Mr urography radiology ans
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
MR urography technique indications radiology sequences static excretory
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive information to provide a thorough answer on MR Urography. Let me compile it all.
MR Urography (MRU) - Radiology
Definition
MR Urography (MRU) is a non-invasive MRI-based technique that evaluates the entire urinary tract - kidneys, renal collecting systems, ureters, and bladder - in a single examination. It is capable of providing both morphological (anatomical) and functional information without using ionising radiation or iodinated contrast media.
Two Main Techniques
1. Static-Fluid (Anatomical) MRU
- Uses heavily T2-weighted sequences (e.g., HASTE/SSFSE - Half-Fourier Acquisition Single-Shot Turbo Spin-Echo)
- Fluid-filled structures (urine, CSF, bile) appear bright white due to long T2 relaxation time
- Does NOT require contrast injection
- Best for: demonstrating hydronephrosis, hydroureter, duplex systems, congenital anomalies
- Works well even in non-dilated or poorly functioning systems
- A thick-slab (60 mm) coronal oblique sequence gives the "urogram" overview
2. Excretory (Functional) MRU
- Uses T1-weighted gradient-echo sequences after IV gadolinium contrast injection
- Mimics conventional intravenous urography/pyelography
- Dynamic contrast-enhanced (DCE) sequences capture: arterial phase → corticomedullary phase → excretory phase
- Provides differential renal function (DRF), renal output efficiency, time-to-peak enhancement
- Strongly correlates with radionuclide scintigraphy (correlation coefficient ~0.95)
Combined static + functional MRU is used in complex cases (e.g., severe hydronephrosis or poorly functioning kidneys where excretory imaging alone may fail).
Typical MRU Protocol Sequences
| Sequence | Purpose |
|---|---|
| T2 HASTE/SSFSE axial (thin slice, 3mm) | Renal parenchyma, masses |
| T2 TRUFI/FIESTA fat-sat axial | Fluid-tissue contrast |
| T2 HASTE coronal (thin, 3mm) | Ureter delineation |
| T2 HASTE coronal thick slab (60mm) | Overview "urogram" image |
| T1 FLASH 3D coronal pre-contrast | Renal cortex, hemorrhage, fat |
| T1 FLASH 3D coronal arterial phase | Renal vasculature |
| T1 FLASH 3D coronal nephrographic + excretory phases | Collecting system with Gd |
| DWI (diffusion-weighted) | Pyelonephritis, tumour, obstruction |
For full functional MRU: patient requires hydration, often a diuretic (furosemide), and a urinary catheter; sedation may be needed in children.
Indications
Primary Indications
- Hydronephrosis - primary indication; assessment of obstructive uropathy
- Pregnancy with suspected ureteric calculus - avoids radiation; CT contraindicated
- Children - avoids radiation burden in the developing patient
- Iodinated contrast contraindicated - previous anaphylaxis, severe renal impairment (though gadolinium also carries NSF risk in GFR <30)
- Upper tract urothelial carcinoma (UTUC) - when CT urography (CTU) is contraindicated
- Haematuria workup - alternative when CTU not possible
- Congenital urogenital anomalies - ectopic ureters, duplex kidneys, cloacal malformations (pre-operative anatomy)
- Post-trauma - integrity of urinary tract
- Genitourinary TB - tract assessment
