Epididymitis Epididymiorchitis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile a thorough, well-structured answer.
Epididymitis and Epididymo-Orchitis
Definition and Anatomy
The epididymis is a tightly coiled tubular structure along the posterior aspect of the testis where sperm mature before transiting to the vas deferens. Epididymitis is inflammation of this structure. When the adjacent testis is also involved - which happens in the majority of bacterial cases - the combined condition is termed epididymo-orchitis. It is the most common intrascrotal inflammatory disease, predominantly affecting men aged 18-35 years, though it can occur at any age.
- Rosen's Emergency Medicine, p.1404
- Schwartz's Principles of Surgery, p.1789
Pathophysiology
Infection reaches the epididymis via retrograde spread from the vas deferens, originating from the urethra or bladder. The specific organisms depend on the patient's age, sexual activity, and comorbidities:
| Age / Risk Group | Predominant Organisms |
|---|---|
| Sexually active men <35 yrs | Chlamydia trachomatis, Neisseria gonorrhoeae |
| Insertive anal intercourse | C. trachomatis, N. gonorrhoeae, enteric Gram-negatives |
| Men >35 yrs / urinary pathology | E. coli, other enteric/urinary pathogens |
| Older men >60 yrs | Urinary pathogens; >50% have lower urinary tract obstruction |
| Children (prepubertal) | Often idiopathic; underlying congenital GU anomaly; neurogenic bladder |
| Rare causes | M. tuberculosis, Treponema pallidum, fungi, amiodarone toxicity, Behcet syndrome, Brucella |
- Rosen's Emergency Medicine, pp.1404-1405
Clinical Features
Symptoms
- Scrotal pain - characteristically gradual in onset (develops over 24-48 hours, unlike torsion which is abrupt within 4-8 hours)
- Pain may initially be referred to the lower abdomen or flank due to inflammation tracking along the vas deferens
- Fever (uncommon in isolated epididymitis, more common with orchitis/abscess)
- Dysuria, urethral discharge, or other urinary symptoms may be present (though only ~10% with STI-related epididymitis have visible urethral discharge)
- Nausea/vomiting from spermatic cord irritation
- Associated UTI symptoms (more common in older men)
Signs
-
Tender, swollen epididymis - initially localized to the epididymis, spreading to the testis over time
-
Testis in normal anatomic position (cf. high-riding testis in torsion)
-
Cremasteric reflex intact (absent in torsion)
-
Scrotal erythema and edema in more advanced cases
-
Reactive hydrocele may develop
-
Prehn's sign (pain relief on scrotal elevation) - historically described as positive in epididymitis, but has low sensitivity and specificity and should not be relied upon
-
A fluctuant scrotum suggests abscess formation
-
Rosen's Emergency Medicine, pp.1405-1406
-
Smith and Tanagho's General Urology, p.787
Differential Diagnosis
The most important differential is testicular torsion, which is a surgical emergency. Key distinguishing features:
| Feature | Epididymo-Orchitis | Testicular Torsion |
|---|---|---|
| Onset | Gradual (24-48 hrs) | Abrupt (exact time recalled) |
| Fever | Uncommon | Absent |
| Urinary symptoms | May be present | Absent |
| Nausea/vomiting | Less common | Sudden, severe |
| Cremasteric reflex | Intact | Absent |
| Testis position | Normal | High-riding, horizontal lie |
| Prehn's sign | Classically positive | Negative |
| Age peak | Any; puberty, >35 yrs | Neonates, adolescents |
Other differentials: torsion of appendix testis ("blue dot" sign), scrotal abscess, herniocoele, orchitis (viral - mumps), varicocele, testicular tumour (10% present with pain from haemorrhage).
- Smith and Tanagho's General Urology, pp.787-788
- Campbell-Walsh-Wein Urology, pp.2269-2270
Critical point: No single clinical feature reliably excludes torsion. Any equivocal presentation must be managed as torsion until proven otherwise - a missed torsion causes testicular loss.
