Telle me how to diagnoseulm embolism
Reading File
Finding Sources
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive content to write a thorough answer. Let me compile everything.
Diagnosis of Pulmonary Embolism (PE)
Pulmonary embolism (PE) is a potentially fatal condition where a blood clot (usually from a deep vein thrombosis) lodges in the pulmonary vasculature. Diagnosis requires integrating clinical probability scoring, laboratory tests, and imaging in a stepwise fashion.
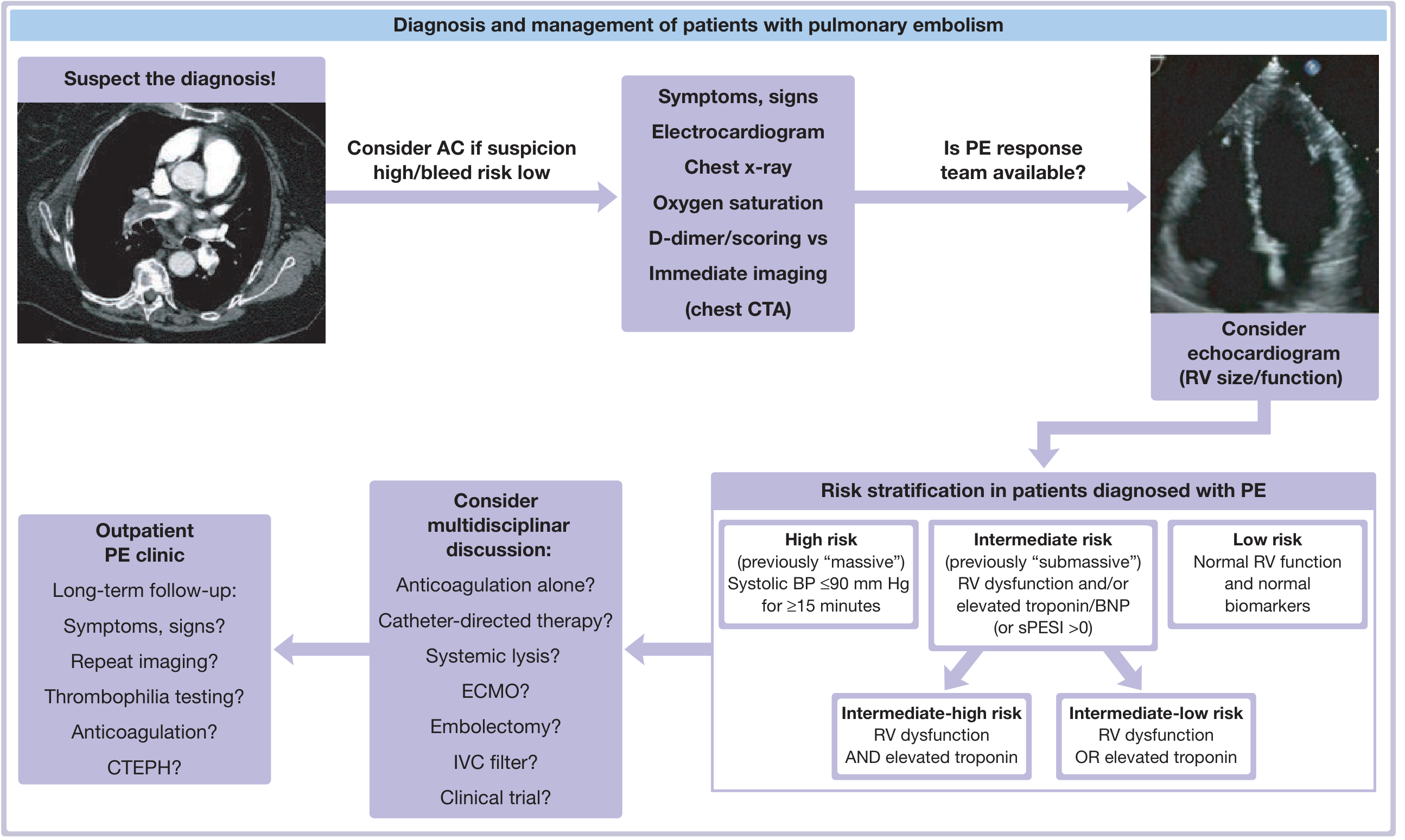
Fuster and Hurst's The Heart, 15th Ed. - Central Illustration: Diagnosis and Management of PE
1. Symptoms and Signs (Suspect the Diagnosis!)
The most important first step is clinical suspicion. PE is commonly missed because its presentation is nonspecific.
