Antiepileptic drug
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have enough comprehensive information to provide a detailed, well-organized response. Let me compile this into a thorough answer.
Antiepileptic Drugs (AEDs)
Also called antiseizure medications (ASMs)
Goals of Treatment
The primary goal is to render the patient seizure-free with the fewest side effects. About 70% of epilepsy patients achieve complete or near-complete seizure control with medications; another 20-25% have significantly reduced attacks. Approximately 45-50% respond to the first drug, 10-15% to a second agent, and the remainder are considered treatment-resistant (refractory epilepsy). Starting at low doses and spacing administration (once or twice daily) is generally preferred. - Adams and Victor's Principles of Neurology, 12th Ed.
Mechanisms of Action
AEDs act through several principal mechanisms, best illustrated in this diagram:
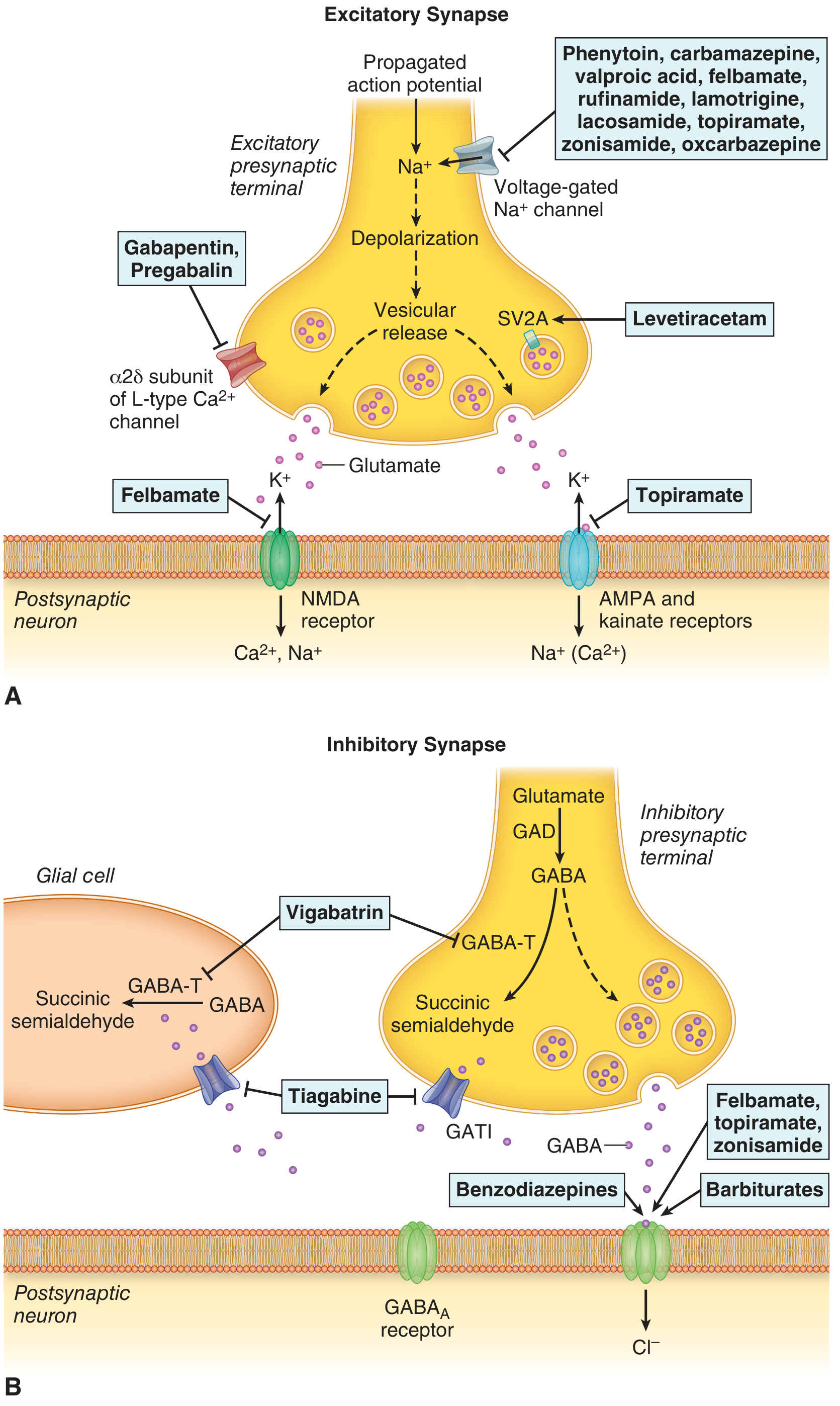
Figure 15-4 from Adams and Victor's Principles of Neurology - AED sites of action
The major mechanisms are:
| Mechanism | Drugs |
|---|---|
| Voltage-gated Na+ channel blockade | Phenytoin, carbamazepine, oxcarbazepine, lamotrigine, lacosamide, valproate, rufinamide, topiramate, zonisamide |
| GABA-A receptor enhancement (Cl- influx) | Benzodiazepines, barbiturates (phenobarbital), topiramate, zonisamide, felbamate |
| GABA reuptake inhibition | Tiagabine |
| GABA transaminase inhibition (raises GABA levels) | Vigabatrin |
| T-type Ca2+ channel blockade | Ethosuximide, valproate |
| Synaptic vesicle protein SV2A binding | Levetiracetam, brivaracetam |
| Alpha-2-delta subunit of Ca2+ channels | Gabapentin, pregabalin |
| AMPA/kainate receptor blockade | Topiramate, felbamate, perampanel |
| NMDA receptor blockade | Felbamate |
- Adams and Victor's Principles of Neurology, 12th Ed., Fig. 15-4; Bradley and Daroff's Neurology
Classification by Generation
First-Generation (Traditional) AEDs
Phenytoin, phenobarbital, primidone, ethosuximide, carbamazepine, valproate
Second-Generation AEDs
Lamotrigine, levetiracetam, topiramate, oxcarbazepine, gabapentin, pregabalin, vigabatrin, tiagabine, felbamate, zonisamide
Third-Generation (Newer) AEDs
Lacosamide, eslicarbazepine, brivaracetam, perampanel, cenobamate, rufinamide, cannabidiol
Pharmacology of Key Individual Drugs
1. Phenytoin (Dilantin)
- Mechanism: Voltage-gated Na+ channel blocker; inhibits abnormal repetitive neuronal firing
- Dose (adult): 300-400 mg/day | Serum level: 10-20 µg/mL | Half-life: 12-36 h
- Use: Focal seizures, generalized tonic-clonic (GTC) seizures; IV form for status epilepticus
