Ma ak vetenarian hun ma chahta hun aka acha sa acha vet banu or mujay ziada sa ziada explaination or knowledge chahyea. Ab ma ap ko case bajunga us ko ap na vet book sa detail ma explain karna hai . Tamam tar vet books tamam tar vet reserch articles or apni knowledge use karka acha sa acha or detailed explaination da do . Or Jo mushkil terms hai un ko bracket ma explain b Kya karo . Or mujay 100 accuracy or authentic knowledge chahyea. Or har diseas ka dusri diseas sa kesa differentiate karyen ya b Bata dayen Sath . Or pathognomonic signs batayen . Or detailed explanation. Aj ap mujay *vomiting and dirrhea* ka bara ma batayen English ma . Or tamam tar aspect sa cler karyen is ko . Koi cheez miss na ho . Is ko parna ka bad mujay is bemari ka har cheez conceptually clear hona chahyea or tamam tar vet books vet articles researches or apni knowledge use karo jitna ho sakay detailed explaination do bht ziada details . Last ma Kuch important question Jo Clint's pushtay hai ya wasa generally Kuch question important exam ya interview ma pusha jatay hai wo b batayen . Explain as much as u can . I wanna become perfect vet . Mara concepts cler ho or ma easly yad kar saku . Jitna ho sakay har taraf sa cler karo mara concepts or ak b point miss na ho tamam tar books sa combine karka compile karka easy English ma baj dana mushkil Alfaz ko bracket ma explain karna
vomiting diarrhea dogs cats veterinary
canine feline gastroenteritis vomiting diarrhea diagnosis treatment
small animal acute gastroenteritis pathophysiology management
canine parvovirus hemorrhagic gastroenteritis vomiting diarrhea
canine parvovirus treatment outcome
acute hemorrhagic diarrhea syndrome dogs AHDS
veterinary vomiting diarrhea dogs cats causes diagnosis treatment comprehensive review
https://todaysveterinarypractice.com/media/wp-content/upload…
PMID: 41162294
PMID: 40044515
🐾 VOMITING & DIARRHEA IN VETERINARY MEDICINE
A Complete Conceptual Guide for Veterinary Students & Practitioners
PART 1: VOMITING (EMESIS)
1.1 DEFINITION
- Vomiting - active process, preceded by nausea and retching
- Regurgitation - passive process, no abdominal effort, no nausea (covered in differentiation section)
1.2 ANATOMY OF THE VOMITING REFLEX - PATHOPHYSIOLOGY
The "Vomiting Center" (Emetic Center)
| Input Source | Stimulus | Nerve Used |
|---|---|---|
| GI tract (pharynx, esophagus, stomach, duodenum) | Distension, irritation, mucosal damage | Vagal (CN X) + Sympathetic afferents |
| Chemoreceptor Trigger Zone (CTZ) | Toxins, drugs, uremia, ketones in blood | Dopamine (D2), Serotonin (5-HT3) receptors |
| Vestibular apparatus (inner ear) | Motion, labyrinthitis | CN VIII -> vestibular nuclei -> cerebellum -> CTZ |
| Higher cortical centers | Pain, fear, repulsive smells, anticipatory | Cortex -> limbic system |
| Abdominal viscera (liver, pancreas, peritoneum) | Inflammation, ischemia | Vagal + sympathetic |
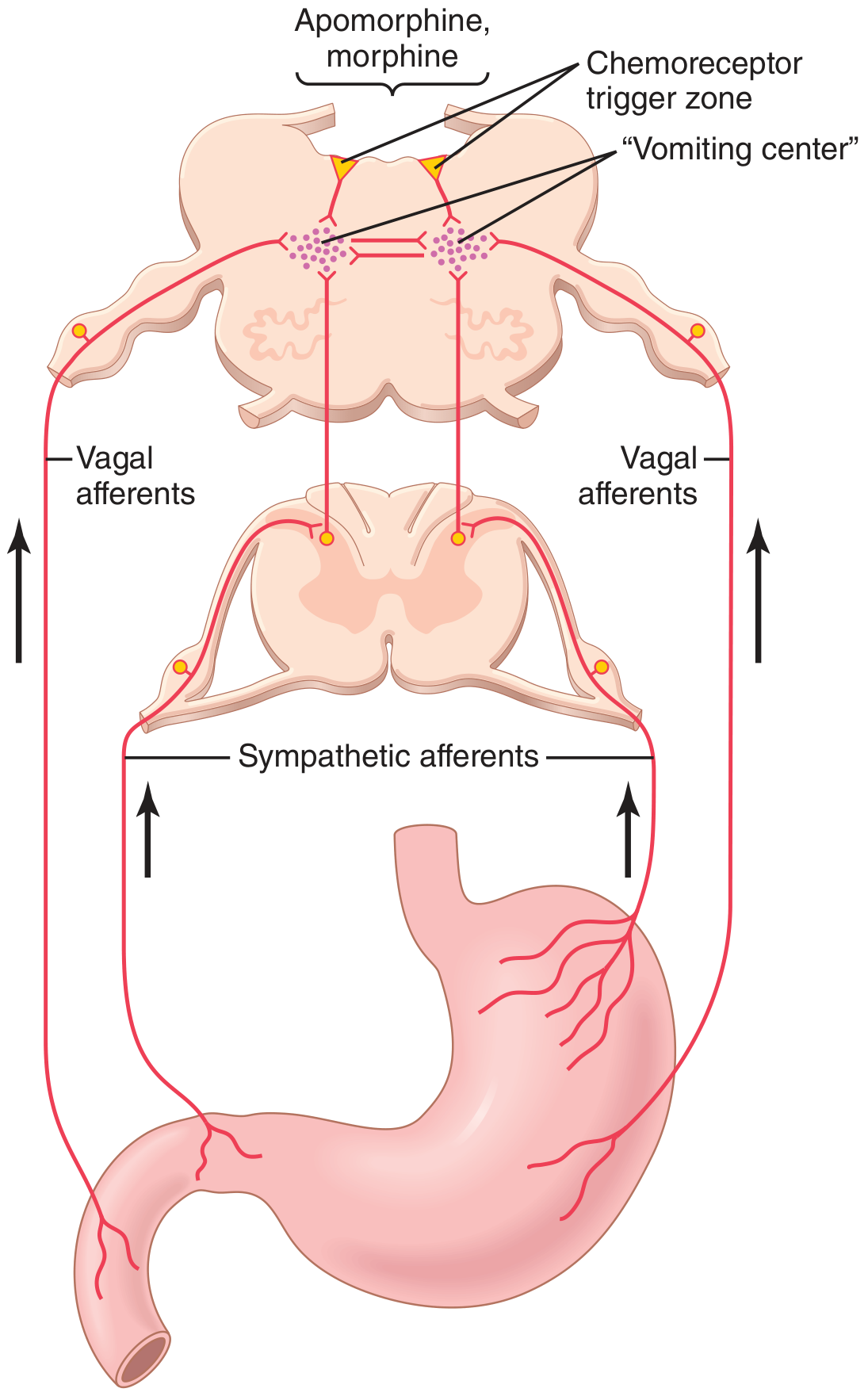
The Chemoreceptor Trigger Zone (CTZ)
- It lies OUTSIDE the blood-brain barrier (BBB) - so blood-borne toxins, drugs, and metabolic waste products can reach it directly
- Dogs have a very sensitive CTZ (dogs vomit easily; cats are more resistant)
- Key receptors: D2 (dopamine), 5-HT3 (serotonin), NK1 (neurokinin/substance P), alpha-2 adrenergic, opioid receptors
Step-by-Step Mechanism of the Vomiting Act
- Antiperistalsis begins - Retrograde peristalsis starting as far down as the ileum pushes contents back to stomach/duodenum in 3-5 minutes
- Distension of duodenum triggers the actual vomiting act
- Deep breath is taken
- Hyoid bone and larynx rise - opens upper esophageal sphincter