- Renal masses - cyst characterisation, VHL syndrome follow-up
- Neuropathic bladder - when spinal imaging also required
- Frequent UTIs - structural assessment
In Children Specifically (Table 72.6, Grainger & Allison)
- Abdominal/pelvic mass diagnosis and follow-up
- Acute pyelonephritis complications (if USS inconclusive)
- Spinal imaging + neuropathic bladder assessment
- Complex urogenital/cloacal malformations
- Post-trauma urine leak evaluation
Advantages of MRU
| Advantage | Detail |
|---|---|
| No ionising radiation | Ideal for children, pregnant patients, repeated follow-up |
| No iodinated contrast | Safe in iodine allergy, avoids CT contrast nephropathy |
| Combined anatomy + function | Single study replaces IVU + renogram |
| Excellent soft tissue contrast | Detects urothelial tumours, renal masses, perinephric pathology |
| DWI capability | Adds sensitivity for pyelonephritis, tumour cellularity, treatment response |
| Multiplanar reconstruction | 3D volumes allow coronal, sagittal views |
Limitations of MRU
| Limitation | Detail |
|---|---|
| Poor sensitivity for calculi | Cannot reliably detect urinary tract stones (the major limitation) - CT is far superior |
| Calculus vs. filling defect | Cannot distinguish stone from blood clot or tumour intraluminally |
| Availability | Not universally available; longer scan time than CT |
| Physiological hydronephrosis in pregnancy | Complicates interpretation - up to 80% of pregnant women have this (right > left) |
| Gadolinium risk in renal failure | Nephrogenic systemic fibrosis (NSF) risk in severe CKD (GFR <30) |
| Motion artifact | Requires breath-holding; sedation often needed in young children |
| Cost and time | More expensive and longer than CT |
MRU vs Other Modalities
| Feature | MRU | CTU | IVU | Ultrasound |
|---|---|---|---|---|
| Radiation | None | High | Moderate | None |
| Stone detection | Poor | Excellent | Good | Moderate |
| Soft tissue detail | Excellent | Good | Poor | Limited |
| Functional info | Yes (DRF) | No | Limited | Limited (Doppler RI) |
| Pregnancy safe | Yes | No | No | Yes |
| Stone differentiation | Poor | Excellent | Good | Poor |
Role in Specific Conditions
Acute Flank Pain / Suspected Ureteric Colic
MRU is limited here due to poor stone detection sensitivity. It is reserved for:
- Pregnant patients after inconclusive USS
- Combined USS + KUB is first approach in pregnancy, with MRU if needed
- Unenhanced CT remains gold standard for stone protocol
Upper Tract Urothelial Carcinoma (UTUC)
- CTU is optimal (sensitivity 67-100%, specificity 93-99%)
- MRU is the alternative when CTU is contraindicated
- Both RCR and ACR guidelines prefer CTU as first-line for haematuria workup
Obstructive Uropathy
- MRU shows hydronephrosis and functional drainage impairment
- Sensitivity 0.75 after intravenous contrast (Campbell-Walsh)
- Functional MRU can replace scintigraphy (MAG3 renogram) in many paediatric centres
Textbook Images
Fig. 72.15 (Grainger & Allison) - 3D T2 MRU showing grossly dilated right collecting system:
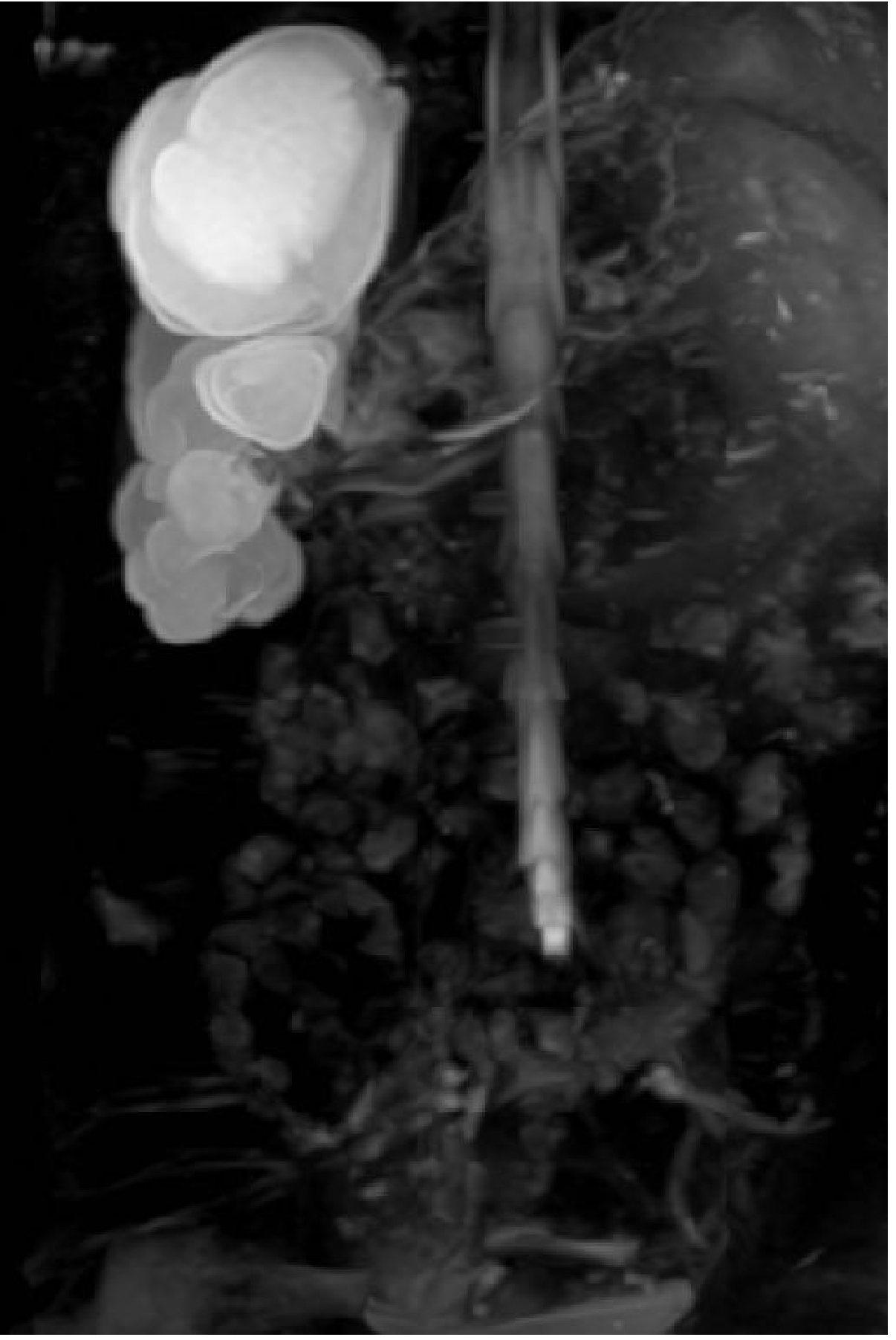
3D T2-weighted MR urography demonstrating grossly dilated right renal collecting system (hydronephrosis). Note the CSF is also visible in the background (also fluid-bright on T2).