Symptoms:
- Dyspnea (most common), pleuritic chest pain, hemoptysis
- Angina-like chest pain, palpitations
- Wheezing, syncope
Signs:
- Tachycardia, tachypnea, hypotension (in severe/massive PE)
- Leg swelling and tenderness (suggesting DVT as source)
- Neck vein distension or right ventricular S3 (signs of RV failure)
- Fever, visible anxiety, chest wall tenderness (with pulmonary infarction)
- Reduced oxygen saturation
The PIOPED study found that >90% of PE patients had at least one of: dyspnea, tachycardia, or pleuritic chest pain. (Fishman's Pulmonary Diseases)
2. Differential Diagnosis
Before pursuing PE workup, consider mimics: acute MI, aortic dissection, pneumothorax, pneumonia, congestive heart failure, pleuritis, pericarditis, costochondritis, and anxiety.
3. Clinical Probability Scoring
A structured pre-test probability score must be calculated before ordering tests. Three validated tools exist:
Wells Score (most widely used)
| Variable | Points |
|---|---|
| Clinical signs/symptoms of DVT | +3 |
| PE is the #1 diagnosis, or equally likely | +3 |
| Heart rate >100/min | +1.5 |
| Immobilization ≥3 days or surgery in previous 4 weeks | +1.5 |
| Previous DVT or PE | +1.5 |
| Hemoptysis | +1 |
| Malignancy (treatment ongoing, or within last 6 months) | +1 |
- Score ≤4 = PE unlikely
- Score >4 = PE likely (proceed to imaging)
Revised Geneva Score (no blood gas required)
| Variable | Points |
|---|---|
| Age ≥65 years | 1 |
| Previous DVT or PE | 3 |
| Surgery or fracture within 1 month | 2 |
| Active malignancy | 2 |
| Hemoptysis | 2 |
| Heart rate 75-94/min | 3 |
| Heart rate >95/min | 5 |
| Unilateral lower limb pain | 3 |
| Pain on deep palpation and unilateral edema | 4 |
Simplified Geneva score <2 + normal D-dimer = ~3% probability of PE.
PERC Rule (to rule out PE without further testing)
PE can be ruled out if ALL 8 are absent AND pre-test probability is ≤15%:
- Age <50 years
- Pulse <100/min
- O2 saturation >94%
- No unilateral leg swelling
- No hemoptysis
- No recent surgery/trauma
- No prior DVT/PE
- No oral contraceptive use
Sensitivity 97.4%, specificity 21.9%. (Fuster and Hurst's The Heart, 15th Ed.)
YEARS Algorithm (newer)
Three items: (1) clinical signs of DVT, (2) hemoptysis, (3) PE most likely diagnosis, plus D-dimer thresholds:
- No YEARS items + D-dimer <1000 ng/mL → PE excluded
- ≥1 YEARS items + D-dimer <500 ng/mL → PE excluded
- All others → proceed to CT angiography
4. Laboratory Tests
D-Dimer
- A breakdown product of cross-linked fibrin
- Measured by high-sensitivity ELISA or ELISA-derived assay
- Sensitivity and NPV ≥95% when below the cutoff
- Use to exclude PE in low-to-moderate pre-test probability patients
- Not useful in hospitalized patients - many comorbidities elevate it non-specifically
- Age-adjusted cutoff: D-dimer threshold = age × 10 ng/mL (in patients >50 years) increases specificity without sacrificing sensitivity
Troponin & BNP/NT-proBNP
- Used for risk stratification after diagnosis, not to diagnose PE
- Elevated troponin = RV myocardial injury
- Elevated BNP/NT-proBNP = RV strain
- Their combination with RV dysfunction on echo helps stratify intermediate vs. high risk
Arterial Blood Gas (ABG)
- Typically shows hypoxemia, hypocapnia (from hyperventilation), and a raised A-a gradient
- Not diagnostic on its own but supports suspicion
- An O2 saturation of 95% doesn't rule out PE - the patient may be working hard to maintain it
5. Electrocardiogram (ECG)
ECG findings are generally nonspecific but important to obtain:
- Sinus tachycardia - most common finding
- S1Q3T3 pattern - classic but present in only ~20% of cases
- Right bundle branch block (complete or incomplete)
- Right axis deviation
- T-wave inversions in V1-V4 (RV strain pattern)
- ST-segment abnormalities
ECG is essential to rule out MI and to suggest RV strain in the right clinical context.
