Iron deficiency anemia according to Robbins pathology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Finding Sources
I now have comprehensive content from both Robbins editions and excellent diagrams. Let me compile the full, detailed answer.
Iron Deficiency Anemia - Robbins Pathology
Iron deficiency is the most common nutritional disorder in the world and the leading cause of anemia globally. About 10% of people in higher-resource countries and 25-50% in lower-resource countries are anemic, with iron deficiency being the most frequent cause.
Iron Metabolism (Background)
Understanding iron deficiency requires knowing normal iron balance.
Body iron distribution (healthy young adults):
| Pool | Males (mg) | Females (mg) |
|---|---|---|
| Total | 3,450-6,000 | 2,450-2,500 |
| Hemoglobin | 2,100 | 1,750 |
| Myoglobin | 300 | 250 |
| Enzymes | 50 | 50 |
| Ferritin/Hemosiderin (storage) | 1,000 | 400 |
- ~80% of body iron is "functional" - present in hemoglobin, myoglobin, and iron-containing enzymes (catalase, cytochromes)
- The remaining 15-20% is in the storage pool as ferritin and hemosiderin in macrophages of the liver, spleen, and bone marrow
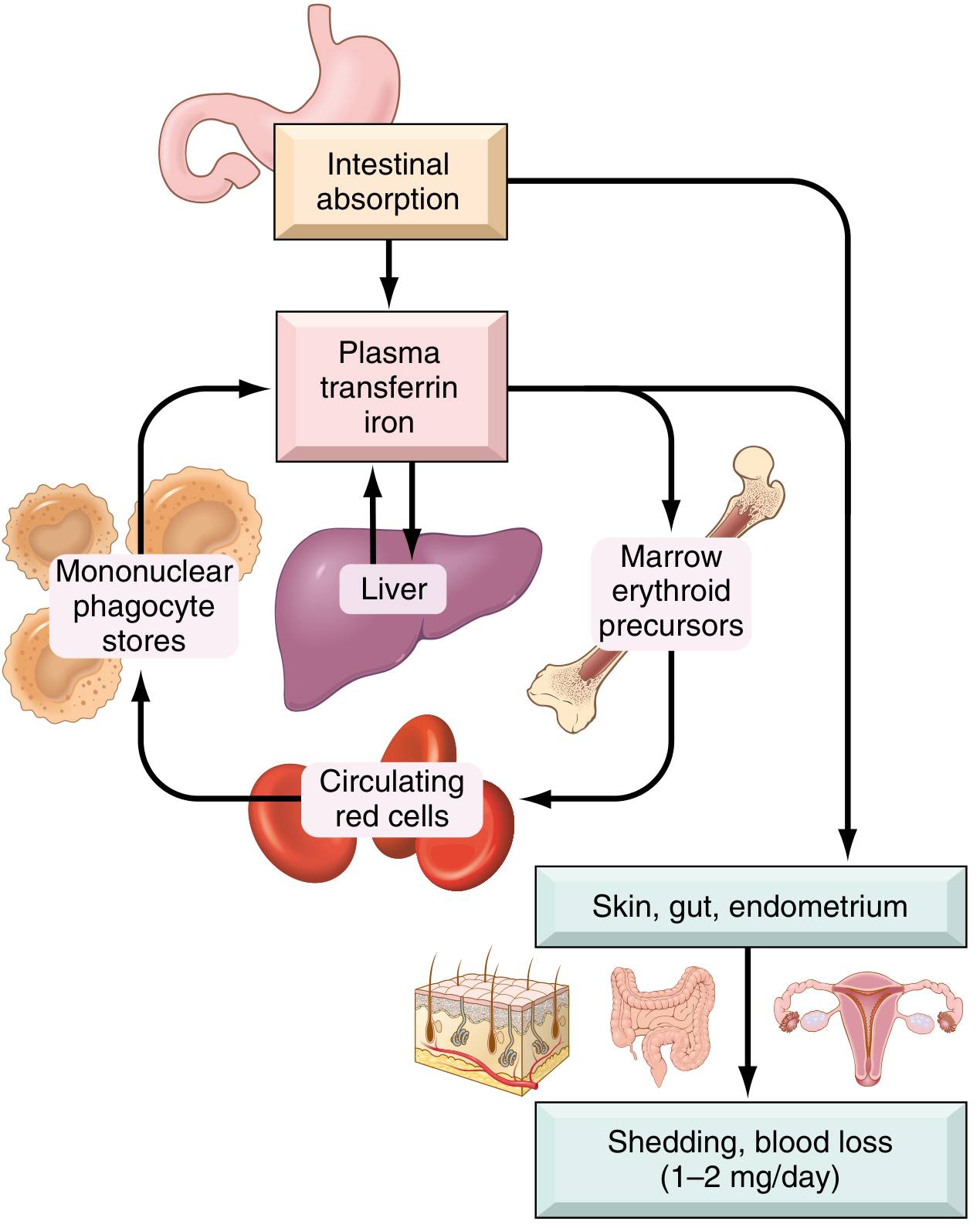
- Iron is lost at 1-2 mg/day through shedding of mucosal and skin epithelial cells
- The normal Western diet provides 10-20 mg/day; about 20% of heme iron and only 1-2% of nonheme iron is absorbable
Iron absorption - key molecular steps:
The diagram below (Fig. 14.21 from Robbins, Cotran & Kumar) illustrates the regulation of iron absorption:
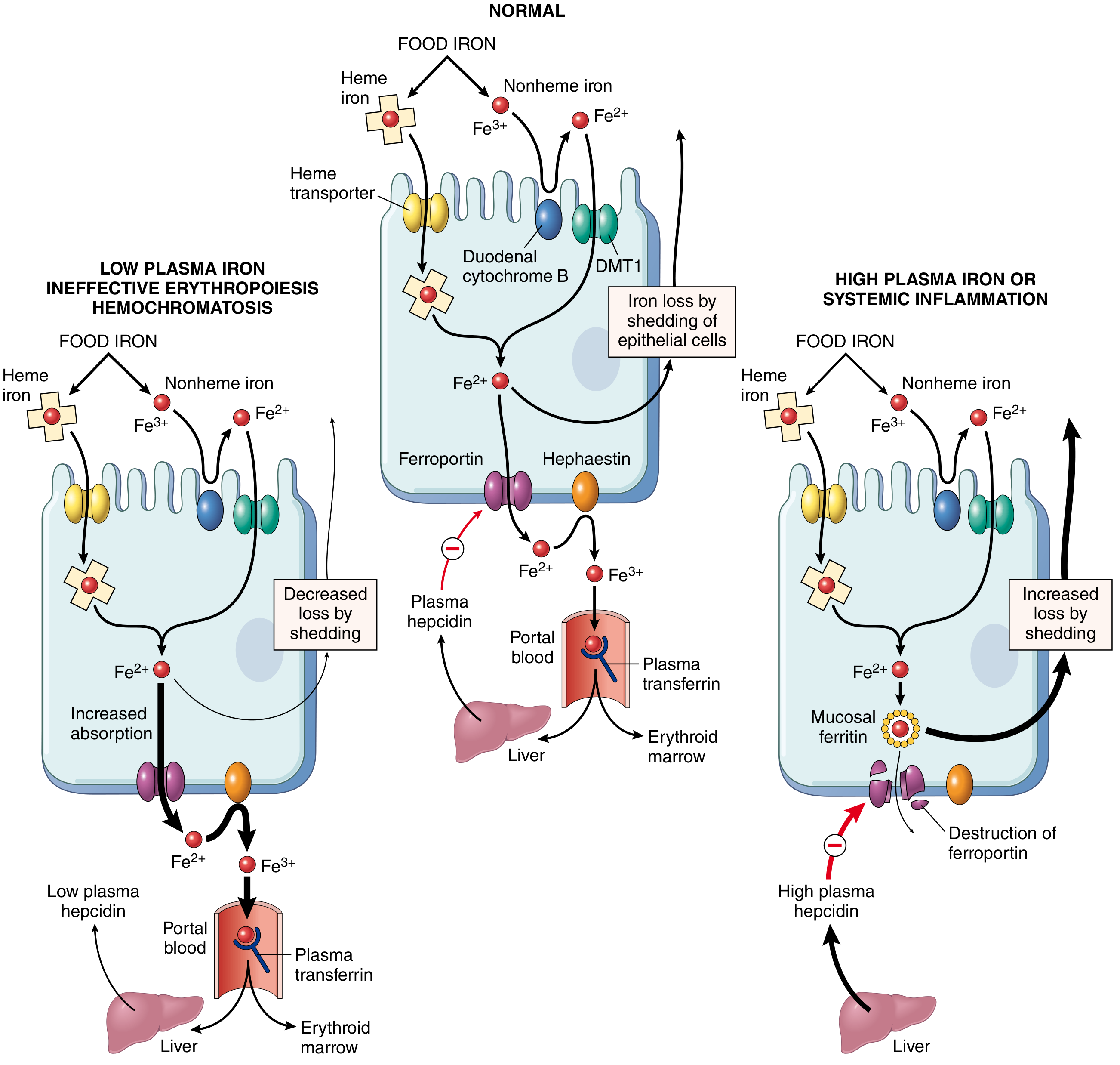
- Duodenal cytochrome B reduces Fe³⁺ → Fe²⁺
- DMT1 (divalent metal transporter-1) transports Fe²⁺ across the apical membrane of enterocytes
- Ferroportin moves iron from cytoplasm to plasma across the basolateral membrane
- Iron is oxidized back to Fe³⁺ by hephaestin and ceruloplasmin, then binds to plasma transferrin
- Transferrin delivers iron to erythroid precursors in the marrow
Hepcidin - the master regulator:
- A small peptide secreted by the liver in an iron-dependent fashion
- Negatively regulates ferroportin - binds and causes its degradation
- When body iron is high → hepcidin rises → ferroportin is destroyed → iron is trapped in enterocytes and macrophages → reduced absorption
- When iron is low → hepcidin falls → increased absorption and release from stores