Fig. 26.15 (Grainger & Allison) - MRI in a pregnant patient with left ureteric calculus:
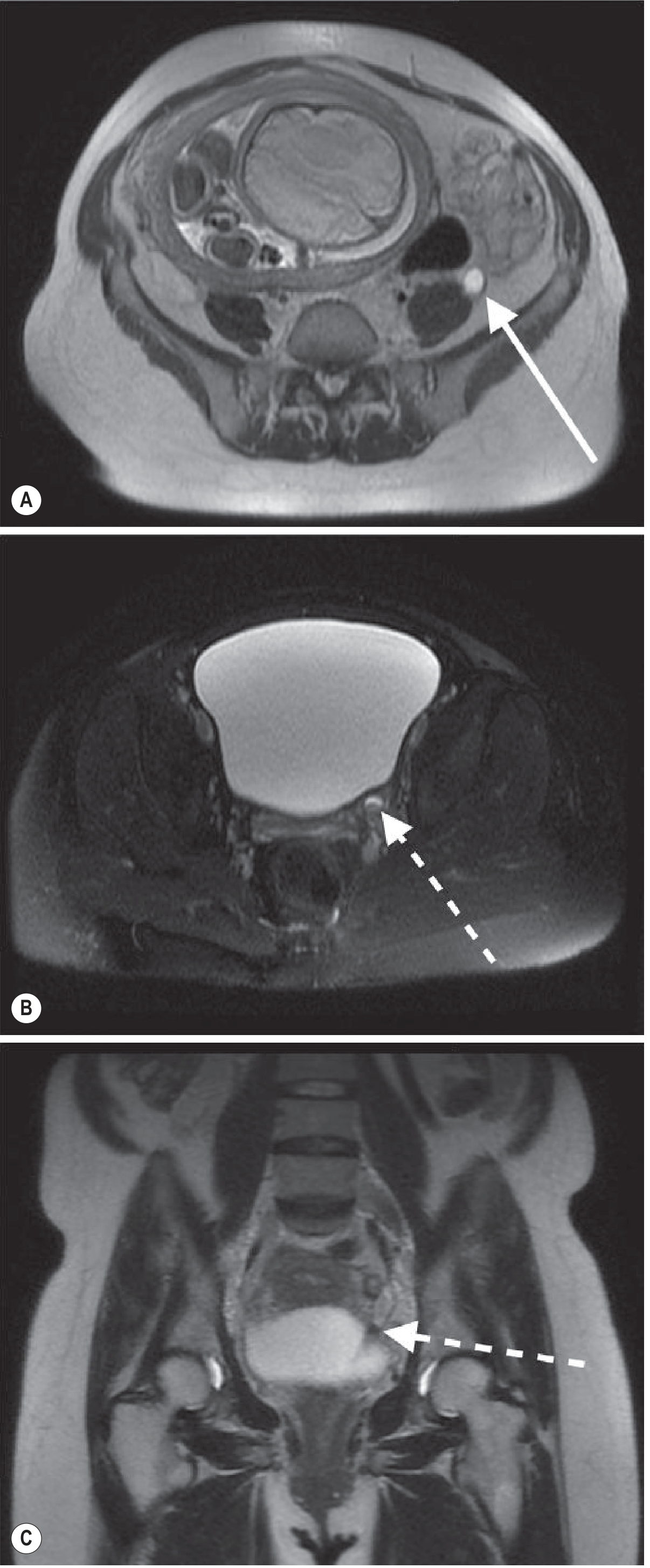
MRI in a pregnant patient with left flank pain and haematuria. (A) Axial T2: left hydroureter (solid arrow). (B,C) Filling defect in distal left ureter consistent with obstructing calculus (dashed arrows). This case illustrates MRU's role in pregnancy when CT is avoided.
Summary Points (Exam-Focused)
- MRU uses two strategies: static T2-fluid imaging (no contrast) + excretory T1-Gadolinium imaging
- Primary indication: hydronephrosis / obstructive uropathy evaluation
- Radiation-free - safe in pregnancy and children; preferred when CTU contraindicated
- Cannot reliably detect stones - CT urography remains superior for calculi
- Full functional MRU requires hydration, diuretic, catheterisation, dynamic T1 sequences
- Functional MRU correlates with MAG3 renogram; DRF correlates coefficient ~0.95
- DWI adds value for pyelonephritis, masses, obstruction assessment
- In UTUC: CTU is first-line; MRU is alternative when CTU not feasible
Sources: Grainger & Allison's Diagnostic Radiology, pp. 728-729; Campbell-Walsh-Wein Urology, Radiologic Imaging chapter; MRIMaster urography protocols
10 mark ans for sonological evalution if extratesticular scrotal lesions rguhs radiology ans
Reading File
Finding Sources
Finding Sources
Searching the Web
sonological evaluation extratesticular scrotal lesions ultrasound RGUHS radiology 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive textbook content for a complete 10-mark RGUHS-style answer. Let me compile it.
Sonological Evaluation of Extratesticular Scrotal Lesions
Introduction
Ultrasound (US) is the primary and gold-standard imaging modality for evaluation of scrotal pathology. High-frequency linear array transducers (9-15 MHz) provide excellent anatomical resolution of the testis and all extratesticular structures. A key role of scrotal US is to determine whether a mass is intratesticular or extratesticular, as this distinction has major clinical significance:
- Intratesticular mass: Generally considered malignant until proven otherwise
- Extratesticular mass: Only 3-6% are malignant in adults; majority are benign
Extratesticular lesions arise from the epididymis, tunica vaginalis, spermatic cord, scrotal wall, or other paratesticular structures, and are broadly classified as cystic or solid.
Technique
- Transducer: High-frequency linear array (9-15 MHz)
- Patient position: Supine, scrotum supported on a towel between the thighs
- Grey-scale US: Both longitudinal and transverse planes; bilateral comparison ("sunglasses view" or "buddy shot")
- Colour/Power Doppler: Essential for vascularity assessment, differentiating torsion from inflammation, and characterising solid masses
- Valsalva maneuver: Performed during Doppler for varicocele assessment
A. CYSTIC EXTRATESTICULAR LESIONS
Cystic lesions are far more common than solid ones in the extratesticular space.
1. Hydrocele
The most common cause of scrotal swelling.