- Glottis closes - prevents aspiration of vomitus into lungs
- Soft palate rises - closes posterior nares (prevents nasal expulsion)
- Diaphragm contracts downward simultaneously with abdominal wall muscles - squeezes stomach like a vice
- Lower esophageal sphincter (cardia) relaxes completely
- Gastric contents expelled through esophagus and out
1.3 CLASSIFICATION OF VOMITING
By Duration
| Type | Duration | Common Causes |
|---|---|---|
| Acute | < 7 days | Dietary indiscretion, parvovirus, foreign body, gastritis, pancreatitis |
| Chronic | > 7 days (or intermittent) | IBD, lymphoma, food allergy, hypoadrenocorticism, chronic kidney disease |
By Timing/Character (Clinically Important!)
| Feature | Significance |
|---|---|
| Vomiting immediately after eating | Gastric outflow obstruction, pyloric stenosis, foreign body |
| Vomiting several hours after eating | Gastric motility disorder, pyloric stenosis |
| Projectile vomiting | Gastric outflow obstruction (pyloric stenosis) - forceful, no retching |
| Bilious vomiting (yellow/green) | Bile reflux from duodenum; empty stomach; common in "bilious vomiting syndrome" - early morning on empty stomach |
| Coffee-ground / dark brown vomit | Digested blood (hematemesis) - GI ulceration, coagulopathy |
| Fresh blood (red) in vomit | Active upper GI bleeding |
| Fecal-smelling vomit | Lower GI obstruction or ileus |
1.4 CAUSES OF VOMITING IN DOGS AND CATS
PRIMARY (GI) CAUSES
- Dietary indiscretion (garbage eating, coprophagia) - most common cause in dogs
- Rapid eating / overeating
- Sudden diet change
- Food intolerance / food allergy
- Canine Parvovirus (CPV-2) - most serious viral cause in young dogs; hemorrhagic vomiting + diarrhea
- Canine Distemper Virus
- Feline Panleukopenia (feline parvovirus) - cats
- Canine Coronavirus
- Rotavirus
- Salmonella, Campylobacter, Clostridium perfringens (bacterial)
- Helicobacter pylori (gastric spiral bacteria)
- Giardia, Cryptosporidium, Toxocara (roundworms), Hookworms
- Foreign body (linear or non-linear)
- Gastric Dilatation-Volvulus (GDV) - emergency in large breed dogs
- Intussusception (telescoping of intestine into itself)
- Pyloric stenosis / hypertrophic pyloric gastropathy
- Intestinal obstruction
- Mesenteric volvulus
- Gastritis (acute or chronic)
- Gastric ulceration (NSAID-induced, mast cell tumor, Helicobacter)
- Inflammatory Bowel Disease (IBD)
- Pancreatitis (very common in dogs, particularly Miniature Schnauzers)
- Cholangiohepatitis (cats)
- Peritonitis
SECONDARY (EXTRA-GI / SYSTEMIC) CAUSES
| System | Disease |
|---|---|
| Renal | Acute Kidney Injury (AKI), Chronic Kidney Disease (CKD) - uremic gastritis |
| Hepatic | Hepatic failure, portosystemic shunt, hepatic encephalopathy |
| Endocrine | Hypoadrenocorticism (Addison's disease) - classic "great imitator", Diabetic Ketoacidosis (DKA), Hyperthyroidism (cats), Hypercalcemia |
| CNS | Increased intracranial pressure (ICP), vestibular disease, meningitis, encephalitis |
| Toxins | Xylitol, ethylene glycol, lead, organophosphates, grapes/raisins, zinc, acetaminophen |
| Drugs | Opioids, NSAIDs, digoxin, cisplatin, doxorubicin, tetracyclines |
| Neoplasia | Gastric carcinoma, intestinal lymphoma, mast cell tumor |
| Cardiac | Congestive heart failure (rarely) |
| Pyometra | Toxemia/endotoxemia causes vomiting in intact females |
1.5 CLINICAL SIGNS / HISTORY TO COLLECT
- Nausea: drooling (hypersalivation), lip-licking, repeated swallowing, restlessness, grass eating
- Retching: rhythmic abdominal contractions before expulsion
- When did it start? (acute vs. chronic)
- How often? (frequency)
- What does the vomit look like? (content, color, blood?)