Investigations
- Urinalysis and urine culture - pyuria present in 20-40% of cases; obtain before starting antibiotics
- Urethral swab or first-void urine NAAT (nucleic acid amplification test / PCR) for C. trachomatis and N. gonorrhoeae in sexually active men - highest sensitivity
- FBC - leucocytosis may be present but is nonspecific; does not differentiate from torsion
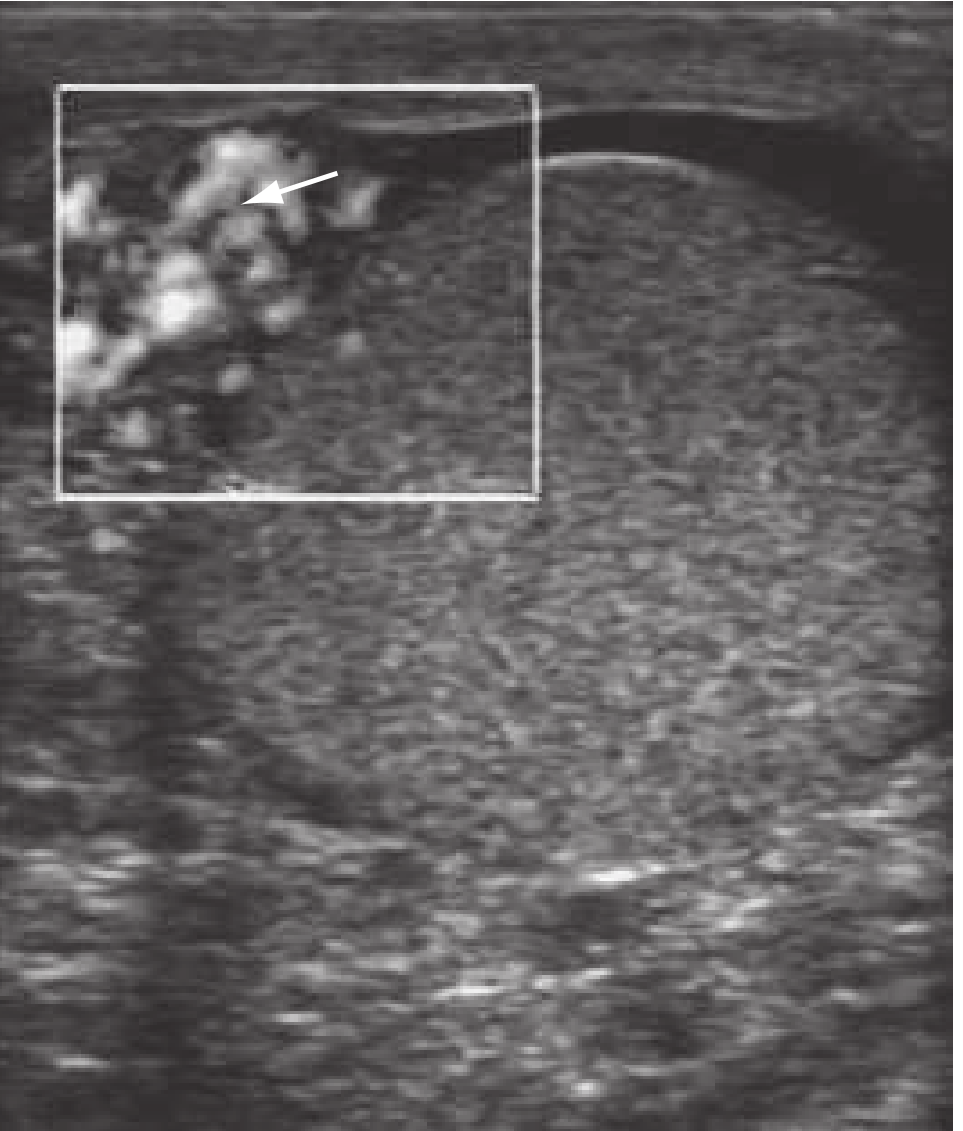
- Scrotal Doppler Ultrasound - primary imaging modality:
- Enlarged, hypoechoic epididymis with increased blood flow on Doppler (epididymitis)
- Reactive hydrocele may be seen
- If torsion is suspected: absence of testicular flow, spermatic cord twist sign
- Note: severe orchitis can reduce testicular flow, potentially mimicking torsion
- Renal US + cystography/VCUG in prepubertal boys with recurrent epididymitis - to detect underlying urinary tract anomalies (found in up to 47% of prepubertal boys in some series)
- Rosen's Emergency Medicine, pp.1405-1406
- Campbell-Walsh-Wein Urology, pp.2396-2398
Management
Antibiotic Therapy
Empirical therapy is guided by the most likely causative organism:
| Clinical Scenario | First-line Regimen |
|---|---|
| Presumed STI (sexually active man, any age) | Ceftriaxone 500 mg IM single dose + Doxycycline 100 mg PO BD x 10-14 days |
| Presumed enteric organism (older man, urinary pathology) | Levofloxacin 500 mg PO OD x 10 days OR Ofloxacin 300 mg PO BD x 10 days |
| STI + enteric risk (insertive anal intercourse) | Ceftriaxone 500 mg IM single dose + Levofloxacin 500 mg PO OD x 10 days |
| IV therapy (febrile, toxic, unable to tolerate PO) | Hospitalise; IV ceftriaxone ± fluoroquinolone; switch to oral when improving |
EAU guidelines recommend ceftriaxone 500 mg IM + doxycycline 200 mg as first dose for STI-presumed cases.
- Rosen's Emergency Medicine, pp.1406; Tintinalli's Emergency Medicine, p.[Table 93-2]
Adjunct / Supportive Care
- NSAIDs (e.g., ibuprofen) - reduce inflammation and pain
- Scrotal support (supportive underwear or elevation)
- Rest and ice packs
- Abstinence from sexual intercourse until both the patient and partner(s) have completed treatment (STI-related cases)
- Partner notification and treatment even if partner cultures are negative
Indications for Hospitalisation
- Fever / systemic toxicity