- Key side effects: Nystagmus, ataxia, diplopia at toxic levels; gingival hyperplasia, hirsutism, coarsening of facial features (long-term); peripheral neuropathy; non-linear (zero-order) kinetics - small dose increases cause disproportionate level rises above 10 µg/mL
- Serious: Blood dyscrasias, hepatotoxicity, Stevens-Johnson syndrome (rare), teratogenicity (fetal hydantoin syndrome)
- Interactions: Warfarin (unpredictable INR changes), oral contraceptives (failure), CYP enzyme inducer
2. Carbamazepine (Tegretol)
- Mechanism: Na+ channel blocker (similar to phenytoin)
- Dose (adult): 600-1,200 mg/day | Serum level: 4-12 µg/mL | Half-life: 14-25 h
- Use: Focal seizures, GTC; also trigeminal neuralgia, bipolar disorder (mood stabilizer)
- Key side effects: Leukopenia (mild, common), diplopia, dizziness, ataxia; hyponatremia (SIADH); hepatotoxicity; pancytopenia (rare)
- Serious: Stevens-Johnson syndrome - HLA-B*1502 screening required in Asian patients; toxic epidermal necrolysis
- Important: Autoinduction - induces its own metabolism, so doses adequate initially become inadequate after weeks; induces CYP3A4 (reduces OCP, warfarin levels)
3. Valproate / Valproic Acid (Depakote)
- Mechanism: GABAergic (enhances GABA synthesis via glutamic acid decarboxylase), Na+ channel blockade, T-type Ca2+ channel blockade
- Dose (adult): 1,000-3,000 mg/day | Serum level: 50-100 µg/mL | Half-life: 6-15 h (shorter - split dosing)
- Use: Broad spectrum - GTC, absence, myoclonic, focal seizures; drug of choice for juvenile myoclonic epilepsy; mood stabilizer (bipolar); migraine prophylaxis
- Key side effects: Weight gain, tremor, hair loss (reversible), nausea/GI upset, hepatotoxicity (potentially fatal in children < 2 years), pancreatitis
- Serious - Teratogenicity: Major risk of neural tube defects (spina bifida, ~1-2%); cognitive impairment in offspring; contraindicated in pregnancy if alternatives exist; menstrual irregularities, polycystic ovarian syndrome
- Inhibits CYP enzymes - elevates levels of phenytoin, lamotrigine, phenobarbital; avoid in women of childbearing age when possible
4. Phenobarbital (Luminal)
- Mechanism: Enhances GABA-A receptor activity (prolongs Cl- channel opening); also inhibits Na+ currents
- Dose (adult): 90-200 mg/day | Serum level: 15-40 µg/mL | Half-life: 40-120 h (longest - once daily dosing)
- Use: GTC, focal, neonatal seizures; status epilepticus (IV)
- Key side effects: Sedation and cognitive dulling (major limiting factor); nystagmus; behavioral problems in children; Dupuytren contractures, frozen shoulder (chronic use); osteoporosis
- Strong CYP inducer - interacts extensively with warfarin, OCP, other AEDs; teratogenic (~5.5% major malformation rate)
5. Lamotrigine (Lamictal)
- Mechanism: Blocks slow voltage-gated Na+ channels - reduces release of excitatory transmitters (glutamate, aspartate)
