Breifly explain paracrine driven vasoconstriction
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
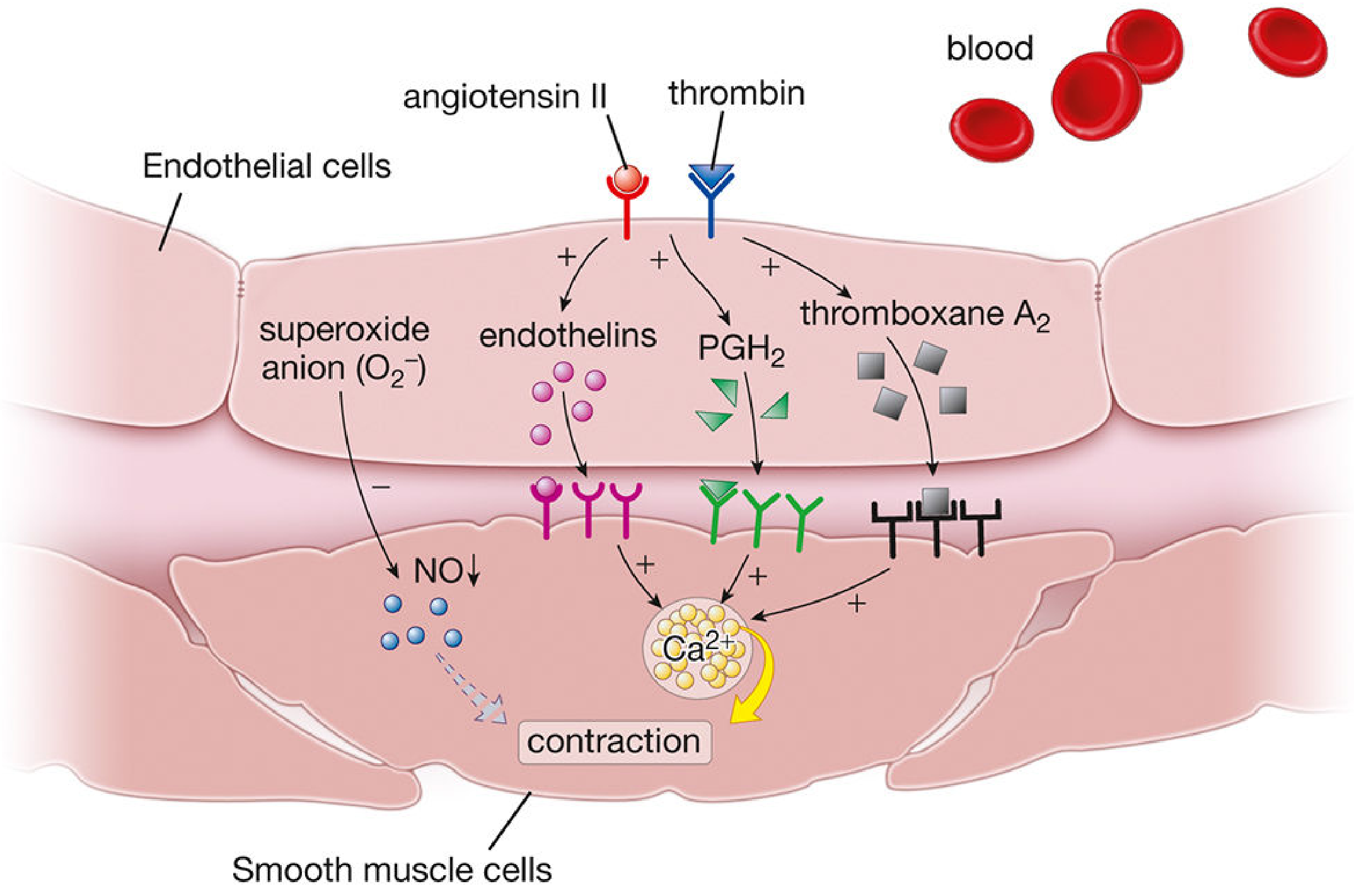
Paracrine-Driven Vasoconstriction
Paracrine signaling refers to locally secreted chemical mediators that act on nearby cells — in this context, substances released by vascular endothelial cells (or platelets) that act on adjacent vascular smooth muscle cells (VSMCs) to cause contraction and narrowing of the vessel lumen.
Key Paracrine Vasoconstrictors
1. Endothelins (ET-1, ET-2, ET-3)
The most potent endogenous vasoconstrictors. Produced by vascular endothelial cells, they are secreted locally and act in a paracrine (and autocrine) fashion rather than as circulating hormones. ET-1 is the dominant isoform.
- Stimulus: Angiotensin II, thrombin, shear stress, hypoxia, and inflammatory cytokines trigger endothelin synthesis.
- Receptor: ET-1 binds ET
Areceptors on VSMCs → activates Gq → ↑IP₃ → ↑intracellular Ca²⁺ → MLCK activation → smooth muscle contraction. - Clinical relevance: Pathologically elevated ET-1 contributes to systemic hypertension, pulmonary arterial hypertension, atherosclerosis, congestive heart failure, and renal failure. — Histology: A Text and Atlas, p. 1083–1084
2. Thromboxane A₂ (TXA₂)
A prostanoid (eicosanoid) synthesized from prostaglandin H₂ (PGH₂). Released primarily by activated platelets, TXA₂ acts paracrinely on adjacent VSMCs to cause contraction — a key mechanism linking platelet activation to local vasoconstriction at sites of vascular injury.