Sonological features:
- Anechoic (non-reflective) fluid collection surrounding the anterior and lateral aspects of the testis
- May contain swirling low-level echoes from cholesterol crystals
- Congenital hydrocele: Patent processus vaginalis in neonates; usually resolves spontaneously
- Acquired hydrocele: Secondary to infection, trauma, tumour, or idiopathic
- Multiloculated hydrocele: May resemble organising haematoma; septations seen
- US indicated when hydrocele prevents clinical palpation of the testis (to exclude underlying malignancy)
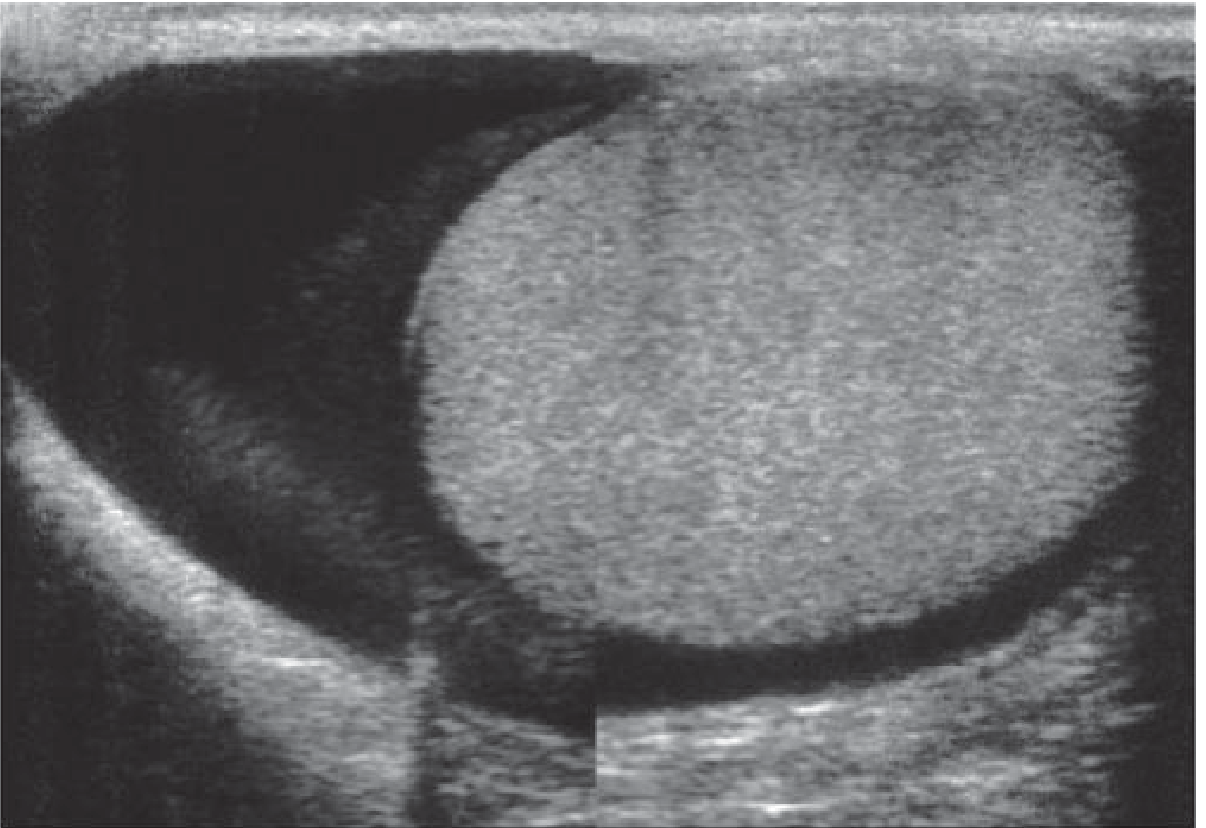
Fig. 33.13 - Longitudinal view of normal testis with a moderate hydrocele surrounding the anterior and lateral testicular surface.
2. Epididymal Cyst / Spermatocele
- Both result from dilated epididymal tubules
- Spermatocele: Retention cyst of the head of epididymis; contains sperm; usually found in the caput
- Epididymal cyst: May occur anywhere in the epididymis; does NOT contain sperm