- Dose (adult): 300-500 mg/day | Serum level: 2-7 µg/mL | Half-life: 15-60 h
- Use: Broad spectrum - focal, GTC, absence; preferred in women (no weight gain, no ovarian/hormonal issues, better teratogenic profile); mood stabilizer in bipolar
- Key side effects: Rash in ~12% (potentially severe); titrate slowly to minimize; Stevens-Johnson syndrome in ~1%
- Interaction: Valproate doubles lamotrigine levels (requires dose halving); enzyme-inducers reduce lamotrigine levels
- Psychiatric: Antidepressant and mood-stabilizing properties; rarely anxiogenic
6. Levetiracetam (Keppra)
- Mechanism: Binds synaptic vesicle protein SV2A - modulates vesicle release; precise anticonvulsant mechanism still under investigation
- Dose (adult): 500-3,000 mg/day | Half-life: 6-8 h | Renally excreted - dose reduce in renal failure
- Use: Focal and generalized seizures; widely used as first-line due to minimal drug interactions; safe in patients on chemotherapy, anticoagulants, complex polypharmacy
- Key side effects: Somnolence, dizziness; irritability, depression, behavioral changes, suicidality - significant psychiatric concern
- Major advantage: No significant hepatic metabolism, no CYP interactions; favorable in liver disease and complex polypharmacy
7. Ethosuximide (Zarontin)
- Mechanism: Blocks T-type Ca2+ channels in thalamic neurons
- Use: Drug of choice for childhood absence epilepsy (petit mal); NOT effective for other seizure types
- Half-life: Long (~40-60 h) - once daily dosing
- Side effects: GI upset, behavioral disturbance, depression, rarely psychosis
8. Gabapentin (Neurontin) & Pregabalin (Lyrica)
- Mechanism: Bind alpha-2-delta subunit of voltage-gated Ca2+ channels - reduce calcium-mediated neurotransmitter release; structurally GABA analogs but do NOT act on GABA receptors
- Use: Adjunctive therapy for focal seizures; also neuropathic pain, fibromyalgia, anxiety (pregabalin)
- Advantages: Not metabolized hepatically; few drug interactions; renally excreted (adjust in renal failure)
- Side effects: Sedation, weight gain, peripheral edema, dizziness; withdrawal anxiety/depression on cessation
9. Topiramate (Topamax)
- Mechanism: Multiple - Na+ channel blockade, GABA-A enhancement, AMPA/kainate receptor blockade, carbonic anhydrase inhibition
- Use: Focal and generalized seizures; migraine prophylaxis; weight loss (Qsymia)
- Side effects: Cognitive slowing ("dopamax"), word-finding difficulties, kidney stones (carbonic anhydrase inhibition), weight loss, metabolic acidosis
- Psychiatric: Anxiety, depression, psychosis (rare)
10. Oxcarbazepine (Trileptal)
- Mechanism: Na+ channel blockade (carbamazepine analogue - acts via active metabolite monohydroxy derivative, MHD)
