Femoral shaft fractures
Reading File
Finding Sources
Searching PubMed
"femoral shaft fracture" AND management
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material for a detailed answer. Let me compile everything.
Femoral Shaft Fractures
Source: Rockwood and Green's Fractures in Adults, 10th ed. (2025), Chapter 57
Epidemiology & Significance
Femur fractures represent 1-9% of all fractures and are a major source of morbidity and mortality. Associated injuries - chest, abdominal, and pelvic trauma; hemorrhage; fat embolism; pulmonary dysfunction; and organ failure - significantly increase morbidity and mortality. With modern surgical techniques, improved implant design, and better management of associated injuries, outcomes continue to improve.
Applied Anatomy
The femur is a tubular long bone with posterior cortical thickening (linea aspera), serving as attachment for fascia and muscles. It has an anterolateral bow with an average radius of curvature of 120 cm - critical for nail selection and insertion.
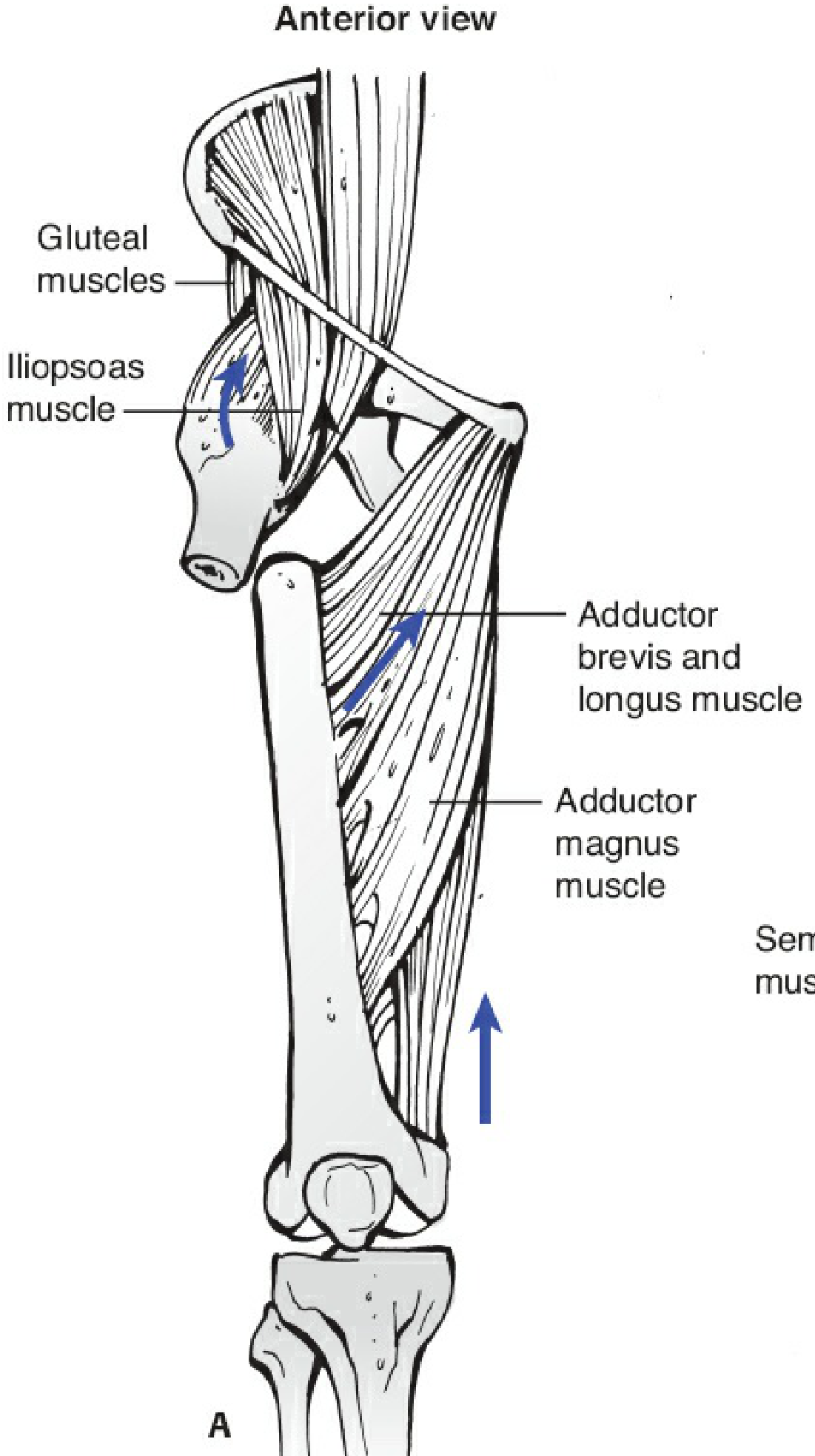
Muscle attachments and deforming forces (Fig. 57-6):
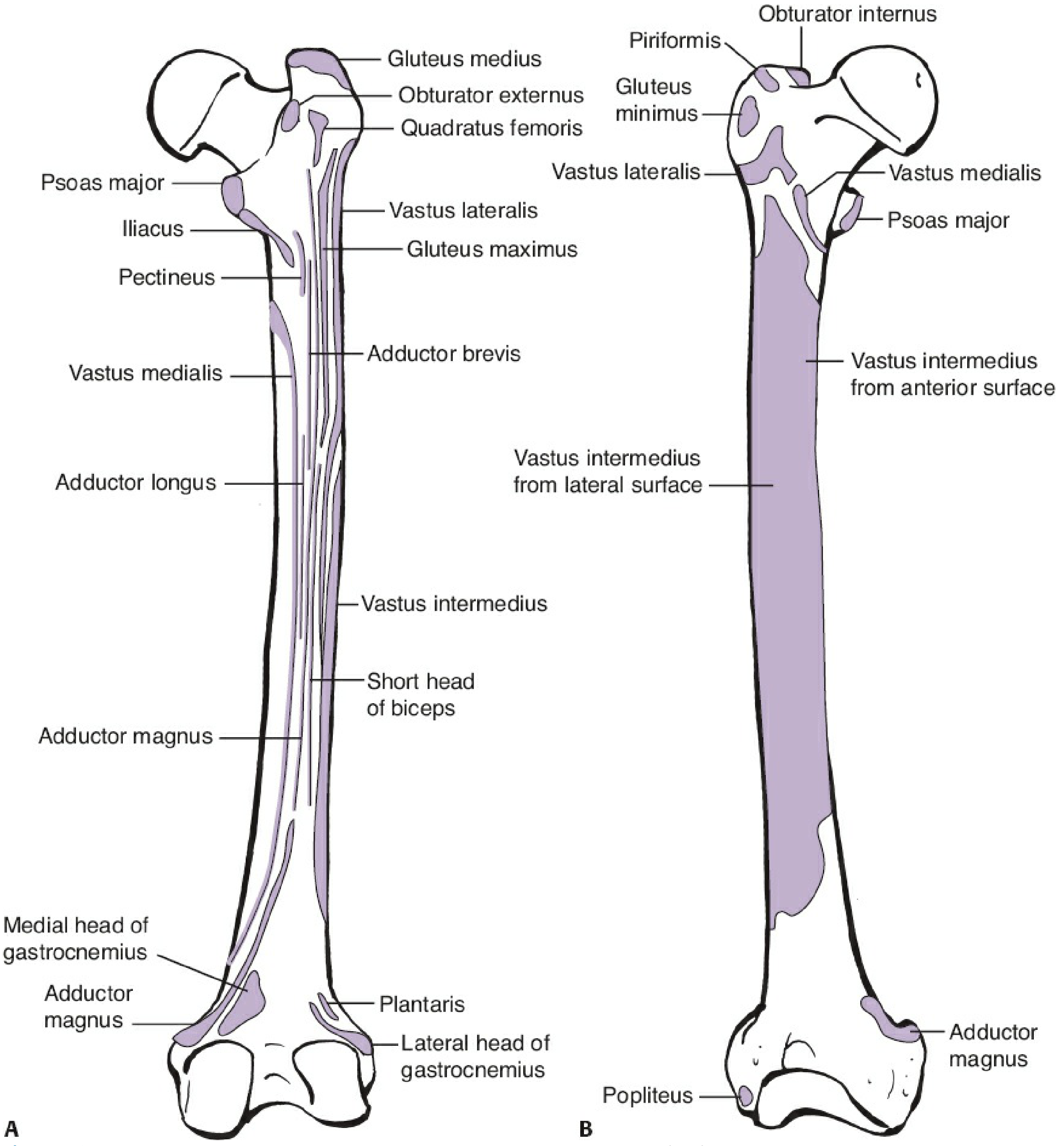
When the femur fractures, predictable deformities occur at each level:
| Fracture Level | Proximal Fragment Deformity | Distal Fragment Deformity |
|---|---|---|
| Proximal third | Flexion + ER (iliopsoas), abduction (gluteals) | Pulled medially + proximally (adductors/hamstrings) |
| Middle third | Mild flexion + abduction | Shortening, slight flexion |
| Distal third/metadiaphyseal | Medialization of shaft (adductors) | Extension deformity (gastrocnemius pulling condyles posteriorly) |
Three thigh compartments:
- Anterior: quadriceps, sartorius, iliopsoas, pectineus - femoral artery/vein, femoral nerve, lateral femoral cutaneous nerve