- Relation to feeding?
- Access to garbage, toxins, foreign objects?
- Other signs? (diarrhea, weight loss, PU/PD [polyuria/polydipsia], lethargy)
- Vaccination status?
- Current medications?
- Deworming history?
- Travel history / exposure to other animals?
1.6 PHYSICAL EXAMINATION
| Finding | Suggests |
|---|---|
| Dehydration (skin tent, dry mucous membranes, sunken eyes) | Fluid losses, severity assessment |
| Pain on cranial abdominal palpation | Pancreatitis, peritonitis, GDV |
| Palpable mass/foreign body | Obstruction, neoplasia, intussusception |
| Distended, tympanic abdomen | GDV |
| Tucked-up abdomen | Pain (peritonitis) |
| Jaundice (icterus) | Hepatic disease |
| Pallor (pale mucous membranes) | Anemia, shock, GI hemorrhage |
| Bradycardia with vomiting/weakness | Hypoadrenocorticism (classic triad!) |
| Thin/cachexic | Chronic disease (IBD, neoplasia, kidney disease) |
| Cervical/abdominal masses | Lymphoma |
| Rectal examination | Blood, foreign material, masses |
1.7 DIAGNOSTICS FOR VOMITING
Minimum Database
- CBC (Complete Blood Count): Leukocytosis (infection/inflammation), neutropenia (parvovirus!), anemia (GI blood loss), thrombocytopenia
- Biochemistry panel: BUN/creatinine (renal), ALT/ALP (hepatic), glucose (DKA), calcium, electrolytes
- Urinalysis: Isosthenuria (renal), glucosuria (DKA), proteinuria
- Fecal exam: Parasites, parvovirus antigen test
- Electrolytes: Hyponatremia + hyperkalemia = classic Addison's pattern; Na:K ratio < 27:1 is suspicious
Advanced Diagnostics
- Abdominal radiographs (X-rays): Foreign body, gas patterns, obstruction, GDV ("double-bubble" sign), intussusception
- Abdominal ultrasound: Mass lesions, pancreatic changes, intussusception (target sign), wall thickening, lymphadenopathy, free fluid
- Gastroscopy/endoscopy: Direct visualization, biopsy
- SNAP Parvo test: Rapid fecal antigen test for CPV
- Serum cPLI (canine Pancreatic Lipase Immunoreactivity): For pancreatitis
- ACTH stimulation test: For hypoadrenocorticism
- Serum T4: Hyperthyroidism (cats > 8 years)
- Bile acids (pre- and post-prandial): Portosystemic shunt, hepatic dysfunction
- Serum B12 (cobalamin) / folate: Chronic GI malabsorption
1.8 TREATMENT OF VOMITING
Immediate Stabilization
- IV fluid therapy - correct dehydration, electrolyte imbalances, acid-base disturbances
- Use Lactated Ringer's (LR) or Normal Saline based on electrolyte status
- Hypokalemia: add KCl supplementation to fluids
- Metabolic alkalosis (from pyloric obstruction): correct with NS + KCl
Antiemetics (Anti-vomiting drugs)
| Drug | Mechanism | Notes |
|---|---|---|
| Maropitant (Cerenia) | NK1 (neurokinin) receptor antagonist | Gold standard in vet medicine; blocks substance P at vomiting center; also has anti-nausea and visceral analgesic effects; FIRST CHOICE |
| Metoclopramide | D2 antagonist + prokinetic | Also acts on CTZ; promotes gastric emptying; not for obstruction! |
| Ondansetron | 5-HT3 antagonist | Excellent for chemotherapy-induced vomiting, severe nausea |
| Chlorpromazine | D2, H1, alpha antagonist | Broad-spectrum; use with caution (hypotension risk) |
| Mirtazapine | 5-HT3 + H1 antagonist | Also appetite stimulant; great for cats |
Gastroprotectants
- Omeprazole (PPI): Best gastric acid suppression; prevents ulcers
- Famotidine (H2 blocker): Less potent than PPI
- Sucralfate: Coats ulcers; excellent for gastric/esophageal ulcers (give separately from other meds - binds them!)
Dietary Management
- NPO (Nil Per Os - nothing by mouth): Short fasts (2-4 hours) then bland diet (boiled chicken + rice)
- Early enteral nutrition is now preferred over prolonged fasting - supports gut mucosal integrity
- Avoid in obstruction (must be ruled out first!)