Sonological features:
- Well-defined, discrete, anechoic (non-reflective) fluid-containing structure
- Single or multiple; posterior acoustic enhancement
- Located adjacent to the testis in the epididymis
- Large cysts may superficially resemble a hydrocele
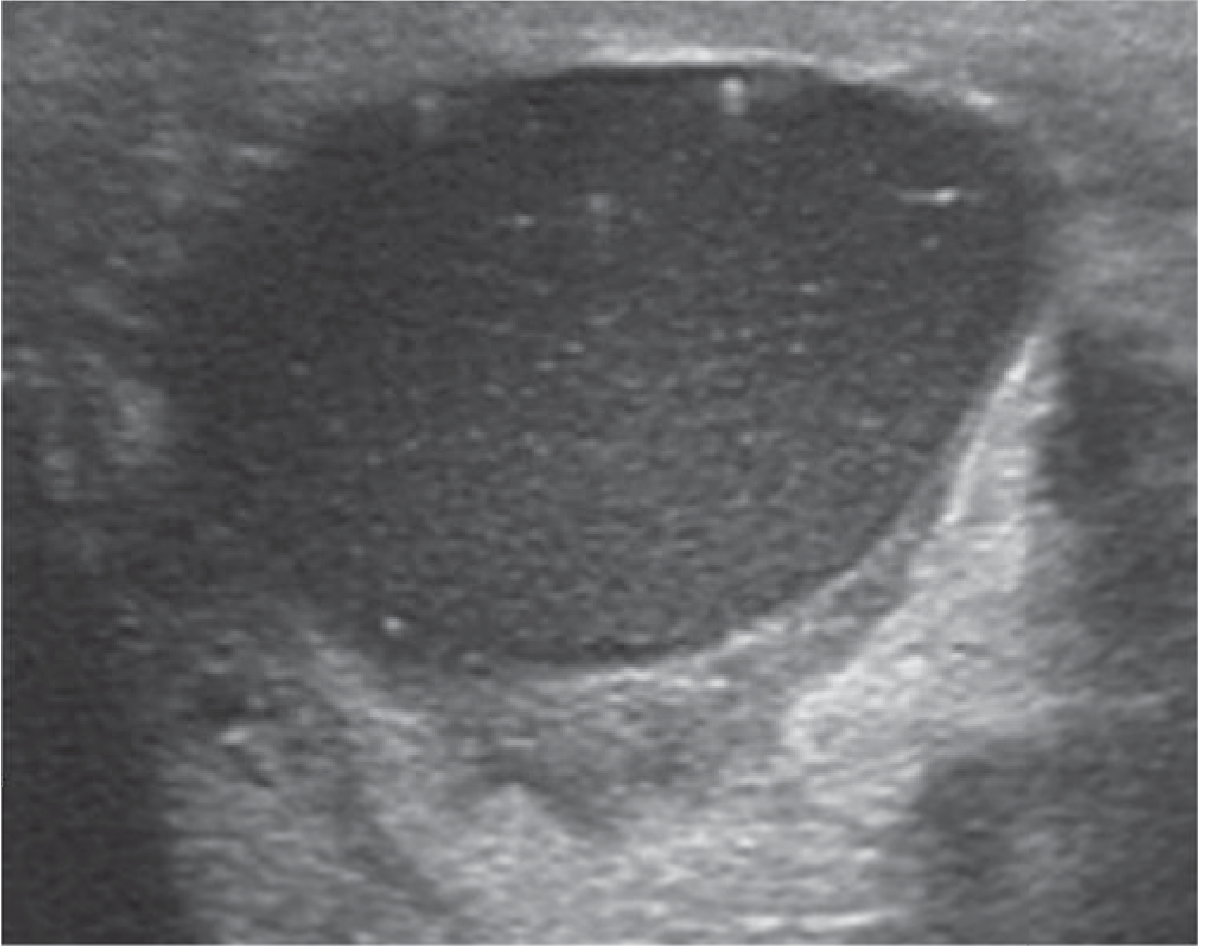
Fig. 33.15 - Well-defined anechoic epididymal cyst/spermatocele in the head of epididymis.
3. Pyocele
A urological emergency - purulent fluid collection within the scrotal sac.
- Rare complication of epididymo-orchitis
- Results from communication between an infected hydrocele and the tunica vaginalis lining
Sonological features:
- Complex, often heavily loculated fluid collection
- Multiple low-level internal echoes due to pus
- Thick irregular walls
- Associated epididymal/testicular abscess
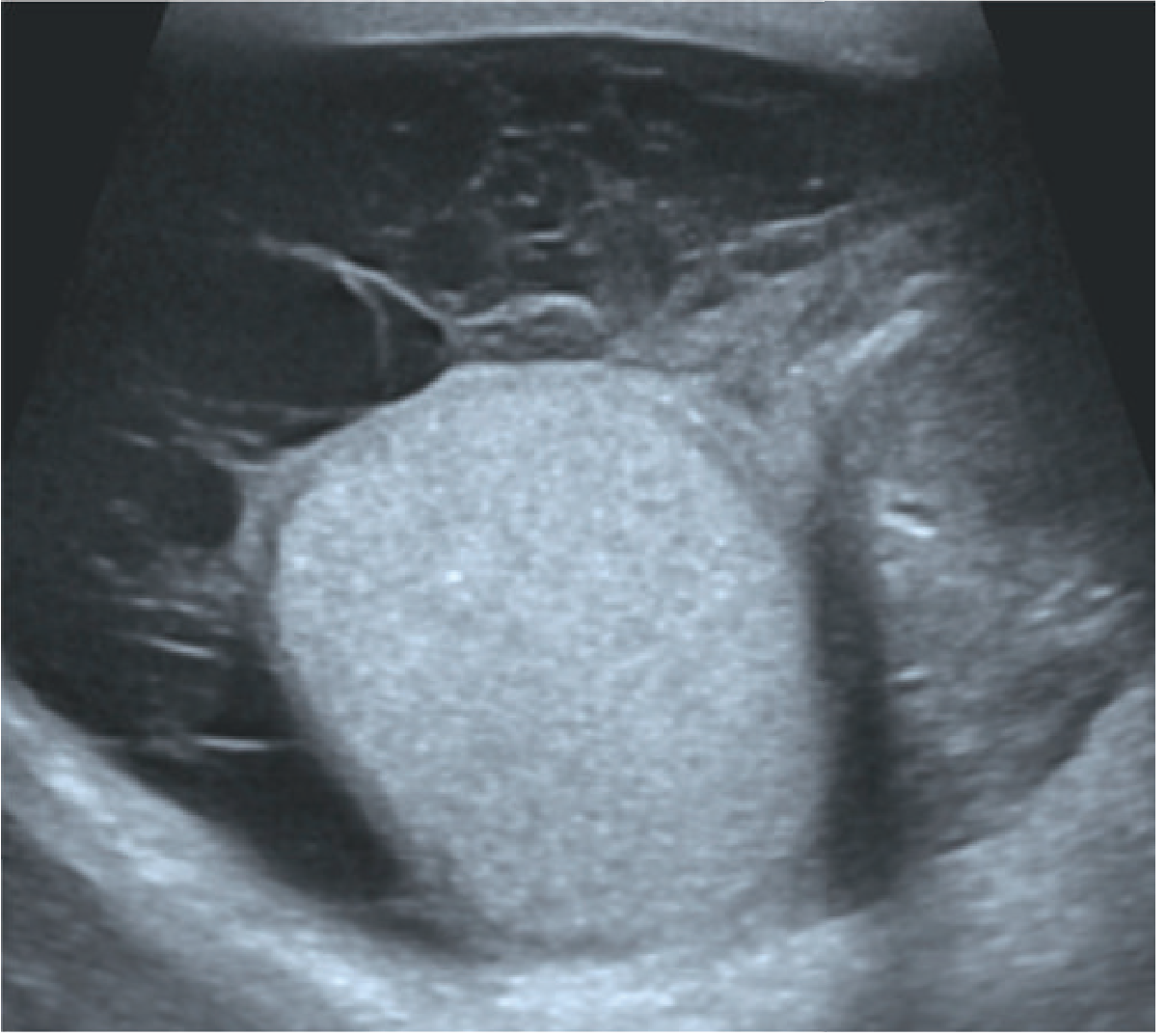
Fig. 33.19 - Pyocele: complex loculated fluid collection with internal echoes following acute epididymitis.