- Medial: adductor group, gracilis, obturator externus - profunda femoris artery, obturator nerve/vessels
- Posterior: biceps femoris, semitendinosus, semimembranosus, part of adductor magnus - sciatic nerve, profunda femoris branches
Mechanism of Injury
- High-energy trauma (most common): MVAs, falls from height, ballistic injuries - typical in younger patients
- Low-energy trauma / fragility fractures: in elderly with osteoporosis; pathologic fractures (metastatic disease)
- Atypical femoral shaft fractures: associated with long-term bisphosphonate use (transverse or short oblique, lateral cortex beaking)
- Stress fractures: repetitive loading (military recruits, distance runners)
Associated Injuries
Always screen for:
- Ipsilateral femoral neck fracture (in 2-9% of femoral shaft fractures - easily missed, higher risk with comminuted fractures)
- Acetabular fractures
- Knee ligament injuries / posterior cruciate ligament tears
- Tibial plateau fractures
- Vascular injuries (popliteal artery with distal fractures)
- Thoracoabdominal trauma in high-energy mechanisms
Classification
OTA/AO Classification (most widely used):
- 32-A: Simple (transverse, oblique, spiral)
- 32-B: Wedge (intact bending wedge, fragmented wedge, spiral wedge)
- 32-C: Complex/comminuted (spiral, segmental, irregular)
Winquist-Hansen Classification (for comminution degree):
- Grade 0: No comminution
- Grade I: Minor comminution, <25% contact
- Grade II: 50% or more cortical contact on each main fragment
- Grade III: <50% cortical contact between main fragments
- Grade IV: No cortical contact (segmental, "floating" bone)
Open fracture grading (Gustilo-Anderson): Grades I-IIIC guide antibiotic prophylaxis, wound management, and timing of definitive fixation.