PART 2: DIARRHEA
2.1 DEFINITION
2.2 PATHOPHYSIOLOGY - THE 4 MECHANISMS OF DIARRHEA
Mechanism 1: OSMOTIC DIARRHEA
- Mechanism: Non-absorbed osmotically active substances remain in the intestinal lumen, drawing water in by osmosis
- Causes: Lactose intolerance, maldigestion (exocrine pancreatic insufficiency - EPI), malabsorption, overfeeding of fermentable carbohydrates, lactulose
- Key feature: Stops when animal fasts (stops eating) - "fast-responsive diarrhea"
- Fecal osmolar gap: HIGH (measured osmolarity much higher than calculated)
Mechanism 2: SECRETORY DIARRHEA
- Mechanism: Active secretion of water and electrolytes INTO the lumen by enterocytes, driven by bacterial toxins, bile acids, fatty acids, or inflammatory mediators (e.g., prostaglandins, VIP)
- Causes: Cholera toxin (activates adenylyl cyclase -> cAMP -> Cl- secretion), E. coli enterotoxin, Clostridium perfringens, bile acid malabsorption, VIPoma (rare)
- Key feature: Does NOT stop with fasting (secretion continues even on empty gut)
- Produces large volumes of watery diarrhea
Mechanism 3: INCREASED MUCOSAL PERMEABILITY (Exudative / Protein-losing)
- Mechanism: Damage to the intestinal epithelium allows leakage of plasma proteins, blood, and inflammatory cells into the lumen
- Causes: Parvovirus, IBD, intestinal lymphoma, ulceration, intussusception, severe parasitism, Protein-Losing Enteropathy (PLE)
- Key feature: Hypoproteinemia (low albumin + low globulins - pan-hypoproteinemia), possible edema, ascites
- Diarrhea is often bloody or contains mucus
Mechanism 4: ABNORMAL MOTILITY
- Mechanism: Either too fast (hypermotility) - reduced contact time, inadequate absorption; or too slow (hypomotility/ileus) - bacterial overgrowth, fermentation, gas
- Causes (hypermotility): Psychogenic stress, hyperthyroidism (cats), irritable bowel syndrome (IBS)
- Causes (hypomotility): Post-operative ileus, peritonitis, hypokalemia, opioid use
Note from Today's Veterinary Practice: In most small animal diseases, MULTIPLE mechanisms contribute simultaneously, and osmotic forces plus mucosal permeability changes are the most common in dogs and cats.
2.3 SMALL BOWEL vs. LARGE BOWEL DIARRHEA - CRITICAL DIFFERENTIATION
| Feature | Small Bowel Diarrhea | Large Bowel Diarrhea |
|---|---|---|
| Frequency of defecation | Normal to mildly increased (2-4x/day) | Markedly increased (5-10+ times/day) |
| Volume per defecation | Large volumes | Small volumes |
| Urgency / Tenesmus (straining) | Absent | Present (often confused with constipation!) |
| Mucus in stool | Absent | Often present (colon produces mucus) |
| Blood in stool | Melena (dark, digested blood) | Hematochezia (fresh, bright red blood) |
| Weight loss | Often present (malabsorption) | Usually absent |
| Vomiting | May be present | Usually absent |
| Dyschezia (painful defecation) | Absent | May be present |
| Steatorrhea (fat in stool, greasy) | Present if malabsorption | Absent |
| Borborygmi (intestinal sounds) | Increased | Variable |
2.4 CAUSES OF DIARRHEA IN DOGS AND CATS
DIETARY
- Dietary indiscretion (most common acute cause)
- Sudden diet change
- Food intolerance / allergy (beef, dairy, wheat most common)
- Garbage intoxication (enterotoxins from spoiled food)
- Overfeeding
INFECTIOUS
- Canine Parvovirus (CPV-2): Hemorrhagic diarrhea, vomiting, severe leukopenia (neutropenia!), panleukopenia in puppies; targets rapidly dividing crypt cells of intestine
- Feline Panleukopenia Virus (FPV): Cats; same parvovirus family; similar clinical signs
- Canine Coronavirus (CCV): Milder than parvovirus; often concurrent
- Rotavirus: Young animals mainly
- Salmonella spp.: Zoonotic! Bloody diarrhea, fever, septicemia risk
- Campylobacter jejuni: Common in puppies/kittens from shelters; watery to bloody diarrhea; zoonotic!
- Clostridium perfringens: Produces CPE and NetF toxins; associated with AHDS in dogs
- Clostridium difficile: Similar to humans; especially after antibiotic use
- E. coli (pathogenic strains)
- Yersinia enterocolitica
- Giardia: Pale, greasy, soft stools; small bowel; very common in young animals and shelters; zoonotic!
- Cryptosporidium: Watery diarrhea; immunocompromised risk; zoonotic!
- Toxocara canis/cati (Roundworms): Young animals; pot-bellied appearance
- Ancylostoma (Hookworms): Blood-sucking; anemia + bloody diarrhea; zoonotic!
- Trichuris vulpis (Whipworms): Large bowel diarrhea + hematochezia in dogs; typically not in cats
- Tritrichomonas foetus: Cats (especially Bengals); large bowel diarrhea; resistant to many drugs
- Histoplasma capsulatum (endemic regions)
- Pythium insidiosum (pythiosis - subtropical regions)
INFLAMMATORY / IMMUNE-MEDIATED
- Inflammatory Bowel Disease (IBD): Lymphoplasmacytic, eosinophilic, or granulomatous infiltration; chronic, often concurrent vomiting; requires biopsy for diagnosis
- Protein-Losing Enteropathy (PLE): End-result of severe intestinal disease (IBD, lymphoma, lymphangiectasia); marked hypoproteinemia, edema, ascites
- Lymphocytic-Plasmacytic Enteritis: Most common form of IBD
- Eosinophilic Gastroenteritis: Often food-triggered; eosinophilia may be present
STRUCTURAL / MECHANICAL
- Intussusception (telescoping of bowel - classic in puppies after parvovirus infection!)