6. Chest X-Ray (CXR)
CXR is usually abnormal but nonspecific. Key findings:
- Atelectasis and parenchymal opacity - most common findings (PIOPED data)
- Hampton's hump - wedge-shaped pleural-based opacity (pulmonary infarction)
- Westermark sign - focal oligemia (area of decreased vascularity)
- Palla's sign - enlarged right descending pulmonary artery
- Normal CXR in a hypoxic, dyspneic patient should raise suspicion for PE
CXR also helps determine whether a V/Q scan is appropriate (abnormal CXR reduces V/Q scan utility). (Fishman's Pulmonary Diseases)
7. Imaging
CT Pulmonary Angiography (CTPA) - Gold Standard
- The primary and preferred imaging modality for diagnosing PE
- Direct visualization of clot in pulmonary arteries
- High sensitivity (~83%) and specificity (~96%)
- Also detects alternative diagnoses in ~17-19% of cases
- MDCT-PA (multidetector CT) has replaced conventional pulmonary angiography in most centers
- Contraindications: severe contrast allergy, renal impairment, pregnancy (relative)
Ventilation-Perfusion (V/Q) Scan
- Preferred when CTPA is contraindicated (renal failure, contrast allergy, pregnancy)
- Results reported as: normal, very low, low, intermediate, or high probability
- High-probability scan + high clinical probability → treat for PE
- Normal scan → effectively excludes PE
- PIOPED showed the problem: most patients get an intermediate probability scan, which requires further testing
- Sensitivity/specificity vary depending on underlying lung disease (COPD worsens accuracy significantly)
- Intermediate scans occurred in 60% of COPD patients vs. only 13% in those with normal CXR (PIOPED)
Pulmonary Angiography (Conventional)
- Historical "gold standard" - now rarely used
- Replaced by CTPA
- Still used in select cases (e.g., prior to catheter-directed therapy)
Echocardiography
- Not diagnostic for PE in most cases, but extremely useful for:
- Detecting RV dilation and dysfunction (RV:LV ratio >0.9)
- Assessing hemodynamic compromise
- Risk stratification after diagnosis
- Bedside evaluation in hemodynamically unstable patients (to identify massive PE quickly)
- Rarely, a clot may be visualized directly in the right heart or main pulmonary artery
MRI/MRA
- Limited utility; lower sensitivity than CTPA
- Used in special circumstances (e.g., pregnancy, contrast allergy)
Compression Ultrasonography (CUS) for DVT
- Useful when PE is suspected but CTPA cannot be done
- Positive CUS (non-compressibility of vein) in a patient with PE symptoms = treat for VTE
- Sensitivity for DVT is lower in pregnancy due to prevalence of isolated pelvic DVT
8. Diagnostic Strategy
Hemodynamically UNSTABLE (shock/hypotension):
- Immediate bedside echocardiography
- If RV dilation or clot-in-transit seen → treat for massive (high-risk) PE immediately
- CTPA if patient can be stabilized
Hemodynamically STABLE:
- Calculate pre-test probability (Wells / Geneva / PERC)
- Low probability: D-dimer → if negative, PE excluded; if positive → CTPA
- Moderate probability: D-dimer → if negative, PE excluded; if positive → CTPA
- High probability: go straight to CTPA (don't wait for D-dimer result, start anticoagulation)
Key principle: Consider starting anticoagulation before diagnosis is confirmed if pre-test probability is high and bleeding risk is acceptable. (Fuster and Hurst's The Heart, 15th Ed.)
9. Risk Stratification After Diagnosis
Once PE is confirmed, classify into:
| Category | Criteria |
|---|---|
| High-risk (previously "massive") | Systolic BP ≤90 mmHg for ≥15 minutes |
| Intermediate-high risk | RV dysfunction AND elevated troponin |
| Intermediate-low risk | RV dysfunction OR elevated troponin |
| Low risk | Normal RV function and normal biomarkers |
The simplified PESI (sPESI) score is also used: score >0 = not low risk.