Initial Assessment & Imaging
Clinical signs: pain, swelling, deformity, shortening, external rotation, inability to bear weight. Examine the hip and knee carefully. Check neurovascular status (posterior tibial and dorsalis pedis pulses, sciatic/peroneal nerve function).
Hemorrhage: The femoral shaft can accommodate 1-2 L of blood loss into the thigh - hemodynamic assessment is mandatory. Closed femoral shaft fractures can cause significant blood loss and hypovolemic shock.
Imaging workup:
- AP and lateral of the entire femur (including hip and knee)
- AP pelvis
- CT scan of the hip/femoral neck if neck fracture suspected
- CT angiography if vascular injury suspected
Treatment
Nonoperative Treatment
Largely historical - traction (skeletal or skin) was the mainstay before IMN. Now reserved for:
- Children under ~6 years (Pavlik harness, spica casting)
- Patients too medically unstable to undergo any surgery (temporary measure)
- Patients with severe contamination precluding surgery
Disadvantages: prolonged bed rest, significant rates of malunion, knee stiffness, DVT risk.
Operative Treatment - Overview
Intramedullary nailing (IMN) is the standard of care for femoral shaft fractures in adults. It provides load-sharing fixation, allows early mobilization, and has excellent union rates.
Antegrade Intramedullary Nailing
Gold standard for most femoral shaft fractures.
Starting point options:
- Piriformis fossa entry: Direct axis of the femoral canal; ideal for straight nails; risk of iatrogenic femoral neck fracture if misdirected
- Greater trochanter (trochanteric) entry: More lateral; requires a laterally offset proximal nail design; technically easier access, especially in obese patients; more widely used today
Positioning:
- Supine on fracture table (most common): Traction pin or boot traction; image intensifier positioned on contralateral side; contralateral hip/leg positioned for lateral imaging
- Lateral decubitus: Easier access to starting point; soft tissue of hip falls away; but limits use of contralateral leg for rotation/length comparison - careful positioning required to avoid inadvertent adduction and internal rotation
Key operative steps: provisional traction to restore length → proper starting point → sequential reaming (over-ream by 1-2 mm) → nail insertion → static interlocking proximally and distally → confirm reduction on AP and lateral
Static vs. dynamic locking: Most femoral shaft fractures are locked statically in both the proximal and distal holes. Dynamization (removal of one interlocking screw) may be used for delayed unions.
Retrograde Intramedullary Nailing
Starting point: Apex of Blumensaat line in the intercondylar notch on the lateral view; consistent with the normal valgus of the distal femoral articular surface.
Indications for retrograde over antegrade:
- Ipsilateral femoral neck fracture (combined retrograde nail + femoral neck fixation)
- Obesity / difficult trochanteric access
- Pregnancy (avoids radiation to the fetus in the supine-on-fracture-table position)
- Bilateral femoral shaft fractures
- Polytrauma (facilitates bilateral simultaneous nailing)
- Fractures extending into the distal metaphysis
- Pre-existing hip arthroplasty above the fracture
Concerns: Risk of knee sepsis, articular cartilage injury, PCL injury with poor starting point, heterotopic ossification around the knee. Retrospective reviews show no increase in knee septic complications.
Plate Fixation
Indications (generally secondary to IMN failure or IMN not feasible):
- Small medullary canal
- Fractures around a pre-existing malunion / nonunion with canal obliteration
- Periprosthetic fractures around stable hip or knee replacements
- Femoral shaft fractures with extension proximally or distally making IMN difficult
- Ipsilateral femoral neck + shaft fractures (combined plate fixation possible)
- Associated vascular injury requiring medial exposure (fracture exposed and plated prior to vascular repair)
- Treatment of nonunions (adjunctive plate around existing IMN)
External Fixation
Used as damage control in:
- Hemodynamically unstable polytrauma patients ("damage control orthopaedics")
- Severely contaminated open fractures
- Burns with wound involvement
Planned conversion to definitive IMN typically performed within 7-14 days, before pin-track colonization develops.
