" showing three arrows pointing downward: (1) Inhalation of droplets → upper airway → bronchioles, (2) Aspiration of oropharyngeal/gastric contents, (3) Haematogenous spread (septicaemia) Central pathway box - "BREAKDOWN OF HOST DEFENSES": - Mucociliary escalator impaired - Alveolar macrophage overwhelmed - Surfactant disrupted - IgA secretion reduced Next box - "BACTERIAL COLONISATION OF BRONCHIOLES": - Bacteria adhere to bronchiolar epithelium - Release of toxins and proteases - Activation of complement and cytokines (IL-1, TNF-α, IL-6, IL-8) Next box - "ACUTE INFLAMMATORY RESPONSE": - Neutrophil recruitment and diapedesis - Vascular congestion and oedema - Exudate (neutrophils + fibrin + RBCs) fills bronchioles AND adjacent alveoli - Patchy (lobular) consolidation - centribronchiolar pattern Bottom section splits into two paths: Left path "RESOLUTION (if host defenses adequate)": - Macrophage phagocytosis of debris - Enzymatic digestion of exudate - Re-aeration of lung - Complete recovery Right path "COMPLICATIONS (if overwhelming infection)": - Lung abscess (tissue necrosis) - Empyema (pleural spread) - Bacteraemia / Sepsis - ARDS - Organisation → Fibrosis (carnification) Use a clean white background, blue and red colour scheme for boxes, arrows in dark grey, clear sans-serif font, well-spaced layout with connecting arrows between each step showing the flow.
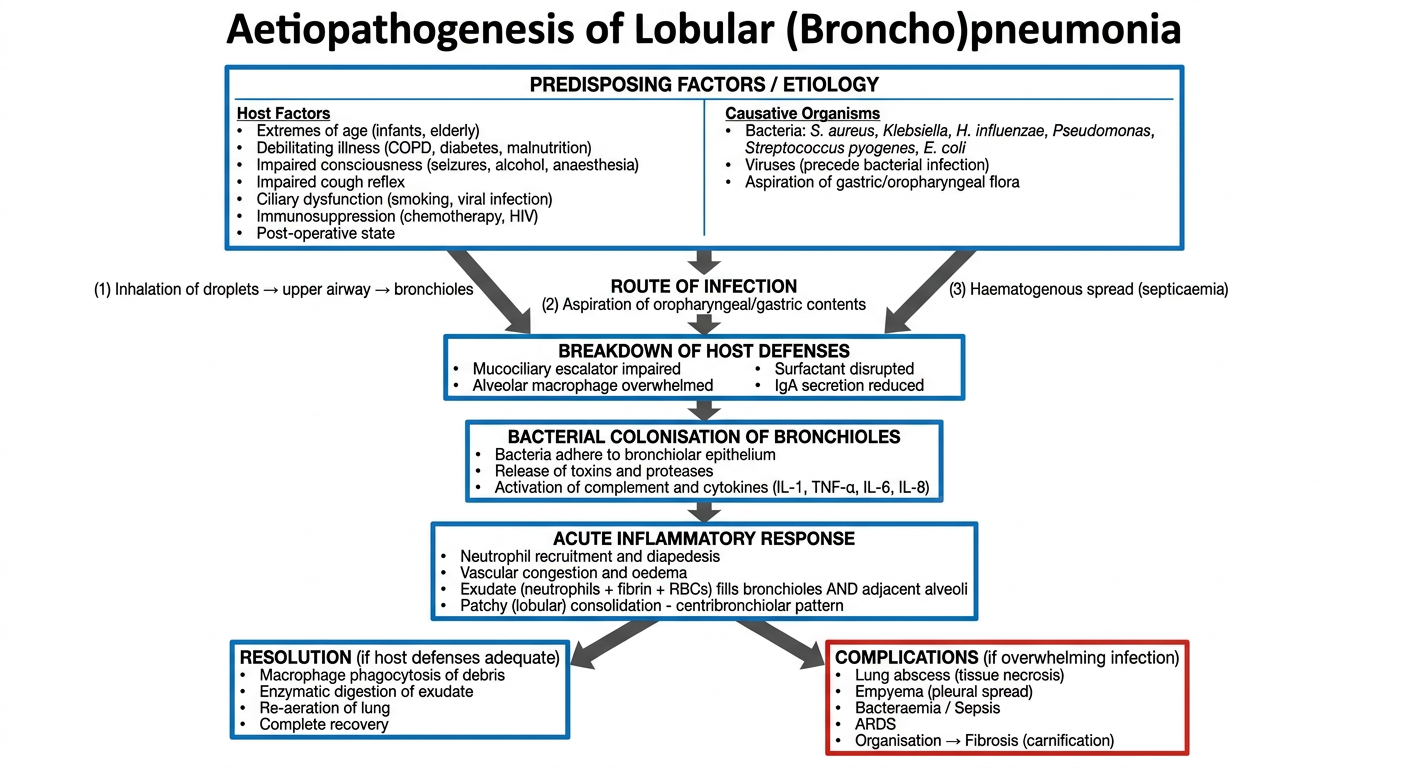
Aetiopathogenesis of Lobular (Bronchopneumonia) - Step by Step
1. Predisposing Factors (Why defences fail)
| Host Factors | Causative Organisms |
|---|---|
| Extremes of age (infants, elderly) | S. aureus, Klebsiella pneumoniae |
| Debilitating illness (COPD, diabetes, malnutrition) | H. influenzae, Pseudomonas aeruginosa |
| Impaired consciousness (alcohol, anaesthesia, seizures) | E. coli, S. pyogenes |
| Smoking / viral infection (ciliary damage) | Mixed oropharyngeal flora (aspiration) |
| Immunosuppression (HIV, chemotherapy) | Viruses precede and predispose to secondary bacterial infection |
| Post-operative state |
2. Routes of Infection
- Inhalation of contaminated droplets → upper airway → bronchioles
- Aspiration of oropharyngeal / gastric contents (most important in bronchopneumonia)
- Haematogenous spread from a distant septic focus
3. Breakdown of Host Defences
- Mucociliary escalator impaired → bacteria not cleared upward
- Alveolar macrophages overwhelmed by bacterial load