Sources:
- Fuster and Hurst's The Heart, 15th Edition, Chapter 58 (Diagnosis of DVT and PE)
- Fishman's Pulmonary Diseases and Disorders, Chapter 30 (PIOPED study; V/Q scanning)
- 2025 ESVM Guidelines on VTE interventional treatment (PMID: 40587333)
Find recent guidelines on PE management and treatment options
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND "management"[MeSH Terms]
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND "anticoagulants"[MeSH Terms]
Finding Sources
Reading Article
PMID: 41712677
Reading Article
PMID: 40578592
Finding Sources
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND "catheter directed thrombolysis"
Reading Article
PMID: 39470698
Reading Article
PMID: 40602356
Reading File
Loading Image
Reading File
Reading File
I have comprehensive content on all treatment modalities. I have enough to write a thorough, well-cited answer now.
Recent Guidelines on Pulmonary Embolism Management and Treatment Options
Guideline Landscape (2025-2026)
The most current and authoritative guidance comes from the 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Joint Guideline (published March/April 2026 in Circulation and JACC). A key feature of this guideline is the introduction of new AHA/ACC Acute PE Clinical Categories to sharpen severity classification and therapy decisions. It covers the full period from symptom onset through clinical follow-up. 2026 AHA/ACC PE Guideline (PMID: 41712677)
Step 1: Risk Stratification - The Foundation of All Treatment Decisions
Treatment intensity is entirely driven by risk category. Before any therapy is chosen, patients must be classified.
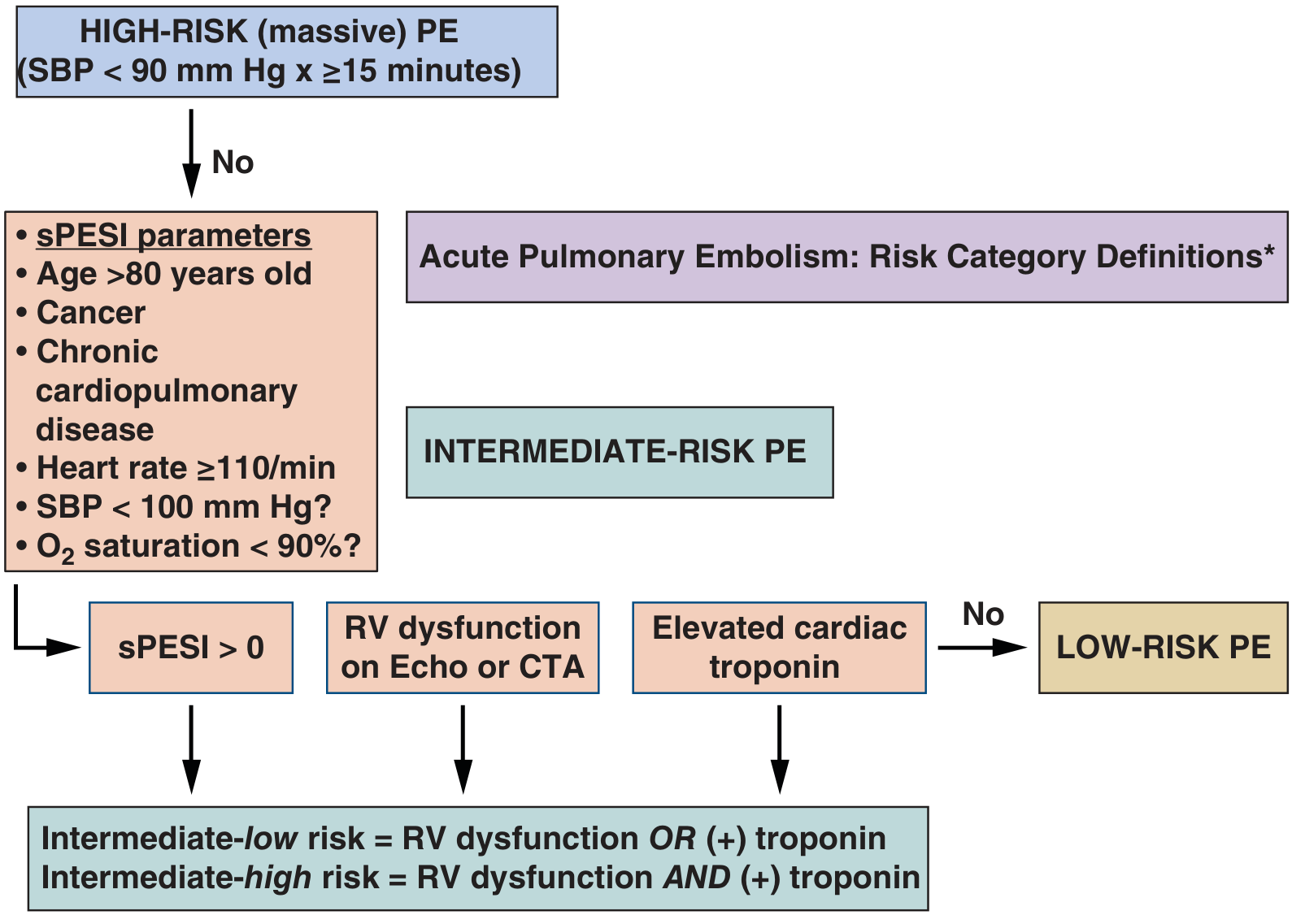
| Risk Category | Definition |
|---|---|
| High-risk (previously "massive") | SBP ≤90 mmHg for ≥15 minutes |
| Intermediate-high risk | sPESI >0 + RV dysfunction (echo or CTA) AND elevated troponin |
| Intermediate-low risk | sPESI >0 + RV dysfunction OR elevated troponin |
| Low-risk | Normal RV function + normal biomarkers; sPESI = 0 |
sPESI parameters (1 point each): age >80, cancer, chronic cardiopulmonary disease, HR ≥110/min, SBP <100 mmHg, O2 sat <90%.