Surgical Pitfalls and Prevention
| Pitfall | Prevention |
|---|---|
| Failure to obtain correct length | Adequate muscular paralysis; contralateral radiographs; ensure guidewire seated in distal femur before measuring |
| Coronal/sagittal malreduction | Center guidewire and reamers on both views; correct starting point |
| Iatrogenic fracture during nail insertion | Pre-op assessment of deformity; over-ream by 1-2 mm; clear intramedullary cortical fragments |
| Femoral malrotation | AP imaging of contralateral femur at known rotation; compare lesser trochanteric profiles; post-op CT if uncertain |
| Missed femoral neck fracture | Preoperative CT of hip in all high-energy femoral shaft fractures; post-nailing imaging of the femoral neck is mandatory |
Postoperative Care
- Weight-bearing as tolerated immediately after locked nailing in isolated fractures
- Physical therapy targeting hip abductors, external rotators, hip and knee flexors/extensors, balance, and gait
- Radiographs at 6 and 12 weeks (callus expected by 6 weeks); continue at 6-8 week intervals until union
- Significant groin pain at follow-up = suspect missed femoral neck fracture regardless of prior imaging
Complications
| Complication | Notes |
|---|---|
| Malrotation | Most common malalignment complication; rotational malunion up to 15-20° tolerated, beyond that symptomatic |
| Angular malalignment | <5° acceptable in all planes |
| Delayed union / nonunion | Rate ~1-2% with modern nailing; risk factors include open fractures, infection, smoking, diabetes, Winquist Grade III/IV, inadequate fixation |
| Infection | 1-2% for closed fractures; significantly higher for open; can lead to osteomyelitis |
| Compartment syndrome | Uncommon in isolated femoral shaft fractures (thigh has large volume); may occur with high-energy or combined injuries |
| Knee stiffness / pain | Common after retrograde nailing and with associated knee injuries |
| Fat embolism syndrome | Risk especially in polytrauma; early fixation (<24 hours) decreases risk |
| Femoral nail failure | Nail breakage usually occurs at unhealed fracture sites; interlocking screw breakage more common |
| Heterotopic ossification | More common around the knee after retrograde nailing |
| Nerve injury | Sciatic nerve most commonly with posterior approaches; usually neurapraxia |
Special Situations
Ipsilateral femoral neck + shaft fracture:
- Occurs in ~5% of femoral shaft fractures
- Femoral neck fracture is often undisplaced and easily missed
- Reconstruction nail (with proximal femoral neck screws) or separate fixation constructs
- Femoral neck fracture takes priority
Open femoral shaft fractures:
- I-IIIB: IMN after thorough debridement (reamed or unreamed); external fixation as bridge in severely contaminated or hemodynamically unstable patients
- IIIC: Vascular repair with temporary vascular shunting; fracture stabilization (external fixator or plate) then definitive nailing once contamination controlled
Periprosthetic fractures (around hip/knee replacement):
- Vancouver classification for hip; Su classification for knee
- Usually require plate fixation; nail possible if the stem allows passage
Pediatric femoral shaft fractures (briefly):
- Under 6 months: Pavlik harness
- 6 months-6 years: spica casting
- 6-11 years: flexible intramedullary nails (TENS)
- Over 11 years / >50 kg: rigid IMN (taking care to protect the greater trochanteric apophysis to avoid AVN)
Recent Evidence (2025)
- A 2025 systematic review (PMID 40127141) on diaphyseal femoral nonunions identified key risk factors including smoking, open fractures, high-grade comminution, infection, and inadequate fixation - confirming known clinical predictors.
- A 2025 network meta-analysis (PMID 41029075) on analgesic strategies before spinal anesthesia in femoral shaft fractures found fascia iliaca compartment blocks among the most effective approaches for preoperative pain control.
- Rockwood and Green's Fractures in Adults, 10th Ed. (2025), Chapter 57 - Femoral Shaft Fractures (Adams JD Jr., Jeray KJ)
Bone healing and it’s stages absolute and relative stability and perrins and wolffs law , factors affecting bone healing
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed. Here is the comprehensive answer:
Bone Healing - Stages, Stability Concepts, Perren's & Wolff's Laws, and Factors Affecting Healing
Sources: Campbell's Operative Orthopaedics 15th Ed. (2026), Rockwood and Green's Fractures in Adults 10th Ed. (2025), Bailey and Love's Short Practice of Surgery 28th Ed., Miller's Review of Orthopaedics 9th Ed.