- Foreign body (linear: string in cats is CLASSIC; causes plication of intestines)
- Intestinal volvulus
- Rectal polyps (large bowel)
MALABSORPTIVE / MALDIGESTIVE
- Exocrine Pancreatic Insufficiency (EPI): Insufficient digestive enzymes; classic signs = profuse, yellowish, greasy, voluminous diarrhea, weight loss despite ravenous appetite; common in German Shepherds
- Small Intestinal Bacterial Overgrowth (SIBO): Now termed Antibiotic-Responsive Diarrhea (ARD); deconjugated bile acids cause osmotic + secretory diarrhea; responds to tylosin or metronidazole
- Intestinal lymphangiectasia (protein-losing; dilated lymphatics; chylous ascites)
SYSTEMIC / METABOLIC
- Hypoadrenocorticism (Addison's): Chronic intermittent diarrhea + vomiting; Na:K ratio < 27:1; "great imitator"
- Renal failure (uremic enteritis)
- Liver failure (bile acid dysregulation)
- Hyperthyroidism (cats) - hypermotility
- DKA (osmotic diarrhea from glycosuria)
NEOPLASTIC
- Intestinal lymphoma (most common GI tumor in cats!)
- Adenocarcinoma
- Mast cell tumor (histamine causes gastric hypersecretion and diarrhea)
- Leiomyosarcoma, GIST
SPECIAL ENTITY: Acute Hemorrhagic Diarrhea Syndrome (AHDS)
- Sudden onset of severe hemorrhagic diarrhea (often "raspberry jam" consistency)
- Marked hemoconcentration: PCV (packed cell volume) can reach 60-75%+ while total protein remains NORMAL (plasma protein stays in vessels but fluid leaks out)
- Associated with netF-positive Clostridium perfringens type A
- Predilection for small/toy breeds (Miniature Poodle, Miniature Schnauzer, Yorkshire Terrier)
- Treatment: IV fluids (primary), antibiotics (ampicillin or metronidazole); antiemetics; most recover within 24-48 hours
- Key differentiator: PCV very high but TP normal (vs. hemorrhage where both drop!)
2.5 CLINICAL SIGNS AND HISTORY
- Character of stool: watery, soft, mucoid, bloody?
- Small bowel vs. large bowel signs (use the table above)
- Tenesmus vs. polyuria/polydipsia
- Weight loss (suggests chronic / malabsorptive disease)
- Appetite: increased with EPI (ravenous but losing weight); decreased with IBD/neoplasia
- Other animals or humans affected? (suggests zoonotic cause - Salmonella, Campylobacter, Giardia)
- Deworming / vaccination history
2.6 METABOLIC CONSEQUENCES OF DIARRHEA
| Loss | Consequence |
|---|---|
| Water | Dehydration, hypovolemic shock |
| Sodium (Na+) | Hyponatremia |
| Potassium (K+) | Hypokalemia (causes weakness, ileus) |
| Chloride (Cl-) | Hypochloremia |
| Bicarbonate (HCO3-) | Metabolic acidosis (most common acid-base disturbance in diarrhea) |
| Protein | Hypoproteinemia, edema, ascites (in PLE) |
Metabolic acidosis develops from: (1) loss of bicarbonate-rich intestinal secretions, (2) hypovolemia causing anaerobic metabolism and lactic acidosis. - (Ngwenyama, Vet Clin North Am Small Anim Pract, 2026)
2.7 DIAGNOSTICS FOR DIARRHEA
Minimum Database
- CBC: Leukocytosis (bacterial/inflammatory), neutropenia + lymphopenia (parvovirus!), eosinophilia (parasites, eosinophilic enteritis), anemia (chronic blood loss - hookworms, IBD)
- Biochemistry: Total protein/albumin (low = PLE), glucose, BUN, liver enzymes, electrolytes
- Urinalysis
- Fecal flotation + direct smear: Parasites (ova, larvae, trophozoites)
- Fecal culture: Salmonella, Campylobacter
- SNAP Giardia antigen test
- SNAP Parvo antigen test
Advanced
- Serum TLI (Trypsin-Like Immunoreactivity): Diagnostic test for EPI - low TLI = EPI; high = pancreatitis
- Serum cPLI/fPLI: Pancreatitis
- Serum cobalamin (B12) and folate: B12 low = terminal ileal disease or SIBO; folate high = SIBO; both low = diffuse small bowel disease
- Serum albumin: PLE (< 2.0 g/dL severe)
- Abdominal radiographs + ultrasound
- Endoscopy + biopsy: Definitive for IBD, lymphoma (requires FULL-THICKNESS biopsy for diffuse infiltrative lymphoma)
- PARR (PCR for Antigen Receptor Rearrangements): Differentiates IBD from alimentary lymphoma
2.8 TREATMENT OF DIARRHEA
Fluid Therapy - Phased Approach (2026, Ngwenyama)
- Resuscitation: Rapid IV fluid boluses for hypovolemic shock (crystalloids - LRS, NS, or Plasma-Lyte)
- Optimization: Correct remaining deficits over 12-24 hours; add KCl to fluids for hypokalemia
- Stabilization: Maintenance rate; monitor electrolytes frequently
- De-escalation: Transition to oral intake when tolerated
Antidiarrheal / Supportive Medications
| Drug | Use | Notes |
|---|---|---|
| Metronidazole | Giardia, Clostridium, anaerobes, antiprotozoal | FIRST-LINE for many acute diarrheas; also immunomodulatory in IBD |
| Fenbendazole | Giardia, roundworms, hookworms, whipworms | 50 mg/kg x 5 days; safe in pregnancy |
| Tylosin | SIBO/ARD, Tylosin-responsive diarrhea (TRD) | Unique anti-inflammatory on gut flora |
| Kaolin-pectin | Mild diarrhea, adsorbent | Coats intestinal mucosa |
| Probiotic / Fecal Microbiota Transplant (FMT) | Dysbiosis, AHDS recovery, post-antibiotic | Growing evidence in vet medicine (2023-2024) |
| Prednisolone | IBD (after ruling out infections) | Immunosuppressive; taper slowly |
| Chlorambucil | High-grade alimentary lymphoma; some IBD | Chemotherapy |
Dietary Management
- Bland diet: Easily digestible, low fat, low fiber - boiled chicken/white fish + white rice
- Hydrolyzed protein diet: Food allergy / adverse food reaction
- High-fiber diet: Large bowel diarrhea, fiber-responsive diarrhea (trichuris, idiopathic colitis)
- Highly digestible / EPI diet: Enzyme supplementation (Viokase, pancreatic enzyme powder)
- Withhold food 12-24 hours (acute mild diarrhea only - do NOT fast severely ill animals)