Step 2: Immediate Supportive Measures
Regardless of risk, all unstable patients receive:
- Oxygen supplementation / mechanical ventilation if needed
- Vasopressors (norepinephrine preferred) for hypotension
- ECMO in refractory cases while planning definitive therapy
- Anticoagulation should be started even before diagnosis is confirmed if suspicion is high and bleeding risk is low - this is the single intervention proven to reduce mortality
Step 3: Anticoagulation - The Cornerstone of Treatment
A. Direct Oral Anticoagulants (DOACs) - Now Preferred First Line
Four DOACs are approved for VTE/PE in the US and Europe. Phase III trials showed they are non-inferior in efficacy and safer on major bleeding vs. the traditional parenteral/warfarin regimen. (Fuster and Hurst's The Heart, 15th Ed.)
| Drug | Class | Dosing | Parenteral lead-in needed? |
|---|---|---|---|
| Rivaroxaban | Factor Xa inhibitor | 15 mg BID x 21 days → 20 mg daily | No |
| Apixaban | Factor Xa inhibitor | 10 mg BID x 7 days → 5 mg BID | No |
| Edoxaban | Factor Xa inhibitor | 60 mg daily | Yes (5-10 days LMWH) |
| Dabigatran | Direct thrombin inhibitor | 150 mg BID | Yes (5-10 days LMWH) |
- Rivaroxaban and apixaban allow single-drug therapy - no bridging needed
- DOACs do NOT require INR monitoring and have fewer drug/food interactions than warfarin
- Reversal agents: idarucizumab (dabigatran), andexanet alfa (rivaroxaban, apixaban, edoxaban) - reserved for life-threatening bleeding
B. Parenteral Anticoagulation (Bridge or Primary)
When DOACs can't be used (e.g., massive PE requiring thrombolysis, renal failure, pregnancy):
- Unfractionated heparin (UFH): Weight-based IV infusion, titrated to aPTT. Preferred in high-risk PE and when thrombolysis may be needed (reversible, short half-life).
- Low-molecular-weight heparin (LMWH): e.g., enoxaparin 1 mg/kg SC BID. Preferred for cancer-associated PE (see below).
- Fondaparinux: Once-daily SC, anti-Xa, no HIT risk.
