Mospel Poisoning Management
Reading File
Finding Sources
Finding Sources
Searching the Web
Mospel poisoning management organophosphate
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive information to provide a full answer. Let me compile everything.
Mospel (Organophosphate) Poisoning - Management
Mospel is a commercial organophosphate (OP) insecticide. Like all OPs, it works by irreversibly inhibiting acetylcholinesterase (AChE), causing accumulation of acetylcholine (ACh) at synapses and overstimulation of both muscarinic and nicotinic receptors.
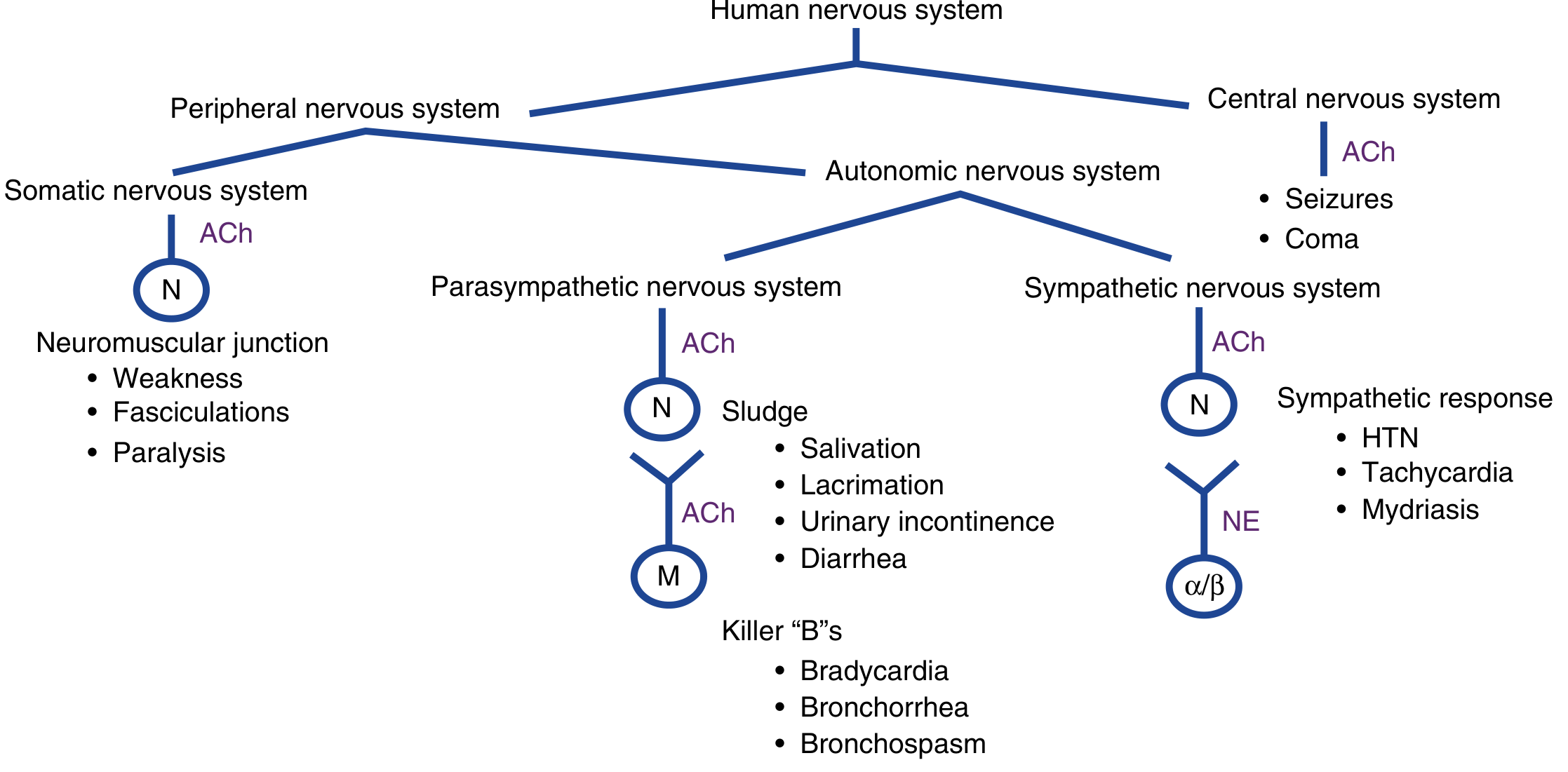
Mechanism of Toxicity
OP compounds phosphorylate and inhibit AChE at the synaptic junction. Accumulated ACh causes:
| Receptor Type | Location | Effects |
|---|---|---|
| Muscarinic | Parasympathetic end-organs | SLUDGE + Killer Bs |
| Nicotinic | Neuromuscular junction | Weakness, fasciculations, paralysis |
| Nicotinic | Sympathetic ganglia | HTN, tachycardia, mydriasis |
| CNS | Brain | Seizures, coma |
Clinical Presentation - The Cholinergic Toxidrome
SLUDGE / DUMBELS (muscarinic effects):
- Salivation
- Lacrimation
- Urination
- Diarrhea / Diaphoresis
- Gastrointestinal cramps
- Emesis
Killer Bs (the lethal muscarinic triad):
- Bradycardia
- Bronchorrhea
- Bronchospasm
Nicotinic effects: Muscle weakness, fasciculations, paralysis (including diaphragm - the proximate cause of death)
CNS effects: Anxiety, seizures, coma
Other: Miosis (pinpoint pupils), garlic/hydrocarbon odor, diaphoresis
The majority of severely poisoned patients will have altered mental status, pinpoint pupils, excessive sweating, and difficulty breathing.