- Surfactant disrupted → bacterial adhesion increases
- Secretory IgA reduced → less neutralisation
4. Bacterial Colonisation of Bronchioles
- Organisms adhere to bronchiolar epithelium
- Toxins and proteases released → epithelial damage
- Complement activated → IL-1, TNF-α, IL-6, IL-8 cytokine storm
5. Acute Inflammatory Response (the Pathological Core)
- Massive neutrophil recruitment via chemokines
- Vascular congestion and oedema
- Exudate (neutrophils + fibrin + RBCs) floods bronchioles and adjacent alveoli
- This produces the characteristic patchy, centribronchiolar (lobular) consolidation - multilobar, bilateral, basal
This is why bronchopneumonia does NOT go through the 4 hepatization stages - inflammation is centred on bronchioles, patchy, and does not flood an entire lobe in one continuous wave.
6. Outcomes
- Macrophages phagocytose debris
- Enzymatic digestion of exudate
- Re-aeration → complete recovery
- Lung abscess - necrosis by proteases and toxins (especially S. aureus, Klebsiella)
- Empyema - spread through visceral pleura
- Bacteraemia / Sepsis - haematogenous dissemination
- ARDS - bilateral alveolar flooding, respiratory failure
- Carnification - organisation of exudate by fibroblasts → permanent fibrosis (failed resolution)
Same of lobar pneumonia
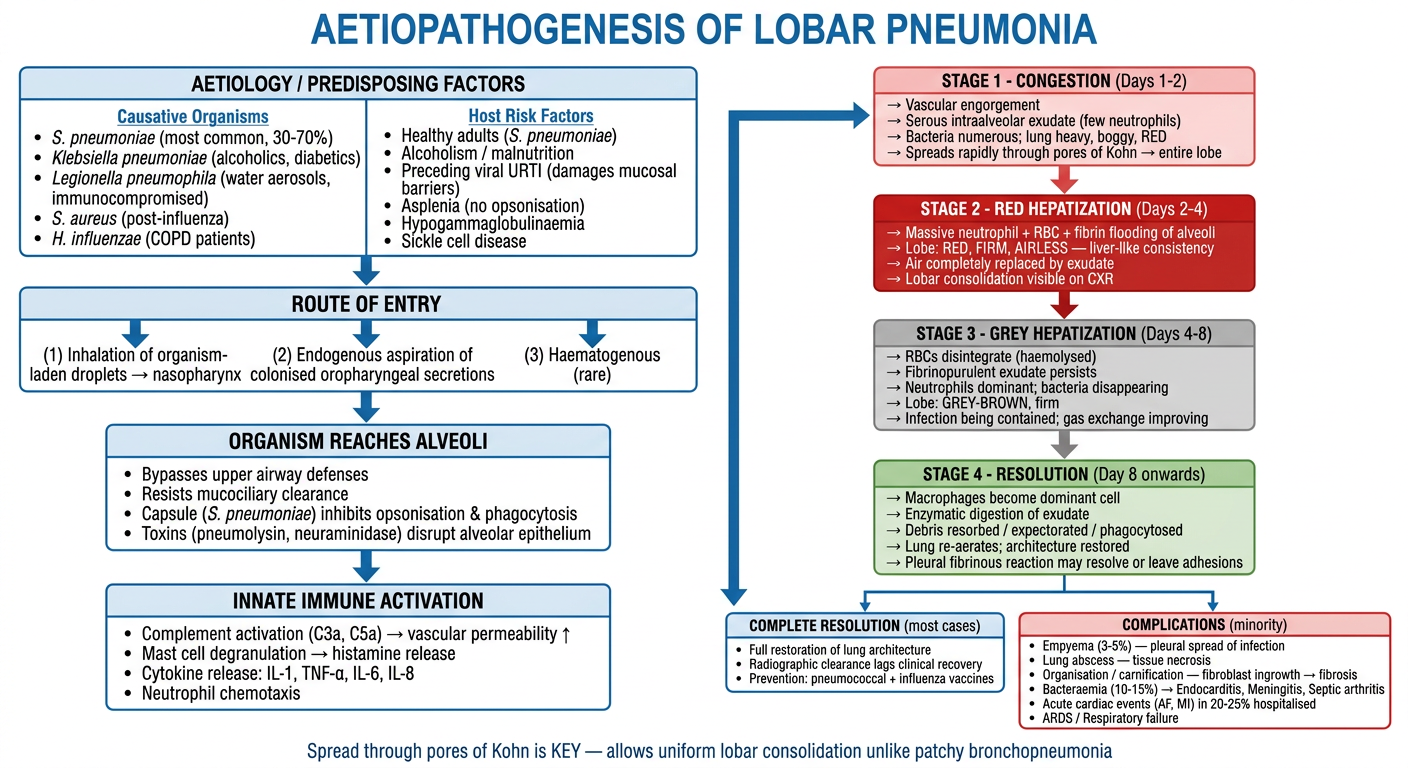
A detailed, clean medical educational flowchart diagram titled "Aetiopathogenesis of Lobar Pneumonia" on a white background with a professional blue and red colour scheme. TOP SECTION - Wide box titled "AETIOLOGY / PREDISPOSING FACTORS" split into two columns: Left column "Causative Organisms": - S. pneumoniae (most common, 30-70%) - Klebsiella pneumoniae (alcoholics, diabetics) - Legionella pneumophila (water aerosols, immunocompromised) - S. aureus (post-influenza) - H. influenzae (COPD patients) Right column "Host Risk Factors": - Healthy adults (S. pneumoniae) - Alcoholism / malnutrition - Preceding viral URTI (damages mucosal barriers) - Asplenia (no opsonisation) - Hypogammaglobulinaemia - Sickle cell disease SECOND BOX - "ROUTE OF ENTRY": Three arrows: (1) Inhalation of organism-laden droplets → nasopharynx, (2) Endogenous aspiration of colonised oropharyngeal secretions, (3) Haematogenous (rare) THIRD BOX - "ORGANISM REACHES ALVEOLI" with sub-points: - Bypasses upper airway defenses - Resists mucociliary clearance - Capsule (S. pneumoniae) inhibits opsonisation & phagocytosis - Toxins (pneumolysin, neuraminidase) disrupt alveolar epithelium FOURTH BOX - "INNATE IMMUNE ACTIVATION": - Complement activation (C3a, C5a) → vascular permeability ↑ - Mast cell degranulation → histamine release - Cytokine release: IL-1, TNF-α, IL-6, IL-8 - Neutrophil chemotaxis Then a CENTRAL VERTICAL PATHWAY showing the 4 STAGES OF LOBAR PNEUMONIA with distinct coloured boxes connected by downward arrows: STAGE 1 - "CONGESTION (Days 1-2)" [light pink box]: → Vascular engorgement → Serous intraalveolar exudate (few neutrophils) → Bacteria numerous; lung heavy, boggy, RED → Spreads rapidly through pores of Kohn → entire lobe STAGE 2 - "RED HEPATIZATION (Days 2-4)" [red box, white text]: → Massive neutrophil + RBC + fibrin flooding of alveoli → Lobe: RED, FIRM, AIRLESS — liver-like consistency → Air completely replaced by exudate → Lobar consolidation visible on CXR STAGE 3 - "GREY HEPATIZATION (Days 4-8)" [grey box]: → RBCs disintegrate (haemolysed) → Fibrinopurulent exudate persists → Neutrophils dominant; bacteria disappearing → Lobe: GREY-BROWN, firm → Infection being contained; gas exchange improving STAGE 4 - "RESOLUTION (Day 8 onwards)" [green box]: → Macrophages become dominant cell → Enzymatic digestion of exudate → Debris resorbed / expectorated / phagocytosed → Lung re-aerates; architecture restored → Pleural fibrinous reaction may resolve or leave adhesions BOTTOM SECTION splits into two outcome boxes: Left box "COMPLETE RESOLUTION (most cases)": - Full restoration of lung architecture - Radiographic clearance lags clinical recovery - Prevention: pneumococcal + influenza vaccines Right box "COMPLICATIONS (minority)": - Empyema (3-5%) — pleural spread of infection - Lung abscess — tissue necrosis - Organisation / carnification — fibroblast ingrowth → fibrosis - Bacteraemia (10-15%) → Endocarditis, Meningitis, Septic arthritis - Acute cardiac events (AF, MI) in 20-25% hospitalised - ARDS / Respiratory failure Use clean sans-serif fonts, clearly labelled boxes, smooth downward arrows between stages, colour-coded stage boxes (pink → red → grey → green), and a note at the bottom: "Spread through pores of Kohn is KEY — allows uniform lobar consolidation unlike patchy bronchopneumonia"
Aetiopathogenesis of Lobar Pneumonia - Detailed Walkthrough
Step 1 - Aetiology
| Organism | Typical Host |
|---|---|
| S. pneumoniae (most common, 30-70%) | Otherwise healthy adults |