1. Overview: Two Modes of Bone Healing
Bone can heal in two fundamentally different ways, determined by the mechanical environment at the fracture site:
| Feature | Primary (Direct) Healing | Secondary (Indirect) Healing |
|---|---|---|
| Callus formed? | No | Yes |
| Mechanical environment | Absolute stability | Relative stability |
| Requires | Anatomic reduction + compression | Alignment restoration only |
| Mechanism | Osteoclastic cutting cones | Endochondral ossification |
| Analogy | Sutured wound | Scab → normal tissue |
| Clinical examples | Lag screw + plate, compression plating | IMN, bridge plate, cast, external fixator |
"Direct bone healing heals directly with bone and without callus formation. It happens in an environment of cortical apposition and absolute stability with no movement or gap between the fracture fragments." - Bailey and Love's, 28th Ed.
2. Stages of Bone Healing (Secondary / Indirect - Most Common)
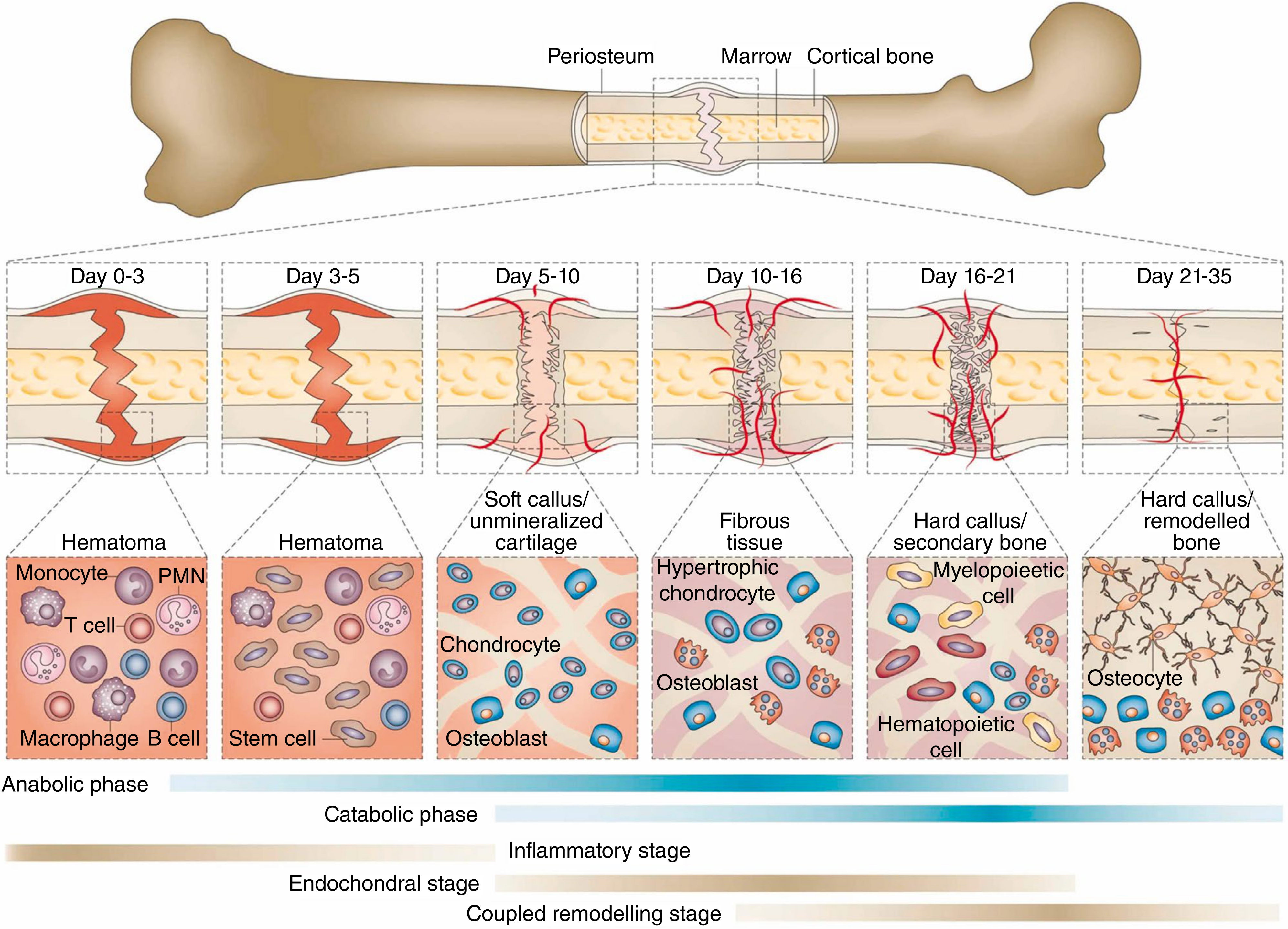
Bone regeneration after fracture is a continuous, overlapping process described in four stages (Einhorn):
Stage 1 - Hematoma Formation (Day 0-3)
- Rupture of blood vessels at the fracture site fills the gap with hematoma
- Hematopoietic cells (monocytes, PMNs, T cells, macrophages, B cells) flood the site
- The hematoma forms the initial scaffold for healing
- Inflammatory cells initiate lysosomal degradation of necrotic tissue
- Fracture surfaces undergo resorption, which initially widens the gap - this is protective as it lowers interfragmentary strain
Stage 2 - Fibrovascular / Granulation Tissue Formation (Day 3-10)
- Reparative phase begins Day 4-5 post-injury
- Pluripotential mesenchymal stem cells invade the hematoma and differentiate into fibroblasts, chondroblasts, and osteoblasts
- Angiogenesis within periosteal tissues and marrow delivers cells to the fracture site
- Soft (cartilaginous) callus forms - the fracture becomes "sticky" but not rigid
