Cbc complete pathology, physiology, anatomy and pharmacology and disease and complications
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have rich content from Harrison's and Rosen's Emergency Medicine. Let me compile the comprehensive CBC guide.
Complete Blood Count (CBC) - Complete Guide
What is a CBC?
A CBC (Complete Blood Count) is a panel of laboratory tests that measures the cellular components of blood. It is performed using automated electronic cell counters that directly measure red cell size (MCV), number of red cells, and hemoglobin levels, with additional values derived from these measurements. It is the most commonly ordered hematologic test worldwide.
- Harrison's Principles of Internal Medicine 22E, p. 488
ANATOMY OF BLOOD - The Components Measured
Blood is a specialized connective tissue consisting of cellular elements suspended in plasma. The CBC evaluates three major cell lines, all derived from pluripotent hematopoietic stem cells in the bone marrow:
| Cell Line | Origin | Normal Lifespan |
|---|---|---|
| Red Blood Cells (Erythrocytes) | Bone marrow (erythroid lineage) | ~120 days |
| White Blood Cells (Leukocytes) | Bone marrow (myeloid/lymphoid lineage) | Hours to years |
| Platelets (Thrombocytes) | Bone marrow megakaryocytes | 7-10 days |
Bone marrow anatomy: Normal marrow has ~40-50% nucleated cellular elements and ~50-60% fat. The ratio changes in disease (erythroid hyperplasia in hemolytic anemia, myeloid hyperplasia in infection/leukemia).
PART 1: RED BLOOD CELLS (RBCs) / ERYTHROCYTES
Physiology
- Biconcave disc, ~7-8 µm diameter, no nucleus, no mitochondria
- Primary function: oxygen transport via hemoglobin (Hb)
- Hemoglobin = 4 globin chains + 4 heme groups; each heme binds 1 O₂
- Adult hemoglobin (HbA) = 2 alpha + 2 beta chains (α₂β₂)
- RBCs use anaerobic glycolysis (Embden-Meyerhof pathway) for energy
- 2,3-DPG regulates oxygen affinity: higher 2,3-DPG = lower O₂ affinity = better tissue O₂ delivery
Compensatory mechanisms in anemia:
- Increased heart rate and cardiac output (immediate)
- Increased 2,3-DPG (hours to days)
- Increased plasma volume (weeks)
Normal CBC Values - RBC Parameters
| Parameter | Formula | Normal Values |
|---|---|---|
| Hemoglobin (Hgb) | Direct measurement | Men: 13.5-17.5 g/dL; Women: 12.0-16.0 g/dL |
| Hematocrit (Hct) | RBC count × MCV ÷ 10 | Men: 41-53%; Women: 36-46% |
| RBC Count | Direct count | Men: 4.5-5.9 × 10⁶/µL; Women: 4.0-5.2 × 10⁶/µL |
| MCV | Hct ÷ RBC count × 10 | 85-95 fL |
| MCH | Hgb ÷ RBC count × 10 | 28.5-32.3 pg |
| MCHC | Hgb ÷ Hct × 100 | 33.8-34.2 g/dL |
| RDW | SD of MCV/Mean MCV × 100 | 11.5-14.5% |
- Harrison's 22E (Table 66-1), p. 488; Rosen's Emergency Medicine (Table 109.2)
Note: MCHC changes very little in most anemias and is of limited value. MCH varies linearly with MCV and also adds limited independent value. MCV is the most clinically useful index.