- Also regulated by erythroferrone (from erythroblasts - suppresses hepcidin) and IL-6 (from inflammation - stimulates hepcidin)
Iron metabolism cycle (Fig. 14.20, Robbins):
Etiology / Causes
Iron deficiency arises from four major mechanisms:
1. Chronic Blood Loss (most important cause in developed countries)
- GI tract: peptic ulcers, colon cancer, hemorrhoids, hookworm infestation
- Genital tract: menorrhagia, metrorrhagia, endometrial cancer
- Key clinical pearl: Iron deficiency anemia in adult males or postmenopausal females in high-income countries must be attributed to gastrointestinal blood loss until proven otherwise - failure to investigate risks missing a GI cancer
2. Dietary Deficiency (most important cause in low-resource countries)
- Predominantly vegetarian diets have poor iron bioavailability
- At-risk groups in developed countries:
- Infants fed exclusively on milk (breast milk provides only ~0.3 mg/L)
- The impoverished with suboptimal diets
- Older adults (restricted diets, poor dentition)
- Vegans (no heme iron)
3. Increased Requirements (unmet by normal intake)
- Infants, children, and adolescents (rapid growth)
- Premenopausal females, especially during pregnancy
- Females in low-resource countries with multiple closely spaced pregnancies are at exceptionally high risk
4. Impaired Absorption
- Celiac disease (sprue)
- Other causes of steatorrhea
- Chronic diarrhea
- Gastrectomy (reduces acidity, increases transit speed through duodenum)
- Dietary inhibitors: tannins (tea), carbonates, oxalates, phosphates
- Dietary enhancers: ascorbic acid, citric acid, amino acids, sugars
Stages of Iron Deficiency
Iron deficiency develops insidiously in three progressive stages:
| Stage | Storage Iron | Serum Iron | Transferrin | Hemoglobin |
|---|---|---|---|---|
| Stage 1 - Depletion | ↓ (ferritin ↓, no marrow stainable iron) | Normal | Normal | Normal |
| Stage 2 - Iron-deficient erythropoiesis | Absent | ↓ | ↑ (TIBC ↑) | Borderline |
| Stage 3 - IDA | Absent | ↓↓ | ↑↑ (TIBC ↑↑) | ↓↓ (anemia) |
Morphology (ROBBINS MORPHOLOGY BOX)
Bone Marrow:
- Mild to moderate increase in erythroid progenitors
- Diagnostically significant: absence of stainable iron in macrophages on Prussian blue stain of aspirated marrow
Peripheral Blood Smear:
- Red cells are microcytic (small) and hypochromic (pale)
- Normal red cells have a central pallor zone measuring ~1/3 of cell diameter