- Granulation tissue replaces the hematoma
Stage 3 - Bony Callus Formation (Day 10-35)
- Hard callus phase: the cartilaginous callus undergoes endochondral ossification, replaced with woven bone
- Peripheral callus (periosteal) forms first, followed by medullary callus (slower)
- Calcified, immature woven bone remains at the end of this stage
- Amount of callus formed is inversely proportional to the extent of immobilization - more motion = larger callus
- Clinical union occurs when stiffness and strength from mineralization make the fracture site stable and pain-free
- Radiographic union = bone trabeculae or cortical bone crossing the fracture line on plain X-ray
Stage 4 - Remodeling (Months to Years)
- Begins in the middle of the repair phase; continues for months to years (radioisotope studies show activity long after clinical/radiographic union)
- Woven bone is replaced by lamellar bone (stronger, organized along lines of stress)
- Medullary canal is restored
- Bone gradually assumes its normal morphology and mechanical strength according to the loads placed upon it (Wolff's Law)
- Remodeling can continue up to 7 years after the fracture
3. Perren's Interfragmentary Strain Theory
Strain is defined as: ΔL / L (change in fracture gap divided by original gap length)
This is the foundational concept linking mechanical environment to tissue differentiation.
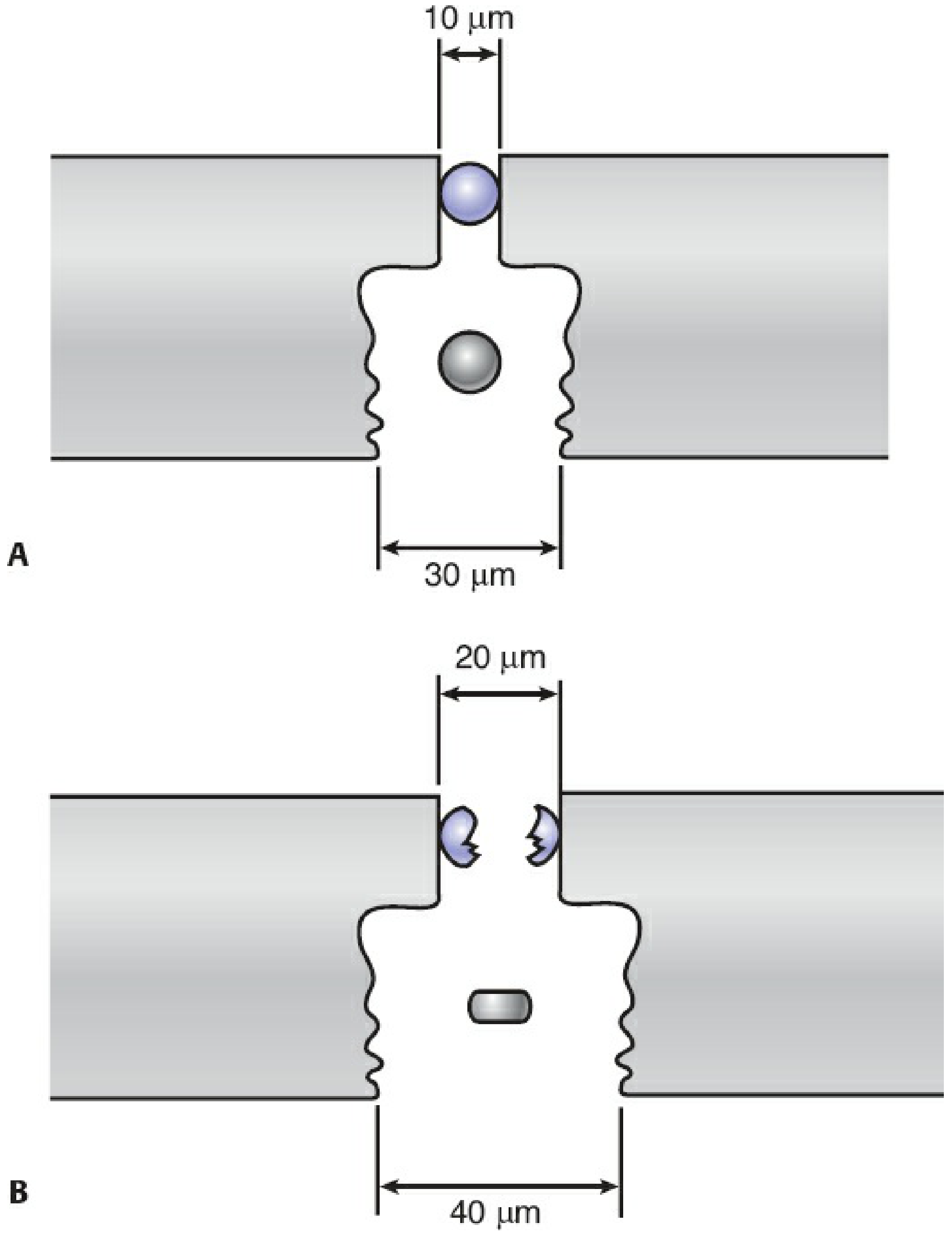
Key concept from the diagram (Fig. 12-23, Rockwood & Green):
- Panel A (10 μm gap): A single cell within a narrow gap ruptures upon even minimal distraction - HIGH strain
- Panel B (20 μm gap): The same amount of distraction across a wider gap with multiple cell layers merely deforms/stretches the cells - LOW strain
This explains why comminuted fractures (large surface area = wide effective gap) tolerate more motion than simple fractures (small surface area = narrow gap = high strain from same motion).