- Use: Focal seizures; better tolerated than carbamazepine
- Advantages over carbamazepine: Less marrow toxicity, no autoinduction, fewer drug interactions
- Side effects: Hyponatremia (more common than carbamazepine, ~3%); rash; dizziness
Drug of Choice by Seizure Type
| Seizure/Epilepsy Type | First-line Drug(s) |
|---|---|
| Focal (partial) seizures | Carbamazepine, lamotrigine, levetiracetam, oxcarbazepine |
| Generalized tonic-clonic | Valproate, lamotrigine, levetiracetam, phenytoin |
| Absence (childhood) | Ethosuximide (first choice), valproate |
| Juvenile myoclonic epilepsy | Valproate, levetiracetam, lamotrigine |
| Myoclonic seizures | Valproate, levetiracetam, clonazepam |
| Status epilepticus | IV lorazepam/diazepam (1st) → IV fosphenytoin/valproate (2nd) → phenobarbital/propofol (3rd) |
| Neonatal seizures | Phenobarbital (IV) |
| Infantile spasms (West) | ACTH, vigabatrin, prednisolone |
| Lennox-Gastaut | Valproate, rufinamide, cannabidiol, clobazam |
| Dravet syndrome | Stiripentol, cannabidiol, valproate |
- Goldman-Cecil Medicine; Adams and Victor's Neurology
Pharmacokinetics Summary
| Drug | Adult Dose (mg/d) | Therapeutic Level (µg/mL) | Half-life (h) | Dosing |
|---|---|---|---|---|
| Valproate | 1,000-3,000 | 50-100 | 6-15 | 2-3x daily |
| Phenytoin | 300-400 | 10-20 | 12-36 | Once daily |
| Carbamazepine | 600-1,200 | 4-12 | 14-25 | 2-3x daily |
| Oxcarbazepine | 900-2,400 | - | 1-5 (MHD: 9-11) | 2x daily |
| Phenobarbital | 90-200 | 15-40 | 40-120 | Once daily |
| Lamotrigine | 300-500 | 2-7 | 15-60 | 2x daily |
| Levetiracetam | 500-3,000 | - | 6-8 | 2x daily |
| Topiramate | 200-400 | - | 20-24 | 2x daily |
| Ethosuximide | 500-1,500 | 40-100 | 40-60 | Once daily |
| Gabapentin | 900-3,600 | - | 5-7 | 3x daily |
- Adams and Victor's Principles of Neurology, Table 15-6
Drug Interactions (Key Points)
Enzyme Inducers (reduce levels of other drugs - OCP, warfarin, other AEDs):
- Phenytoin, carbamazepine, phenobarbital, primidone, rufinamide
Enzyme Inhibitors (raise levels of co-drugs):
- Valproate - inhibits CYP2C9, displaces protein-bound drugs; raises phenytoin, lamotrigine, phenobarbital levels
Renally Excreted (safer in liver disease, fewer interactions):
- Levetiracetam, gabapentin, pregabalin - dose reduce in renal failure
Clinically Critical Interactions:
-
Valproate + lamotrigine: doubles lamotrigine levels → rash risk; halve lamotrigine dose
-
Valproate + carbamazepine: carbamazepine epoxide builds up via epoxide hydrolase inhibition → toxicity
-
Phenytoin/carbamazepine + oral contraceptives: OCP failure - adjust estradiol dose
-
Fluoxetine/fluvoxamine + phenytoin or carbamazepine: raises AED levels (CYP inhibition)
-
Adams and Victor's, p. 361; Maudsley Prescribing Guidelines, 15th Ed.