- In iron deficiency, the central pallor zone is enlarged - hemoglobin seen only in a narrow peripheral rim
- "Pencil cells" (small, elongated red cells/poikilocytosis) are characteristically seen
Laboratory Findings
| Test | Finding in IDA |
|---|---|
| Hemoglobin/Hematocrit | Decreased (usually moderate) |
| MCV, MCH, MCHC | Low (microcytic, hypochromic indices) |
| Serum iron | Low |
| Serum ferritin | Low (< 12 μg/L) |
| TIBC (transferrin level) | High (elevated) |
| Transferrin saturation | < 15% |
| Serum hepcidin | Decreased |
| Platelet count | Often elevated (reactive thrombocytosis) |
| Reticulocytes | Low initially; rise after 5-7 days of iron therapy |
| Erythropoietin | Elevated but marrow response blunted by iron deficiency |
Clinical Features
Most cases are mild and asymptomatic. Symptoms, when present, are nonspecific:
- Weakness, listlessness, pallor
- Koilonychia (spoon nails) - thinning, flattening, and "spooning" of fingernails in long-standing anemia
- Pica - compulsion to consume non-food substances (dirt, clay, ice) - a curious but characteristic neurobehavioral complication
- Impaired work performance and cognitive function
- Reduced immunocompetence
- Dominant symptoms often relate to the underlying cause (GI disease, menorrhagia, malabsorption)
Key Clinical Pearl
"Persons often die with iron deficiency anemia but virtually never of it. An important point to remember is that in well-nourished persons, microcytic hypochromic anemia is not a disease but rather a symptom of another underlying disorder (e.g., colon cancer leading to chronic blood loss)."
- Robbins & Kumar Basic Pathology
IDA vs. Anemia of Chronic Inflammation (Differential)
Since both are microcytic/hypochromic, distinguishing them is clinically important:
| Feature | IDA | Anemia of Chronic Inflammation |
|---|---|---|
| Serum iron | ↓ | ↓ |
| TIBC (transferrin) | ↑ | ↓ |
| Serum ferritin | ↓ | ↑ |
| Marrow iron stores | Absent | Increased |
| Hepcidin | ↓ | ↑ (due to IL-6) |
Treatment
- Oral iron supplementation
- Reticulocyte count rises within 5-7 days, followed by gradual normalization of blood counts and red cell indices
- Treating the underlying cause is paramount
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), Chapter 14, pp. 612-614
- Robbins & Kumar Basic Pathology (Robbins Pathology), Chapter 10, pp. 393-394
This is a shared conversation. Sign in to Orris to start your own chat.