- Inability to take oral antibiotics
- Suspected abscess (requires surgical drainage or orchiectomy)
- Immunocompromised patients
Special Considerations
-
Testicular abscess: If abscess develops from untreated/progressive infection, surgical drainage or orchiectomy may be needed
-
Tuberculosis: Antituberculous therapy; if no resolution in 2 months, epididymectomy or orchiectomy; chronic involvement characterised by lower pole epididymal swelling, beading of the vas, possible "cold" abscess
-
Children: Broad-spectrum antibiotics with Gram-negative coverage if pyuria present; in absence of UTI, symptoms may resolve without antibiotics
-
Viral orchitis (Mumps): Supportive only; occurs in 20-30% of post-pubertal males with mumps; main complication is testicular atrophy potentially causing infertility if bilateral
-
Bailey and Love's Surgery, pp.1326-1336; Rosen's Emergency Medicine, p.1406
Complications
| Complication | Notes |
|---|---|
| Testicular abscess | Requires drainage or orchiectomy |
| Infertility | Bilateral involvement, tubular obstruction |
| Chronic epididymitis | Persistent/recurrent pain; quinolones or doxycycline x 4-6 weeks; epididymectomy if refractory (50% continue pain post-surgery) |
| Testicular atrophy | Especially in mumps orchitis |
| Sepsis | Rare but life-threatening; IV antibiotics, hospitalisation |
| Reactive hydrocele | Usually resolves with treatment |
- Bailey and Love's Surgery, p.1328; Rosen's Emergency Medicine, p.1404
Epididymo-Orchitis vs Isolated Epididymitis
In most bacterial infections, the testis is secondarily involved once epididymal infection is established, making epididymo-orchitis the more accurate term for the majority of cases. Isolated orchitis without epididymal involvement is rare in bacterial disease but common in viral infections (mumps, coxsackievirus, EBV, varicella). Immunocompromised patients may develop orchitis from mycobacteriosis, cryptococcosis, toxoplasmosis, or candidiasis.
- Tintinalli's Emergency Medicine, p.[Orchitis section]; Schwartz's Principles of Surgery, p.1789
Sources: Rosen's Emergency Medicine 9e | Campbell-Walsh-Wein Urology | Schwartz's Principles of Surgery 11e | Bailey and Love's Surgery 28e | Smith and Tanagho's General Urology 19e | Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.