C. Vitamin K Antagonists (Warfarin)
- Still used when DOACs are contraindicated
- Target INR 2.0-3.0
- Must overlap with heparin for ≥5 days (warfarin initially prothrombotic due to protein C/S depletion)
- Initial dose 10 mg for 2 days; 5 mg for elderly/malnourished
Step 4: Advanced/Escalated Therapy
High-Risk (Massive) PE with Hemodynamic Collapse
Systemic Thrombolysis
- Alteplase 100 mg IV over 2 hours is the primary reperfusion therapy for high-risk PE with hemodynamic instability
- Rapidly dissolves thrombus and restores hemodynamics
- Major risk: bleeding, including intracranial hemorrhage (~2%)
- Absolute contraindications: recent stroke, active internal bleeding, recent CNS surgery
- Reduced-dose thrombolysis is being studied (37060258) but not yet standard
Surgical Embolectomy
- Indicated when thrombolysis is contraindicated or fails
- High-volume centers report good outcomes
- Direct surgical extraction from pulmonary arteries under cardiopulmonary bypass
Intermediate-Risk (Submassive) PE
This is the most actively evolving area. Current options include:
Catheter-Directed Thrombolysis (CDT)
- Low-dose tPA infused directly into the clot via catheter
- Lower bleeding risk than systemic thrombolysis
- Standard approach for intermediate PE where intervention is warranted
Large-Bore Mechanical Thrombectomy (LBMT)
-
The PEERLESS RCT (2025, Circulation, n=550, PMID: 39470698) compared LBMT vs CDT in intermediate-risk PE with RV dilation:
- LBMT won on the primary hierarchical composite (win ratio 5.01, p<0.001)
- Fewer episodes of clinical deterioration (1.8% vs 5.4%)
- Markedly less post-procedural ICU use (41.6% vs 98.6% ICU admission)
- Shorter hospital stay (4.5 vs 5.3 nights)
- No difference in mortality, intracranial hemorrhage, or major bleeding
- Better dyspnea scores and RV function at 24 hours
A 2025 meta-analysis (PMID: 40602356) pooling PEERLESS + 6 observational studies confirmed MT results in shorter hospital stays vs CDT, with comparable mortality and readmission rates overall.
Bottom line on catheter therapies: LBMT appears to offer clinical advantages over CDT for intermediate-risk PE, particularly in reducing ICU utilization. However, mortality is equivalent and further RCTs are needed before definitive guideline adoption.
IVC Filter Placement
- Not routinely recommended
- Indications: PE with absolute contraindication to anticoagulation, or recurrent PE despite adequate anticoagulation
- Retrievable filters preferred
Step 5: Treatment by Special Populations
Cancer-Associated PE (CAT)
A 2025 meta-analysis (10 RCTs, n=4713, PMID: 40578592) comparing DOACs vs LMWH in CAT found:
- DOACs reduced recurrent VTE significantly vs LMWH (IRR 0.66, 95% CI 0.56-0.79)
- Total bleeding and all-cause mortality were not significantly different
- DOACs are now considered a viable and potentially preferred option over LMWH in many cancer patients (preferred DOACs: apixaban, rivaroxaban, edoxaban)
- Exception: luminal GI or genitourinary cancers carry higher bleeding risk with DOACs - LMWH still preferred there
Low-Risk PE - Outpatient Management
- HESTIA criteria or sPESI = 0 identifies patients safe for home treatment
- DOAC started in ED, patient discharged with close follow-up
- Reduces hospitalization without increasing adverse events
Pregnancy
- LMWH is the drug of choice (DOACs are teratogenic; warfarin teratogenic in weeks 6-12)
- Dose adjustments needed as pregnancy progresses
- Postpartum: DOACs can be used after delivery
Duration of Anticoagulation
| PE Type | Recommended Duration |
|---|---|
| Provoked PE (surgery, trauma, transient risk) | 3 months |
| Unprovoked first PE | At least 3-6 months; consider indefinite if low bleeding risk |
| Recurrent unprovoked PE | Indefinite anticoagulation |
| Cancer-associated PE | Continue as long as cancer active |
PE Response Teams (PERT)
The 2026 guideline and current practice emphasize multidisciplinary PE response teams (PERT) at high-volume centers. These teams rapidly convene specialists (pulmonology, cardiology, interventional radiology, cardiovascular surgery, hematology) for intermediate-high and high-risk PE to guide escalation decisions in real time.
Long-Term Follow-Up
After discharge all PE patients need:
- Repeat imaging if symptoms persist (to detect CTEPH - chronic thromboembolic pulmonary hypertension, which develops in ~1% of cases)
- Thrombophilia testing (especially for unprovoked or recurrent PE)
- Duration of anticoagulation reassessment
Key Sources:
- 2026 AHA/ACC PE Guideline (Circulation, PMID 41712677) - the most current comprehensive guidance
- PEERLESS RCT 2025 - LBMT vs CDT in intermediate-risk PE (Circulation, PMID 39470698)
- DOACs vs LMWH in cancer-associated PE - meta-analysis 2025 (Am J Cardiol, PMID 40578592)
- MT vs CDT meta-analysis 2025 (Am J Emerg Med, PMID 40602356)
- Fuster and Hurst's The Heart, 15th Edition, Chapter 58
This is a shared conversation. Sign in to Orris to start your own chat.