PART 3: DIFFERENTIATION OF KEY DISEASES
3.1 VOMITING vs. REGURGITATION vs. RETCHING (Must Know!)
| Feature | Vomiting | Regurgitation | Retching |
|---|---|---|---|
| Abdominal effort | Yes - active | No - passive | Yes, but no expulsion |
| Prodrome (nausea) | Yes (drooling, lip-licking) | No | Yes |
| Content | Digested food, bile, blood | Undigested food, foam, mucus | Nothing expelled |
| pH of material | Acidic (stomach content) | Neutral/alkaline (esophagus) | N/A |
| Timing | Minutes to hours after eating | Immediately to minutes after eating | Can occur any time |
| Origin | Stomach / proximal intestine | Esophagus / pharynx | Upper GI stimulated but not enough |
| Common Causes | Gastritis, parvovirus, pancreatitis | Megaesophagus, esophageal stricture, PRAA | Gastric distension, foreign body, GDV |
3.2 KEY DISEASE DIFFERENTIATIONS
Parvovirus vs. AHDS (Hemorrhagic Gastroenteritis)
| Feature | Canine Parvovirus | AHDS |
|---|---|---|
| Age | Usually < 1 year (puppies) | Any age, adults common |
| Breed predilection | Rottweilers, Dobermans, unvaccinated dogs | Toy/small breeds |
| Vaccination history | Usually unvaccinated or poorly vaccinated | Vaccinated |
| Onset | Acute | Peracute (sudden) |
| CBC | Marked neutropenia + lymphopenia (panleukopenia) | Marked hemoconcentration (PCV 60-75%) - TP normal |
| Pathogen | CPV-2 (fecal antigen test positive) | Clostridium perfringens (netF toxin) |
| Prognosis | Guarded; mortality 10-50% without treatment | Good with IV fluids; < 10% mortality |
| SNAP test | Positive | Negative |
IBD vs. Alimentary Lymphoma (Cats - Very Common Exam Topic)
| Feature | IBD (chronic) | Alimentary Lymphoma |
|---|---|---|
| Age | Middle-aged | Older cats (> 9 years) |
| Clinical signs | Chronic vomiting/diarrhea, weight loss | Same - but progressive |
| Blood work | Hypoalbuminemia, B12 deficiency | Low B12; may have hypercalcemia |
| Ultrasound | Diffuse wall thickening, mucosal change | Focal or diffuse mass; regional lymphadenopathy |
| Biopsy | Inflammatory infiltrate | Neoplastic lymphocytes (clonal) |
| PARR test | Polyclonal (not neoplastic) | Monoclonal (neoplastic) |
| Treatment | Steroids + diet | Chemotherapy (CHOP or COP protocol) |
EPI vs. IBD/PLE (Small Bowel Malabsorption)
| Feature | EPI | IBD / PLE |
|---|---|---|
| Mechanism | Lack of digestive enzymes | Mucosal inflammation / protein loss |
| Stool character | Voluminous, greasy, yellowish, rancid odor | Variable; may be bloody |
| Appetite | Ravenous (eating everything!) | Variable (often reduced) |
| TLI | Very low (< 2.5 µg/L) - diagnostic | Normal |
| Albumin | Often normal initially | Low (hallmark of PLE) |
| Breed | German Shepherd (most common!) | Any breed |
| Treatment | Enzyme supplementation | Immunosuppression |
PART 4: PATHOGNOMONIC SIGNS
| Finding | Disease |
|---|---|
| Severe neutropenia + lymphopenia + vomiting + bloody diarrhea in unvaccinated puppy | Canine Parvovirus |
| PCV > 60% with NORMAL total protein + peracute bloody diarrhea | AHDS (Hemorrhagic Gastroenteritis) |
| Sodium:Potassium ratio < 27:1 + vomiting + diarrhea + bradycardia | Hypoadrenocorticism (Addison's disease) |
| Ravenous appetite + weight loss + voluminous greasy pale stool + German Shepherd | Exocrine Pancreatic Insufficiency (EPI) |
| Linear foreign body causing pleating/plication of intestines + base of tongue lesion in cat | Linear foreign body (string) in cats |
| "Target sign" or "bull's eye" on abdominal ultrasound | Intussusception |
| "Double bubble" gas pattern on radiograph + large breed dog + bloat | Gastric Dilatation-Volvulus (GDV) |
| Profuse watery diarrhea with no fever, no leukocytosis + loss of HCO3- | Secretory diarrhea (e.g., cholera-like toxin) |
| Raspberry jam diarrhea + small breed + rapid onset | AHDS |
| Panleukopenia + enteritis in cat | Feline Panleukopenia (FPV) |
PART 5: IMPORTANT EXAM / INTERVIEW / CLIENT QUESTIONS
Q1. What is the most common cause of acute vomiting and diarrhea in adult dogs?