Special Populations
Pregnancy
- All AEDs are potentially teratogenic - folic acid supplementation and vitamin K before delivery are essential
- Valproate carries the highest teratogenic risk (neural tube defects, reduced IQ in offspring) - avoid if possible; switch to levetiracetam for juvenile myoclonic epilepsy before conception
- Lamotrigine has a more favorable teratogenic profile than most others
- Enzyme-inducing AEDs accelerate vitamin K metabolism - give to mother and newborn to prevent neonatal hemorrhage
Women of Childbearing Age
- Avoid valproate when alternatives exist
- Enzyme inducers reduce OCP efficacy
- Lamotrigine or levetiracetam are preferred first-line choices
Elderly
- Prefer drugs with fewer interactions: gabapentin, levetiracetam, brivaracetam, lacosamide
- Avoid enzyme inducers (carbamazepine, phenytoin, phenobarbital) due to complex polypharmacy
Renal Failure
- Reduce dose of renally excreted AEDs: levetiracetam, gabapentin, pregabalin
Liver Failure
- Monitor levels more closely; prefer renally excreted drugs
Psychiatric Side Effects
| Drug | Adverse Effects | Psychiatric Benefits |
|---|---|---|
| Barbiturates | Behavioral disturbance, depression, cognitive impairment | Anxiolytic, hypnotic |
| Carbamazepine/Oxcarbazepine | Insomnia | Mood stabilizing, anti-manic |
| Lamotrigine | Anxiogenic in some | Antidepressant, mood stabilizing |
| Levetiracetam | Anxiety, behavioral disturbance, depression, suicidality | None confirmed |
| Valproate | Behavioral disturbance at high doses (children) | Mood stabilizing, anti-manic, anti-panic |
| Topiramate | Anxiety, depression, psychosis | Possible anti-manic |
| Phenytoin | Behavioral disturbance, depression | Anti-manic |
| Vigabatrin | Behavioral disturbance, depression, psychosis | None |
- Maudsley Prescribing Guidelines, 15th Ed., Table 10.4
Skin Reactions (Rashes)
- Aromatic AEDs (phenytoin, carbamazepine, phenobarbital, primidone, lamotrigine) have the highest rash risk with significant cross-reactivity
- Typical rash: maculopapular, trunk-predominant, within the first month
- Severe reactions: Stevens-Johnson syndrome, toxic epidermal necrolysis - most common with lamotrigine (especially if escalated too fast) and carbamazepine
- HLA-B*1502: Screen Asian patients before starting carbamazepine (risk of SJS/TEN)
- HLA-A*3101: Associated with skin eruptions in Caucasians on carbamazepine
- If replacing an aromatic drug: use valproate, gabapentin, topiramate, or levetiracetam as substitutes
Discontinuation of AEDs
- Consider after 2 years of seizure freedom; taper slowly
- ~40% relapse risk at 2.5 years, ~50% at 5 years after stopping (vs ~20% on continued therapy)
- Obtain EEG before withdrawal - paroxysmal activity favors continuing treatment
- Juvenile myoclonic epilepsy: Lifelong therapy usually recommended
- Relapse risk is higher in focal seizures vs. absence/generalized-onset
Bone Health
Most AEDs (especially enzyme inducers) reduce bone density through CYP450-mediated vitamin D degradation. Consider calcium, vitamin D supplementation, and periodic bone density monitoring - particularly in women on long-term therapy. - Adams and Victor's, p. 362
References:
- Adams and Victor's Principles of Neurology, 12th Ed., Ch. 15 (Antiepileptic Drugs - General Principles, Specific Drugs, Tables 15-5 & 15-6)
- Goldman-Cecil Medicine International Edition, Ch. 372 (Table 372-7)
- Maudsley Prescribing Guidelines in Psychiatry, 15th Ed., Table 10.4
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
This is a shared conversation. Sign in to Orris to start your own chat.