- Also produced by endothelial cells themselves under pathological conditions.
- Acts via thromboxane-prostanoid (TP) receptors → ↑Ca²⁺ → VSMC contraction. — Basic Medical Biochemistry, p. 1143
3. Prostaglandin H₂ (PGH₂)
The precursor to TXA₂; itself a vasoconstrictor that binds TP receptors on VSMCs. Its vasoconstrictive effect is normally balanced by the vasodilatory prostacyclin (PGI₂) released from endothelial cells. — Histology: A Text and Atlas, p. 1084
4. Reactive Oxygen Species / Superoxide (O₂⁻)
Superoxide anion produced under conditions like insulin resistance or inflammation scavenges nitric oxide (NO), reducing its bioavailability and removing a key vasodilatory brake — indirectly promoting net vasoconstriction. — Harrison's Principles, p. 217
5. Serotonin (from Platelets)
Serotonin released by aggregating platelets acts paracrinely on smooth muscle cells of pulmonary arteries to cause vasoconstriction, proliferation, and mitogenesis — a mechanism particularly relevant in pulmonary arterial hypertension (PAH). — Braunwald's Heart Disease
Downstream Mechanism (Final Common Pathway)
All paracrine vasoconstrictors ultimately converge on ↑intracellular Ca²⁺ in VSMCs:
Ca²⁺ → binds calmodulin (CaM) → activates myosin light-chain kinase (MLCK) → phosphorylates myosin light chain (MLC) → cross-bridge cycling → smooth muscle contraction
Summary Table
| Mediator | Source | Receptor on VSMC | Effect |
|---|---|---|---|
| Endothelin-1 (ET-1) | Endothelial cells | ET | ↑Ca²⁺ → contraction |
| Thromboxane A₂ | Platelets / endothelium | TP | ↑Ca²⁺ → contraction |
| PGH₂ | Endothelium | TP | ↑Ca²⁺ → contraction |
| Serotonin | Platelets | 5-HT₂ | Contraction + proliferation |
| O₂⁻ (superoxide) | Endothelium / NADPH oxidase | Indirect (↓NO) | Removes vasodilatory brake |

Explain this text and the graph simply and easily please
Glucose Reabsorption in the Kidney — Simple Explanation
The Basic Idea
Your kidneys filter your blood constantly. Normally, all the glucose that gets filtered is pulled back into the body — none is wasted in the urine. This happens in the proximal convoluted tubule (PCT) using special transporters that grab glucose alongside sodium (Na⁺/glucose cotransport).
The Graph — What's Being Shown
The graph tracks what happens to filtered glucose as blood sugar rises:
| Line | What It Means |
|---|---|
| Filtered (red, straight) | How much glucose the kidney filters — rises linearly with blood sugar |
| Reabsorbed (blue dashed) | How much is pulled back into the body |
| Excreted (red dashed) | How much spills into the urine |
Step by Step
At normal blood sugar (60–120 mg/dL):
- All filtered glucose is reabsorbed. Zero glucose in urine. The "Excreted" line is flat at zero.
At ~200 mg/dL (Renal Threshold):
- Blood sugar is high enough that the transporters start getting overwhelmed.
- Glucose begins spilling into the urine → this is called glucosuria.
- This is a key clinical sign of diabetes mellitus.
At 375 mg/min transport rate (Tm~):
- All transporters are completely full (saturated) — they can't reabsorb any more.
- This maximum capacity is called T
m(transport maximum). - Beyond this point, any extra filtered glucose goes straight into the urine.
The "Splay" Phenomenon
You'd expect the threshold to be a sharp corner on the graph — but it's actually a gradual curve. This is the "splay."
Why? Because not all nephrons are identical — each one has a slightly different Tm. Some get saturated earlier, some later. So glucose starts leaking into the urine gradually, not all at once.
Think of it like a row of buckets of different sizes — the small ones overflow first, then the larger ones follow.
Special Situations
Pregnancy:
- The kidneys filter MORE blood (↑ GFR), so more glucose gets filtered.
- The transporters get overwhelmed even at normal blood sugar → glucosuria in pregnancy doesn't necessarily mean diabetes.
SGLT2 Inhibitors (e.g., dapagliflozin, empagliflozin — the "-flozin" drugs):
- These drugs deliberately block the glucose transporters.
- Result: glucose spills into the urine even when blood sugar is below 200 mg/dL.
- Used as a treatment for type 2 diabetes to lower blood sugar, and also have proven heart and kidney benefits.
One-Line Summary
The kidney normally reclaims all filtered glucose, but when blood sugar exceeds ~200 mg/dL the transporters are overwhelmed and glucose appears in the urine — a sign exploited both clinically (diabetes diagnosis) and therapeutically (SGLT2 inhibitors).
This is a shared conversation. Sign in to Orris to start your own chat.