Diagnosis
- Clinical - based on history + cholinergic toxidrome. Do not delay treatment while awaiting labs.
- Plasma butyrylcholinesterase - easier to assay, decreases first; may be reduced up to 50% in asymptomatic patients
- Red cell acetylcholinesterase - more accurate indicator; reduced to 10-20% of normal in moderate poisoning, <10% in severe
- ECG: QTc prolongation, ST changes, torsades de pointes, AV block
- CXR: Pulmonary edema in severe cases
- Bloods: Pancreatitis, hypo/hyperglycemia, leukocytosis, abnormal LFTs possible
Management - Four Goals
- Decontamination
- Supportive care with respiratory stabilization
- Reversal of acetylcholine excess (antidotes)
- Reversal of toxin binding at cholinesterase
Step 1: Scene Safety & Decontamination
- PPE for staff: Level C protection - full-face air purifier mask, eye shield, chemical-resistant suit, nitrile/butyl rubber gloves (NOT latex)
- Remove all clothing - place in plastic bags and treat as hazardous waste
- Wash skin thoroughly with copious water and mild detergent (soap/dishwashing liquid); include scalp, hair, fingernails, skin folds, conjunctivae
- Eye exposure: Flush with water for at least 15 minutes
- Inhalation: Remove to fresh air immediately
- Ingestion: Gastric lavage and activated charcoal have no proven benefit - vomiting/diarrhea already flush GI tract; rapid absorption negates benefit
- Contain and dispose of runoff water as hazardous material
Step 2: Airway & Supportive Care
- 100% oxygen via non-rebreather mask - optimize oxygenation before atropine to minimize dysrhythmia risk
- Intubation if: coma, seizures, respiratory failure, severe bronchospasm/bronchorrhea
- Preferred paralytic: Rocuronium 1 mg/kg (non-depolarizing, not metabolized by cholinesterases)
- Avoid succinylcholine if possible - metabolized by cholinesterases; in OP poisoning, duration may extend to 4-6 hours
- Suction airway secretions aggressively
- Cardiac monitoring + pulse oximetry + ECG
- IV access with baseline bloods including cholinesterase levels
- Avoid beta-blockers for tachycardia - treat the underlying cholinergic excess instead
Step 3: Antidote Therapy
A. Atropine (Muscarinic Antagonist) - FIRST-LINE
Atropine blocks ACh at muscarinic receptors only (does not reverse nicotinic/NMJ effects).
| Parameter | Details |
|---|---|
| Route | IV (IM if IV not yet available) |
| Initial adult dose | 1.2-3 mg IV (severity-dependent) |
| Initial pediatric dose | 0.05 mg/kg IV |
| Titration | Double the dose every 5 minutes until atropinization achieved |
| Total dose | No maximum - patients may require 200-500 mg in the first hour |
| Maintenance infusion | 10-20% of total cumulative dose per hour |
| Typical infusion range | 0.4-4 mg/hour IV in adults |
Endpoints of atropinization (target):
- Dry chest on auscultation (secretions cleared)
- Heart rate >80 bpm
- Systolic BP >80 mmHg
- Respiratory rate normalizing
Atropine does NOT: treat miosis, fasciculations, or muscle weakness (these are nicotinic effects).