4. Haematocele / Organising Haematoma
- Blood within the tunica vaginalis, usually post-traumatic
Sonological features:
- Septated, complex collection with variable echogenicity
- Hyperechoic acutely, becoming more complex over time
- May be indistinguishable from a multiloculated hydrocele
B. SOLID EXTRATESTICULAR LESIONS
Important distinction: 50% of paediatric extratesticular solid masses are malignant (usually rhabdomyosarcoma), whereas the vast majority of adult extratesticular solid masses are benign.
5. Epididymitis (Acute)
The most common cause of acute scrotal pain in adults.
Causative organisms: E. coli, Pseudomonas, Aerobacter, Gonococcus, Chlamydia. Tuberculous epididymitis results from secondary spread (via prostatic TB).
Sonological features (Grey-scale):
- Enlarged epididymis (focal or diffuse involvement)
- Heterogeneous and hypoechoic echotexture compared to normal
- The tail and body are most commonly affected
- Associated reactive hydrocele common
- Scrotal wall thickening/oedema
Colour Doppler US:
- Increased colour flow in ALL cases of acute epididymitis - key diagnostic feature
- None of the cases of scrotal pain WITHOUT epididymitis demonstrate this finding
- Doppler differentiates epididymitis from testicular torsion (which shows absent flow)
- If orchitis co-exists (epididymo-orchitis), the testis also shows increased vascularity
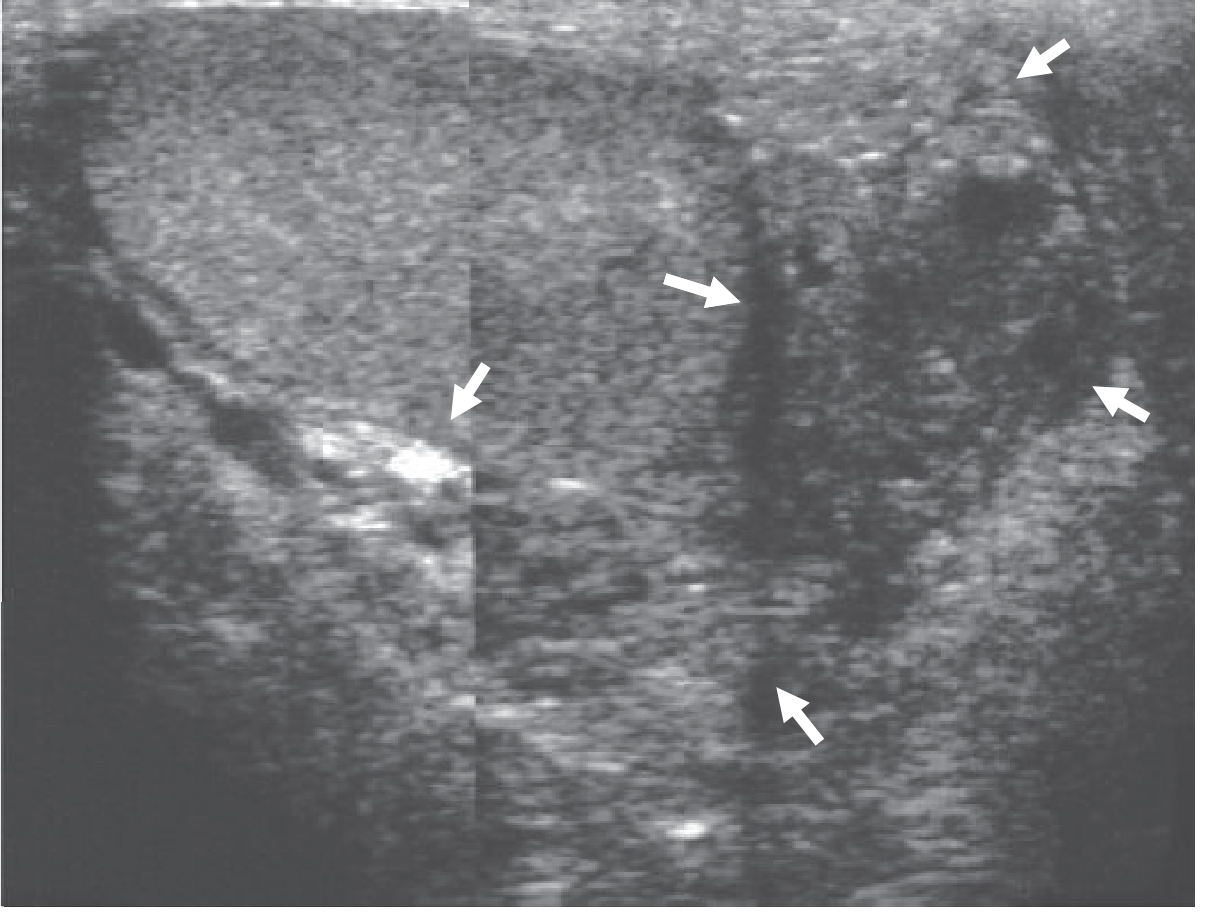
Fig. 33.17 - Acute bacterial epididymitis: the body and tail (arrowed) are heterogeneous and enlarged. The testis is normal.
6. Varicocele
Dilatation of the pampiniform venous plexus of the spermatic cord. Common cause of male infertility. Predominantly left-sided (due to left gonadal vein draining at right angle into left renal vein).