Strain Thresholds and Tissue Formed
| Interfragmentary Strain | Tissue Formed | Clinical Implication |
|---|---|---|
| < 2% | Bone (primary healing / direct ossification) | Absolute stability needed |
| 2% - 10% | Cartilage → endochondral ossification (secondary bone healing) | Relative stability: callus forms |
| 10% - 100% | Fibrous tissue | Too much motion - fibrous nonunion risk |
| > 100% | No tissue forms; cell rupture | Gross instability - healing cannot proceed |
"A little movement is good, too much movement is bad" - Bailey and Love's
Dynamic strain reduction: As granulation tissue and then callus form at the fracture site, they mechanically increase the cross-sectional area, reducing strain progressively. This is why a simple fracture CAN heal under relative stability - the process is self-reinforcing. The early inflammatory resorption of fracture surfaces also widens the effective gap, reducing strain, which promotes the progression from fibrous tissue → cartilage → bone.
Zero strain is NOT optimal: Some load and resulting strain are necessary within a healing fracture to stimulate bone formation. Studies show that femurs fixed with lower stiffness rods produced more stabilizing callus than those with rigid fixation.
4. Absolute Stability vs. Relative Stability
Absolute Stability
- Definition: No motion at the fracture site under physiologic loads
- Strain: Near zero (< 2%)
- Healing: Primary bone healing - no callus formed, osteoclastic cutting cones tunnel across the fracture, followed by osteoblasts laying lamellar bone
- Requirements: Anatomic reduction + interfragmentary compression
- Implant examples: Lag screws ± neutralization plate, dynamic compression plating
- Indications: Articular fractures (require anatomic reduction), simple diaphyseal fractures amenable to compression
- Drawbacks: Longer healing time; harder to confirm by radiology (no visible callus); implants must have longer fatigue life; biologically demanding (removes fracture hematoma)
Relative Stability
- Definition: Controlled micromotion at the fracture site under physiologic loads
- Strain: 2-10% range
- Healing: Secondary bone healing - callus formation via endochondral ossification
- Requirements: Length, alignment, and rotation restored; anatomic reduction of individual fragments NOT needed
- Implant examples: Intramedullary nails, bridge plates, casts, external fixators, flexible elastic nails
- Indications: Diaphyseal fractures, comminuted fractures, most metaphyseal fractures
- Mechanism: Micromotion stimulates callus; callus then increases stability; strain progressively decreases; healing self-reinforces
- Pitfall: Too much motion → hypertrophic nonunion (callus spreads to reduce force but never mineralizes) or fibrous nonunion
"Diaphyseal fractures need treatment with relative stability and indirect reduction techniques to maximize the local healing process. In contrast, articular fractures usually require a direct reduction for perfect anatomy and subsequent fixation with absolute stability." - Mulholland and Greenfield's Surgery 7th Ed.
5. Wolff's Law and Related Laws
Wolff's Law (Julius Wolff, 1892)
Bone deposition and resorption depend on the stresses applied to it.
Bone adapts its structure in response to mechanical loading:
- Areas under increased load → bone is deposited (thicker trabeculae, denser cortex)
- Areas under reduced load → bone is resorbed (stress shielding under a rigid plate causes cortical thinning)
- Trabeculae align along principal stress trajectories
- Clinically relevant in: rehabilitation (weightbearing stimulates healing), implant design (stress shielding), stress fractures (repetitive loading exceeds remodeling capacity), and periprosthetic bone loss
Piezoelectric effect: When bone is mechanically loaded, the organic collagen matrix generates electrical charges (electronegative on compression side, electropositive on tension side) that further stimulate osteoblastic activity. This is the proposed mechanism for electromagnetic bone stimulation devices.