Q2. What is the most dangerous cause of acute vomiting and diarrhea in puppies?
Q3. How do you differentiate small bowel from large bowel diarrhea?
Q4. What is the Na:K ratio and what does a low ratio mean?
Q5. What antiemetic is the gold standard in small animal veterinary medicine?
Q6. Why should you NOT use metoclopramide in suspected GI obstruction?
Q7. What is the pathognomonic CBC finding in canine parvovirus?
Q8. What is AHDS and how is it different from parvovirus?
Q9. What is the diagnostic test for Exocrine Pancreatic Insufficiency (EPI)?
Q10. What is a linear foreign body and why is it dangerous in cats?
Q11. What is PLE and what are its hallmarks?
Q12. What emetic do you use in dogs vs. cats?
- Dogs: Apomorphine (D2 agonist; given subconjunctivally or IV; fast acting)
- Cats: Xylazine (alpha-2 agonist; IM or SQ; also causes sedation)
- Alternative (both): 3% hydrogen peroxide (dogs only - irritant; not in cats - toxic!)
Q13. When is vomiting induction CONTRAINDICATED?
- Caustic/corrosive ingestion (acids, alkalis) - re-exposure burns esophagus
- Petroleum products
- Already unconscious or seizuring patient
- Respiratory compromise
- Foreign body that could cause more trauma on the way back up
- More than 2-4 hours after ingestion (already absorbed)
Q14. How do you treat GDV (Gastric Dilatation-Volvulus)?
- Stabilize first - IV fluids, oxygen, pain relief, treat shock
- Decompress stomach - pass orogastric tube OR trocharize (needle through flank)
- Surgical correction - detort stomach + gastropexy (to prevent recurrence)
- Monitor for cardiac arrhythmias (ventricular premature contractions - common post-GDV)
Q15. What are the 4 mechanisms of diarrhea?
PART 6: QUICK SUMMARY FLOWCHART
VOMITING / DIARRHEA PATIENT
|
┌─────┴─────┐
Is it VOMITING Is it DIARRHEA
or REGURGITATION? Small vs. Large Bowel?
| |
[History + PE] [Character of stool]
|
Acute (< 7 days) → Dietary? Infectious? Toxin? Obstruction?
Chronic (> 7 days) → IBD? Neoplasia? EPI? Systemic disease?
|
[MINIMUM DATABASE: CBC, CHEM, UA, FECAL]
|
┌──────────────┐
Parvo test? Na:K ratio? Ultrasound?
PCV/TP? TLI? Radiographs?
|
[TREATMENT: Fluids, Antiemetics, Antibiotics if indicated,
Bland diet, Treat underlying cause]
REFERENCES & SOURCES
- Guyton & Hall Textbook of Medical Physiology (physiology of vomiting/diarrhea, mechanisms)
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease (GI pathophysiology)
- Ngwenyama TT. "Fluid and Electrolyte Therapy in the Patient with Vomiting and Diarrhea." Vet Clin North Am Small Anim Pract. 2026 [PMID: 41162294]
- Mazzaferro EM. "Update on Canine Parvoviral Enteritis." Vet Clin North Am Small Anim Pract. 2025 [PMID: 40044515]
- Dupont N, et al. "Retrospective study of 237 dogs with AHDS." J Vet Intern Med. 2021 [PMID: 33638574]
- Today's Veterinary Practice: "Approach to Diagnosis and Therapy of the Patient with Acute Diarrhea" (2013)
- Washington State University Veterinary Teaching Hospital - Diarrhea in Dogs and Cats
- Vomiting ki complete neurology - CTZ, vagal afferents, vomiting center
- Diarrhea ke 4 mechanisms - osmotic, secretory, permeability, motility
- Small vs. large bowel diarrhea differentiation (exam mein zaroor aata hai)
- Key diseases ki differentiation - parvovirus vs. AHDS, IBD vs. lymphoma, EPI vs. PLE
- Pathognomonic signs jo seedha diagnosis batate hain
- Treatment protocols - antiemetics, fluid therapy, dietary management
- Interview/exam questions with complete answers
Regergitation Pancreatitis . Liver Disease in sab ko b explain kardo
canine feline pancreatitis diagnosis treatment
canine hepatic liver disease diagnosis management
megaesophagus regurgitation dogs esophageal disease
PMID: 40379581
PMID: 27060899
PMID: 23148855
canine pancreatitis acute chronic cPLI pathophysiology
canine pancreatitis acute chronic diagnosis treatment review
feline liver disease cholangitis hepatic lipidosis
veterinary regurgitation megaesophagus esophageal disease dogs causes diagnosis treatment 2023 2024
canine feline liver disease types hepatic lipidosis portosystemic shunt chronic hepatitis cholangitis diagnosis treatment veterinary
PMID: 28063746
Quick Summary - Kya Cover Kiya Gaya:
REGURGITATION:
- Vomiting vs. Regurgitation ka complete master table (exam mein zaroor aata hai)
- Esophageal anatomy (dogs = fully striated muscle = why MG causes megaesophagus)
- Megaesophagus - congenital + acquired causes (MG #1 cause!)