Sonological features:
- Multiple serpiginous, tubular anechoic structures in the spermatic cord, posterior and superior to the testis
- Pampiniform venous diameter >3 mm = abnormal
- Increased diameter on Valsalva manoeuvre / upright position
- Colour Doppler: Retrograde (reversed) venous flow on Valsalva maneuver = diagnostic criterion
- Subclinical varicoceles not palpable on clinical exam can be detected by US + Doppler
Isolated right-sided varicocele on US warrants CT abdomen to exclude retroperitoneal mass causing venous compression.
7. Epididymal Tumours
Adenomatoid tumour: The most common benign epididymal tumour (~30% of paratesticular neoplasms).
Sonological features:
- Well-defined, solid mass
- Echotexture similar to or slightly hyperechoic compared to testis
- Usually no increased Doppler flow
- Size ranges from 3 mm to 5 cm
- Location: tail of epididymis most commonly
Sperm Granuloma: Chronic inflammatory lesion from extravasated sperm.
- Seen following vasectomy, trauma, or infection
- Solid, well-defined, hypoechoic extratesticular mass ≤1 cm
- Located in epididymis or along vas deferens
8. Spermatic Cord Lipoma
- Most common spermatic cord "mass"
- Appears as echogenic fatty tissue within the cord
- No internal vascularity on Doppler
9. Splenogonadal Fusion
A rare benign congenital anomaly - fusion between the developing genital ridge and splenic anlage.
Sonological features:
- Extratesticular solid lesion adjacent to the upper pole of the left testis
- Colour Doppler may show a central feeding vessel branching outward (splenic-type pattern)
- Nuclear medicine (99mTc sulphur colloid scan) confirms ectopic splenic tissue
- Can be mistaken for intratesticular solid lesion, leading to unnecessary orchiectomy if not recognised preoperatively
10. Post-Vasectomy Changes
- Normal late post-vasectomy finding: epididymal enlargement in ~45% of men
- Epididymis appears enlarged but otherwise normal in echogenicity
- No increased Doppler flow (distinguishes from epididymitis)
C. MISCELLANEOUS EXTRATESTICULAR CONDITIONS
Testicular Torsion (Paratesticular component)
- While the testicle itself is involved, the spermatic cord twisting produces extratesticular changes
- Twisted, oedematous spermatic cord may be visible as a "whirlpool sign" on Doppler
- Absent or markedly reduced testicular blood flow on Colour Doppler = torsion
- Reactive hydrocele may be present
Fournier Gangrene (Scrotal Wall)
- Necrotising fasciitis of perineum/scrotum
- US shows thickened scrotal wall with dirty shadowing/gas within scrotal wall
- CT preferred for full extent assessment
D. SUMMARY TABLE
| Lesion | Grey-Scale US | Doppler |
|---|---|---|
| Hydrocele | Anechoic fluid around testis | Not applicable |
| Epididymal cyst | Anechoic, well-defined, epididymal | Avascular |
| Spermatocele | Anechoic, caput epididymis | Avascular |
| Pyocele | Complex loculated fluid, internal echoes | - |
| Acute epididymitis | Enlarged, hypoechoic, heterogeneous epididymis | Increased flow (all cases) |
| Varicocele | Tubular anechoic structures >3mm, spermatic cord | Retrograde flow on Valsalva |
| Adenomatoid tumour | Solid, well-defined, isoechoic/hyperechoic | No increased flow |
| Sperm granuloma | Solid, hypoechoic, ≤1 cm | Avascular |
| Haematocele | Septated complex collection | Variable |
Summary Points (RGUHS Exam)
- US is the first-line imaging for all extratesticular scrotal lesions - no radiation, real-time, cheap
- Key role: Determine intratesticular vs extratesticular location (malignancy risk differs dramatically)
- Extratesticular masses are predominantly benign in adults but 50% malignant in children
- Hydrocele = most common extratesticular cystic lesion; anechoic fluid surrounding testis anteriorly and laterally
- Epididymitis: Enlarged heterogeneous epididymis + increased Colour Doppler flow (differentiates from torsion)
- Varicocele: Tubular anechoic structures >3 mm + retrograde flow on Valsalva on Doppler
- Adenomatoid tumour = most common solid epididymal tumour
- Pyocele = emergency - complex loculated collection with pus echoes
- Doppler US is essential for all solid extratesticular lesions and acute scrotal pain
- Isolated right varicocele on US warrants CT to exclude retroperitoneal pathology
Source: Grainger & Allison's Diagnostic Radiology; Smith & Tanagho's General Urology; Radiopaedia scrotal US
10 mark ans
Asking for Preferences
Above extratesticular scrotal lesions ans
Here is the complete 10-mark RGUHS-style answer for Sonological Evaluation of Extratesticular Scrotal Lesions, formatted exactly as you would write it in an exam:
Sonological Evaluation of Extratesticular Scrotal Lesions
Introduction (1 mark)
Ultrasound (US) is the gold standard imaging modality for evaluation of scrotal pathology. It uses a high-frequency linear array transducer (9-15 MHz) and provides excellent real-time anatomical detail of the testis and all extratesticular structures with no ionising radiation.
The most important role of scrotal US is to determine whether a lesion is intratesticular or extratesticular:
- Intratesticular mass → generally malignant until proven otherwise
- Extratesticular mass → only 3-6% malignant in adults; majority benign
- Exception: In children, 50% of extratesticular solid masses are malignant (usually rhabdomyosarcoma)
Extratesticular lesions are classified as Cystic or Solid.