Hueter-Volkmann Principle (related - governs growth plates)
| Principle | Law |
|---|---|
| Hueter-Volkmann | Compressive forces inhibit physeal growth; tensile forces stimulate growth |
| Wolff's Law | Bone deposition and resorption depend on stresses applied |
Both principles govern bone remodeling and are relevant to understanding deformity correction in children - improving the biomechanical environment can reverse abnormal growth patterns.
6. Factors Affecting Bone Healing
(Miller's Review of Orthopaedics 9th Ed. / Campbell's 15th Ed. 2026)
A. Biologic (Patient-Related) Factors
| Factor | Effect |
|---|---|
| Age | Children heal faster; elderly have reduced osteogenic potential and vascularity |
| Nutritional status | Protein, calcium, Vitamin D, Vitamin C deficiency all impair healing |
| Hormones | Growth hormone, PTH, thyroid hormone promote healing; corticosteroids inhibit it |
| Vascular status | Poor blood supply (PVD, compartment syndrome, stripping of periosteum) severely impairs healing |
| Nerve function | Denervated limbs heal poorly - neurotrophic factors contribute to bone healing |
| Comorbidities | Diabetes (impairs microvascular flow and immune function), renal failure, liver disease, malignancy, immunodeficiency |
| Infection | Impairs all phases; especially problematic in open fractures; increases nonunion risk ~8x with 3+ comorbidities |
| Smoking | Most notable inhibitor - clinical and animal studies consistently show smoking, previous smoking, and smokeless tobacco significantly delay fracture and wound healing and increase nonunion risk |
| Medications | NSAIDs (conflicting data), corticosteroids, fluoroquinolones (implicated in slowing healing), chemotherapeutics; bisphosphonates - current evidence shows no significant impairment of fracture healing at therapeutic doses |
| Obesity | Increased complication rates |
| Osteoporosis | Reduced bone stock; impaired osteoblastic response |
| Growth factors | BMPs (especially BMP-2 for open tibial fractures, BMP-7 for tibial nonunions), TGF-β, IGF, PDGF, FGF |
B. Local (Injury-Related) Factors
| Factor | Effect |
|---|---|
| Fracture type | Transverse/simple > spiral/comminuted for healing speed; comminuted tolerate more motion |
| Soft tissue injury | Periosteal and soft tissue stripping reduces blood supply - major determinant of healing |
| Bone loss / gap | Large gaps cannot heal without bone grafting |
| Energy of injury | High-energy injuries damage vascularity and biology more severely |
| Number of bones | Ipsilateral or multiple fractures compete for repair resources |
| Pathologic conditions | Infection, tumor, Paget disease, radiation, avascular bone |
| Anatomic location | Cancellous (metaphyseal) bone heals faster (larger surface area, richer blood supply) than cortical (diaphyseal) bone; distal tibia and scaphoid are notoriously slow healers due to poor vascularity |
| Soft tissue interposition | Muscle or periosteum interposed between fracture fragments prevents healing |
C. Treatment-Related (Mechanical) Factors
| Factor | Effect |
|---|---|
| Type and rigidity of fixation | Must match fracture type: absolute stability for articular, relative stability for diaphyseal |
| Overdistraction | Excessive traction or distraction across fracture prevents bony bridging |
| Fracture displacement after reduction | Poor reduction, malalignment → increased complications and nonunion |
| Weight bearing / muscular stimulation | Lack of loading reduces mechanical stimulus for bone formation (Wolff's law) |
| Surgical trauma | Extensive soft tissue stripping reduces biologic potential; MIPO and biological fixation techniques reduce this |
| Bridge plating of simple fractures | Rigid bridge plating of unreduced simple fractures without callus formation = high nonunion risk |
7. Types of New Bone Formation in Fracture Repair
Four mechanisms operate simultaneously (Campbell's 15th Ed.):
- Osteochondral ossification - endochondral (cartilage → bone); main route in secondary healing
- Intramembranous ossification - direct bone formation without cartilage intermediate; occurs at periosteum
- Appositional new bone formation - periosteal surface deposition
- Osteonal migration (creeping substitution) - cutting cones traverse necrotic bone, seen in primary healing and cortical repair
8. Terminology
| Term | Definition |
|---|---|
| Clinical union | Fracture site stable and pain-free under physiologic loads |
| Radiographic union | Callus or bone trabeculae bridging the fracture line on X-ray |
| Delayed union | No progression of healing over serial radiographs; not yet defined as failure |
| Nonunion | Failure to progress to union; requires intervention. Types: hypertrophic (adequate biology, inadequate stability), oligotrophic, atrophic (inadequate biology) |
| Malunion | Fracture healed in an unacceptable position |
Sources: Campbell's Operative Orthopaedics 15th Ed. (2026), Ch. 58 | Rockwood and Green's Fractures in Adults 10th Ed. (2025), Ch. 12 | Bailey and Love's Short Practice of Surgery 28th Ed. | Miller's Review of Orthopaedics 9th Ed., Ch. 1
This is a shared conversation. Sign in to Orris to start your own chat.