"External Nasal Deformities" ENT essay answer with Diagrams under 1000 words
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
external nasal deformity saddle nose twisted nose types
Reading File
Searching Images
nasal anatomy external nose bones cartilage diagram
Reading File
Loading Image
Loading Image
Loading Image
Here is the complete essay:
External Nasal Deformities
Introduction
External nasal deformities encompass a spectrum of structural abnormalities affecting the bony and cartilaginous framework of the nose that produce visible cosmetic and/or functional impairment. They may arise from trauma, congenital anomalies, systemic disease, or iatrogenic causes following prior rhinoplasty. Correction requires a thorough preoperative analysis integrating observation, palpation, photography, and radiological assessment before planning septorhinoplasty.
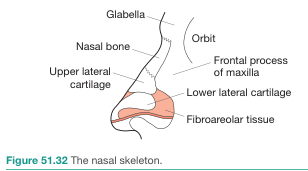
Surgical Anatomy of the External Nose
The external nose is supported by a three-part skeleton:
| Region | Structures |
|---|---|
| Upper third (bony vault) | Paired nasal bones + frontal process of maxilla |
| Middle third (middle vault) | Upper lateral cartilages (ULC) + dorsal septum |
| Lower third (tip & alar lobule) | Lower lateral cartilages (LLC) — medial & lateral crura |

Classification of External Nasal Deformities
1. Traumatic Nasal Deformity
The most common cause. Nasal trauma displaces nasal bones, the external nasal cartilages, or the septum. Isolated nasal deformity results from displacement of the nasal bones, external nasal cartilages, or the septum. Nasal bones can often be repositioned with closed reduction if performed within 2 weeks of injury. Delayed or comminuted fractures require open septorhinoplasty.
2. The Twisted (Crooked) Nose
The twisted nose involves deviation at the bony vault, middle vault, or tip — or all three levels simultaneously. The septum must be straightened to correct a severely twisted nasal deformity; the external approach (open rhinoplasty) is almost universally employed for the twisted nose.
Key surgical manoeuvres:
- Septoplasty — straightening the dorsal and caudal struts
- Spreader grafts — to stabilise the middle vault and widen the internal nasal valve
- Batten grafts — correct internal and external nasal valve collapse
- Osteotomies — to reposition a deviated bony pyramid
- Caudal septal repositioning with draw sutures and anterior spine fixation
3. Saddle Nose Deformity
Characterised by depression of the nasal dorsum (loss of the normal convex profile) due to collapse of the cartilaginous or bony nasal framework.

Causes:
- Trauma (septal haematoma → avascular necrosis)
- Iatrogenic (over-resection of dorsal septum)
- Infections — syphilis, leprosy, tuberculosis
- Granulomatous disease — Granulomatosis with Polyangiitis (GPA/Wegener's)
- Congenital (e.g., failed septal support)
Surgical correction:
Augmentation is the mainstay. Preferred autogenous materials in order of preference:
- Septal cartilage — first choice
- Auricular cartilage
- Costal (rib) cartilage — for large defects
- Bone grafts (iliac crest, calvarial) — for bony defects
- Alloplastic implants (Gore-Tex, Silastic) — if autologous unavailable
4. Cleft Lip Nasal Deformity
A congenital deformity with distinct features:
| Type | Features |
|---|---|
| Unilateral | Tip and columella deviated to noncleft side; cleft nostril wider; nasal floor widened |
| Bilateral | Short columella deviated to less involved side; bifid, poorly defined tip; alar base displaced laterally, posteriorly, and inferiorly |
Surgical goal: improve symmetry of nasal tip and base, and restore nasal airway. The LLC is freed of both surface and vestibular skin and rotated medially to project the tip (Millard technique).
5. Non-Caucasian Nose
A recognised anatomical variant requiring specialised surgical approach. Characteristics: thick skin, weak cartilage, flat/broad dorsum, underprojected and poorly defined tip, wide alar base. Augmentation rhinoplasty with structural grafting is usually required rather than reduction techniques.
6. Hump Nose (Dorsal Hump Deformity)
An excess convexity of the nasal dorsum, predominantly at the osseocartilaginous junction. The nasofrontal angle can be modified to shorten or lengthen the apparent nasal dorsum. Correction involves dorsal hump reduction followed by osteotomies to close the open roof deformity.
Surgical Approach
| Approach | Indication |
|---|---|
| Closed (endonasal) | Mild deformities, limited tip work |
| Open (external/decorticate) | Twisted nose, revision rhinoplasty, cleft nose, implant placement, severe asymmetries |
The external approach is preferred when severe asymmetries, deviations, and tissue deficiencies are evident, as it provides superior exposure and opportunity for precise graft placement. — Cummings Otolaryngology, Chapter 32
Summary
External nasal deformities are classified by aetiology and anatomical level of involvement. A combined septorhinoplasty that corrects both internal and external nasal deformities in one stage is the ideal strategy. The surgeon must master a variety of grafting, osteotomy, and suturing techniques to address each unique nasal deformity. Autogenous materials — primarily septal, auricular, and costal cartilage — remain the gold standard for augmentation and reconstruction.
Sources: Cummings Otolaryngology Head and Neck Surgery (Ch. 32); Bailey & Love's Short Practice of Surgery (28th ed., p. 785); Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.