Technique
- High-frequency linear array transducer: 9-15 MHz
- Patient: supine, scrotum supported on a towel
- Grey-scale + Colour/Power Doppler imaging
- Bilateral comparison ("sunglasses/buddy shot" - both testes side-by-side)
- Valsalva manoeuvre during Doppler for varicocele
A. CYSTIC EXTRATESTICULAR LESIONS (3 marks)
1. Hydrocele
- Most common cause of scrotal swelling
- Congenital: Patent processus vaginalis in neonates; usually resolves spontaneously
- Acquired: Secondary to infection, trauma, tumour, or idiopathic
Sonological features:
- Anechoic (non-reflective) fluid surrounding the anterior and lateral aspects of the testis
- May contain swirling low-level echoes (cholesterol crystals)
- Multiloculated hydrocele may mimic organising haematoma
- US indicated when size prevents clinical palpation of testis (to exclude underlying tumour)
2. Epididymal Cyst / Spermatocele
Both result from dilated epididymal tubules.
- Spermatocele = retention cyst of caput (head) of epididymis; contains spermatozoa
- Epididymal cyst = may occur anywhere in epididymis; does NOT contain sperm; single or multiple
Sonological features:
- Well-defined, discrete, anechoic fluid structure with posterior acoustic enhancement
- Located adjacent to the testis within the epididymis
- Large cysts may superficially resemble a hydrocele
3. Pyocele
Urological emergency - purulent fluid collection within the scrotal sac; rare complication of epididymo-orchitis.
Sonological features:
- Complex, heavily loculated fluid collection
- Multiple low-level internal echoes due to pus
- Thick, irregular walls
- Associated epididymal or testicular abscess
- Must be urgently communicated to the clinical team - risk of Fournier gangrene
4. Haematocele
- Blood within the tunica vaginalis, usually post-traumatic
Sonological features:
- Septated, complex collection; variable echogenicity
- Acutely hyperechoic; becomes more complex/septated over time
- May be indistinguishable from multiloculated hydrocele
B. SOLID EXTRATESTICULAR LESIONS (4 marks)
5. Acute Epididymitis
Most common cause of acute scrotal pain in adults. Organisms: E. coli, Pseudomonas, Gonococcus, Chlamydia. Tuberculous epididymitis is secondary to prostatic TB.
Grey-scale features:
- Enlarged epididymis (whole or focal - body/tail most commonly)
- Heterogeneous, hypoechoic echotexture compared to normal
- Associated reactive hydrocele and scrotal wall thickening
Colour Doppler (KEY FINDING):
- Increased colour flow demonstrated in ALL cases of acute epididymitis
- None of the cases without epididymitis show this - highly specific
- Differentiates epididymitis (increased flow) from testicular torsion (absent flow) - critical distinction
6. Varicocele
Dilatation of the pampiniform venous plexus of the spermatic cord. Predominantly left-sided (left gonadal vein drains at right angle into left renal vein). Important cause of male infertility.
Grey-scale features:
- Multiple serpiginous, tubular anechoic structures posterior and superior to testis in the spermatic cord
- Diameter increases in upright position and with Valsalva
Colour Doppler (DIAGNOSTIC):
- Pampiniform vein diameter >3 mm = abnormal
- Retrograde (reversed) venous flow on Valsalva manoeuvre = diagnostic
- Detects subclinical varicoceles not palpable clinically
Note: Isolated right-sided varicocele on US must prompt CT abdomen to exclude a retroperitoneal mass causing venous obstruction.
7. Adenomatoid Tumour (Most Common Solid Epididymal Tumour)
- Comprises ~30% of all paratesticular neoplasms
- Benign; usually found in the tail of epididymis
Sonological features:
- Well-defined, solid mass; size 3 mm to 5 cm
- Echotexture similar to or slightly hyperechoic compared to testis
- No significant increase in Doppler flow
- No internal vascularity
8. Sperm Granuloma
- Chronic inflammatory reaction to extravasated sperm
- Increased incidence following vasectomy, trauma, or infection
Sonological features:
- Solid, well-defined, hypoechoic extratesticular mass ≤1 cm
- Located in the epididymis or along the vas deferens
- Avascular on Doppler
9. Splenogonadal Fusion
Rare benign congenital anomaly - fusion between genital ridge and splenic anlage. Preoperative misdiagnosis leads to unnecessary orchiectomy in ~1/3 of cases.
Sonological features:
- Extratesticular solid lesion adjacent to upper pole of left testis
- Colour Doppler: central feeding vessel branching outward (splenic vascular pattern)
- Confirmed by 99mTc sulphur colloid nuclear medicine scan
C. SUMMARY TABLE (1 mark)
| Lesion | Grey-Scale US | Doppler Finding |
|---|---|---|
| Hydrocele | Anechoic fluid anterior/lateral to testis | Not applicable |
| Epididymal cyst | Anechoic, well-defined, epididymal | Avascular |
| Spermatocele | Anechoic, caput epididymis | Avascular |
| Pyocele | Complex loculated, internal echoes | - |
| Acute epididymitis | Enlarged, hypoechoic, heterogeneous | Increased flow (all cases) |
| Varicocele | Tubular anechoic >3 mm, spermatic cord | Retrograde flow on Valsalva |
| Adenomatoid tumour | Solid, well-defined, isoechoic | No/minimal flow |
| Sperm granuloma | Solid, hypoechoic, ≤1 cm | Avascular |
| Haematocele | Septated complex collection | Variable |
Conclusion (1 mark)
Scrotal US with Colour Doppler remains the first-line and definitive imaging investigation for extratesticular scrotal lesions. Its ability to:
- Localise a lesion as extratesticular (excluding malignancy in most adult cases)
- Characterise it as cystic or solid
- Assess vascularity in real-time with Doppler
...makes it indispensable. MRI is reserved for troubleshooting when US is inconclusive. The key clinical impact is that US prevents unnecessary surgery for benign lesions while ensuring prompt treatment of emergencies like pyocele and torsion.
Source: Grainger & Allison's Diagnostic Radiology, 6th Ed., Chapter 33 - Extratesticular Scrotal Lesions; Smith & Tanagho's General Urology, 19th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.