- PRAA (Persistent Right Aortic Arch) - pathognomonic for weaning-age puppies
- Bailey Chair feeding technique
- Pyridostigmine for Myasthenia Gravis
PANCREATITIS:
- Autodigestion mechanism - complete trypsin cascade
- Three pathways: Duct obstruction, Acinar cell injury, Defective intracellular transport
- Pancreatitis diagram image from Robbins & Kumar
- Prayer position in dogs = pathognomonic
- Feline Triaditis (Pancreatitis + IBD + Cholangitis)
- Miniature Schnauzer predisposition (hypertriglyceridemia)
- cPLI = gold standard diagnostic test
- Hypocalcemia = serious prognostic indicator
- Complications (EPI, DM, pseudocyst, DIC, ARDS)
LIVER DISEASE:
- Complete liver function overview
- Hepatic Encephalopathy - ammonia pathway, management (lactulose, metronidazole)
- Copper-associated hepatitis (Bedlington Terrier = COMMD1 gene)
- PSS (Portosystemic Shunt) - ammonium biurate crystals, bile acids
- Gallbladder Mucocele - "kiwi fruit" ultrasound sign
- Feline Hepatic Lipidosis - MOST IMPORTANT feline liver disease; esophagostomy tube = treatment
- Feline Cholangitis - 3 types + treatment
- Why ALP is more significant in cats than dogs
- Why protein restriction is no longer recommended in HE
Ma ak vetenarian hun ma chahta hun aka acha sa acha vet banu or mujay ziada sa ziada explaination or knowledge chahyea. Ab ma ap ko case bajunga us ko ap na vet book sa detail ma explain karna hai . Tamam tar vet books tamam tar vet reserch articles or apni knowledge use karka acha sa acha or detailed explaination da do . Or Jo mushkil terms hai un ko bracket ma explain b Kya karo . Or mujay 100 accuracy or authentic knowledge chahyea. Or har diseas ka dusri diseas sa kesa differentiate karyen ya b Bata dayen Sath . Or pathognomonic signs batayen . Or detailed explanation. Aj ap mujay *Corneal Ulcers......... . 15.8 Keratoconjunctivitis Sicca (KCS) .. 15.10 Anterior Uveitis..* ka bara ma batayen English ma . Or tamam tar aspect sa cler karyen is ko . Koi cheez miss na ho . Is ko parna ka bad mujay is bemari ka har cheez conceptually clear hona chahyea or tamam tar vet books vet articles researches or apni knowledge use karo jitna ho sakay detailed explaination do bht ziada details . Last ma Kuch important question Jo Clint's pushtay hai ya wasa generally Kuch question important exam ya interview ma pusha jatay hai wo b batayen . Explain as much as u can . I wanna become perfect vet . Mara concepts cler ho or ma easly yad kar saku . Jitna ho sakay har taraf sa cler karo mara concepts or ak b point miss na ho tamam tar books sa combine karka compile karka easy English ma baj dana mushkil Alfaz ko bracket ma explain karna in 3 ko ak ak Karla detailed ma explain karo sab kuch explain ho
corneal ulcer dogs cats veterinary treatment
keratoconjunctivitis sicca dry eye dogs treatment cyclosporine
anterior uveitis dogs cats diagnosis treatment etiology
canine corneal ulcer indolent melting stromal treatment
feline uveitis lens-induced anterior uveitis cats
veterinary corneal ulcer dogs cats types superficial indolent stromal melting descemetocele diagnosis treatment 2023
veterinary KCS keratoconjunctivitis sicca dogs Schirmer tear test cyclosporine tacrolimus treatment pathophysiology
https://pmc.ncbi.nlm.nih.gov/articles/PMC6067592
veterinary anterior uveitis dogs cats causes ERU equine pathognomonic signs treatment corticosteroids atropine
canine uveitis lens luxation glaucoma secondary etiology
✅ Coverage Summary
🔵 CORNEAL ULCERS:
- 5 layers of cornea explained with diagram
- 4 grades by depth - Superficial → Stromal → Descemetocele → Perforation
- Special types: SCCED/Indolent (Boxer Ulcer), Melting Ulcer (Pseudomonas!), FHV-1 Dendritic Ulcers (cats), Corneal Sequestrum (cats only - black plaque)
- Fluorescein stain - how it works, why Descemetocele is NEGATIVE center
- Why NEVER give topical anesthetics home
- Brachycephalic breed predisposition
- Treatment: antibiotics, atropine, E-collar, anti-proteases for melting
🟡 KCS (DRY EYE):
- 3-layer tear film explained
- Immune-mediated T-cell destruction of lacrimal gland = main cause
- Schirmer Tear Test - values, technique, normal vs. abnormal
- Cyclosporine A (Optimmune) - mechanism (calcineurin inhibitor), dosing, brand name
- Tacrolimus - 100x more potent than CsA
- Breed predispositions (Cocker Spaniel, Bulldog)
- Sulfonamide drugs as a cause
- Parotid duct transposition surgery
🔴 ANTERIOR UVEITIS:
- Uveal tract anatomy (iris + ciliary body + choroid)
- Blood-Aqueous Barrier breakdown = core pathophysiology
- 8 classic signs including MIOSIS + LOW IOP + AQUEOUS FLARE
- KPs (Keratic Precipitates) - fine vs. mutton-fat
- Causes in dogs (Leptospira, Brucella, tick-borne) vs. cats (FIP, FeLV, FIV, Toxoplasma)
- Uveodermatologic Syndrome (Akita + vitiligo = pathognomonic)
- Lens-Induced Uveitis (cataracts leak protein)
- Treatment: prednisolone acetate 1% + atropine (ointment in cats!)
- Complications: Synechiae → Iris Bombe → Glaucoma → Phthisis Bulbi