| Klebsiella pneumoniae | Alcoholics, diabetics, malnourished |
| Legionella pneumophila | Immunocompromised, water aerosol exposure |
| S. aureus | Post-influenza (secondary bacterial) |
| H. influenzae | Patients with COPD |
Step 2 - Route of Entry & Why Defences Fail
- Organism-laden droplets inhaled → reach alveoli
- S. pneumoniae polysaccharide capsule is the master virulence factor - it resists opsonisation and phagocytosis by alveolar macrophages
- Pneumolysin and neuraminidase disrupt alveolar epithelium
- Once one alveolus is seeded, the organism spreads rapidly to the entire lobe through the pores of Kohn (inter-alveolar communications) - this is what makes lobar pneumonia LOBAR, unlike the centribronchiolar spread of bronchopneumonia
Step 3 - Innate Immune Activation
- Complement activated → C3a, C5a → vascular permeability increases
- IL-1, TNF-α, IL-6, IL-8 released → systemic fever, acute phase response
- Massive neutrophil chemotaxis begins
Step 4 - The 4 Morphological Stages
| Stage | Timing | Gross | Microscopy | Key Event |
|---|---|---|---|---|
| Congestion | Days 1-2 | Heavy, boggy, red | Vascular engorgement; oedema fluid, few neutrophils; many bacteria | Initial vascular flooding |
| Red Hepatization | Days 2-4 | Red, firm, airless - liver consistency | Neutrophils + RBCs + fibrin pack alveoli | Complete air replacement; peak consolidation on CXR |
| Grey Hepatization | Days 4-8 | Grey-brown, still firm | RBCs lysed and gone; fibrinopurulent exudate; neutrophils dominant; bacteria disappear | Infection contained; gas exchange begins improving |
| Resolution | Day 8+ | Re-aerating | Macrophages dominant; exudate enzymatically digested; debris phagocytosed or expectorated | Full architectural restoration |
The Critical Difference from Bronchopneumonia
Pores of Kohn allow the exudate to spread continuously from alveolus to alveolus across an entire lobe, producing uniform lobar consolidation. In bronchopneumonia, spread is centribronchiolar and patchy - the pores are not the primary route.
Step 5 - Outcomes
- Empyema - pleural spread (~3-5%)
- Lung abscess - necrosis (more common with Klebsiella, type 3 pneumococcus)
- Carnification - failed resolution → fibroblasts organise the exudate → permanent fibrosis
- Bacteraemia (10-15%) → endocarditis, meningitis, septic arthritis
- Acute cardiac events (AF, MI, worsening heart failure) in ~20-25% of hospitalised patients
- ARDS in severe/bilateral disease