Tachycardia and mydriasis during atropine therapy are NOT indications to stop - continue until secretions are dry.
Atropine toxicity (over-atropinization): absent bowel sounds, hyperthermia, delirium - reduce dose if present.
Note: Atropine requirements can exhaust hospital supplies. Alternative anticholinergics if atropine unavailable: IV glycopyrrolate (does not cross BBB - no CNS effect) or nebulized ipratropium bromide for pulmonary muscarinic effects.
B. Pralidoxime / 2-PAM (Oxime - Cholinesterase Reactivator) - SECOND-LINE
Pralidoxime reactivates phosphorylated AChE before "aging" (irreversible conformational change occurs). It addresses both muscarinic AND nicotinic effects, including NMJ paralysis.
| Parameter | Details |
|---|---|
| Timing | Give as soon as possible; may still be effective 24-48 hours after exposure |
| Adult loading dose | 30 mg/kg IV (or 1-2 g bolus) mixed in normal saline, infused over 5-10 min |
| Pediatric loading dose | 30 mg/kg IV (up to 1 g) |
| Maintenance infusion | 8 mg/kg/hour for 24-48 hours |
Pralidoxime is most effective when given early. Once "aging" of the OP-AChE bond occurs (varies by compound), it is no longer effective. Aging for most agricultural OP compounds occurs over hours to days; nerve agents like soman age within minutes.
C. Benzodiazepines (for Seizures)
- Diazepam 5-10 mg IV (repeat as needed) - first-line for seizures
- Other benzodiazepines (lorazepam, midazolam) are also appropriate
- Benzodiazepines should be given after airway is secured
Step 4: Manage Complications
| Complication | Management |
|---|---|
| Pulmonary edema/bronchospasm | O2, intubation, PEEP, atropine, pralidoxime |
| Seizures | Benzodiazepines IV |
| Torsades de pointes | Standard protocol (MgSO4) |
| Ventricular tachycardia/fibrillation | Metoprolol 5 mg IV boluses every 5 min |
| Hyperthermia (from prolonged seizures) | Benzodiazepines + external evaporative cooling |
| Rhabdomyolysis | IV crystalloid hydration + urine alkalinization |
| Metabolic acidosis / AKI | IV fluids, supportive |
Avoid: Succinylcholine, ester anesthetics, beta-blockers (may potentiate poisoning)
Step 5: Enhanced Elimination
- No role for hemodialysis or other extracorporeal elimination techniques.
Intermediate Syndrome
A delayed complication occurring 24-96 hours after acute poisoning (after the cholinergic crisis resolves):
- Proximal limb weakness, neck flexor weakness
- Respiratory muscle paralysis (can cause respiratory failure)
- Cranial nerve palsies
- Managed with respiratory support; usually resolves within 7 days
Delayed Neuropathy (Organophosphate-Induced Delayed Neuropathy - OPIDN)
- Appears weeks after exposure
- Symmetrical sensorimotor axonopathy - leg cramps, weakness, can mimic Guillain-Barré syndrome
- Cognitive dysfunction, autonomic dysfunction, peripheral neuropathy, extrapyramidal signs
- No specific antidote; supportive management
Disposition
- All symptomatic patients require hospital admission for monitoring and treatment
- Severe cases require ICU-level care
- Asymptomatic patients with confirmed significant exposure should be observed for at least 6-8 hours
Summary Algorithm
MOSPEL (OP) POISONING
│
├── SCENE SAFETY → PPE for all staff
├── DECONTAMINATION → Remove clothes, wash skin with soap & water
│
├── AIRWAY → O2, intubate if needed (use rocuronium, not succinylcholine)
├── MONITORING → Cardiac monitor, SpO2, ECG, IV access
│
├── ANTIDOTES:
│ ├── ATROPINE → 1.2-3 mg IV, double q5min → atropinize → then infusion 10-20%/hr
│ ├── PRALIDOXIME → 30 mg/kg IV over 5-10 min → 8 mg/kg/hr x 24-48h
│ └── BENZODIAZEPINES → Diazepam 5-10 mg IV for seizures
│
└── COMPLICATIONS → Treat seizures, arrhythmias, rhabdomyolysis, hyperthermia
Sources:
- Rosen's Emergency Medicine: Concepts and Clinical Practice, Chapter 152
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, Chapter 201
- Morgan & Mikhail's Clinical Anesthesiology, 7e
- Lippincott Illustrated Reviews: Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.