PART 2: THE PERIPHERAL BLOOD SMEAR
The blood smear allows direct visualization of blood cells and complements the CBC indices:
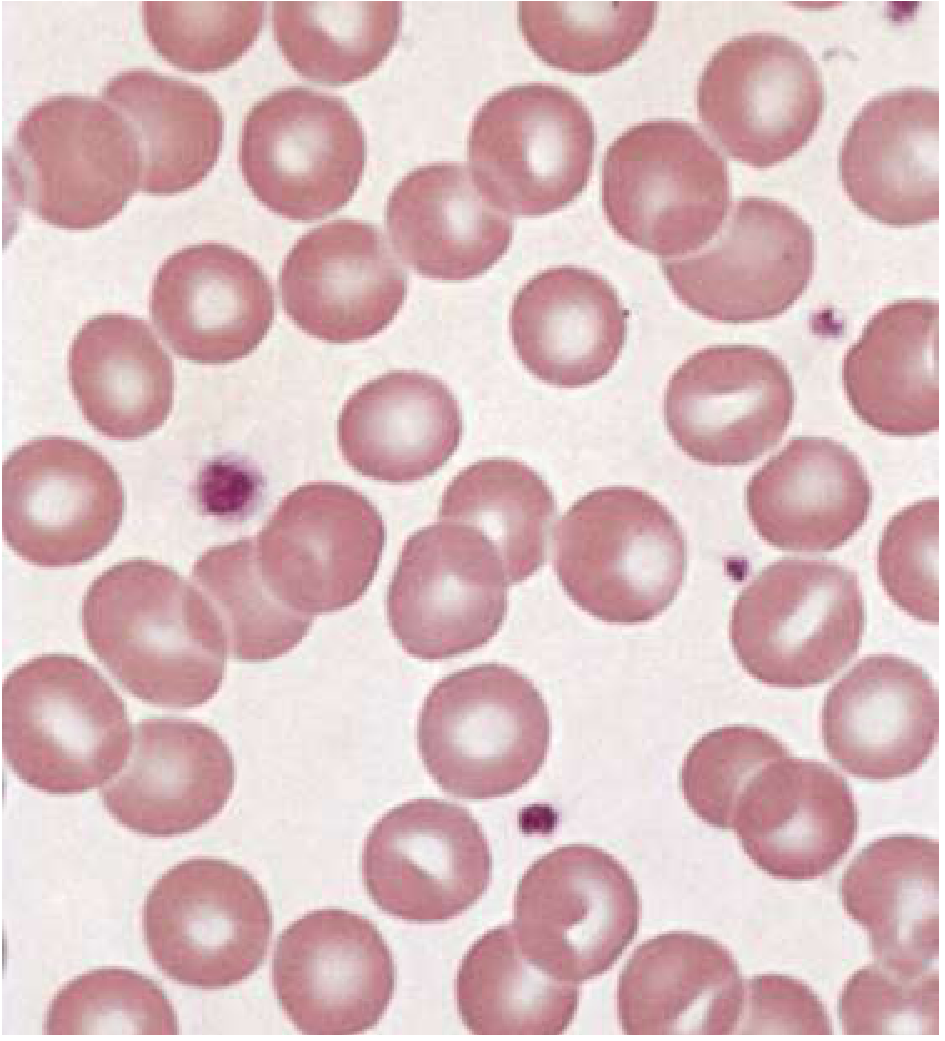
Key smear findings:
| Finding | Description | Significance |
|---|---|---|
| Anisocytosis | Variation in cell size | Correlates with elevated RDW |
| Poikilocytosis | Variation in cell shape | Defective maturation or fragmentation |
| Polychromasia | Large, grayish-blue cells | Premature reticulocytes (EPO stimulation) |
| Hypochromia | Enlarged area of central pallor | Iron deficiency, thalassemia |
| Teardrop cells (dacrocytes) | Teardrop shape | Marrow disruption, severe iron deficiency |
| Schistocytes | Fragmented cells | Microangiopathic hemolytic anemia (TTP, HUS, DIC) |
| Sickle cells | Crescent shape | Sickle cell disease |
| Target cells | Bull's-eye appearance | Thalassemia, liver disease, HbC |
| Spherocytes | Small, round, no central pallor | Hereditary spherocytosis, autoimmune hemolytic anemia |
PART 3: RETICULOCYTE COUNT
- Reticulocytes contain mRNA for ~24h after marrow release; detected by new methylene blue stain
- Measure of red cell production
- Separates hyperproliferative (hemolysis/blood loss) from hypoproliferative (production defect) anemia
Corrected reticulocyte count = Measured retic count × (Patient Hct / 45%)
Absolute reticulocyte count = (Reticulocyte % / 100) × RBC count
-
Normal absolute count: 25,000-75,000 cells/µL
-
No hematocrit correction needed for absolute count
-
Harrison's 22E, p. 490-491
PART 4: WHITE BLOOD CELLS (WBCs) / LEUKOCYTES
Normal WBC Parameters
| Parameter | Normal Range |
|---|---|
| Total WBC count | 4,500-11,000 /µL |
| Neutrophils | 50-70% (absolute: 1,800-7,700/µL) |
| Lymphocytes | 20-40% (absolute: 1,000-4,800/µL) |
| Monocytes | 2-8% (absolute: 200-900/µL) |
| Eosinophils | 1-4% (absolute: 100-400/µL) |
| Basophils | 0.5-1% (absolute: 0-200/µL) |
WBC Differential - Functions
| Cell | Key Function |
|---|---|
| Neutrophils | First responders to bacterial/fungal infection; phagocytosis |
| Lymphocytes | Adaptive immunity - B cells (antibodies), T cells (cell-mediated) |
| Monocytes | Phagocytosis; become macrophages in tissues |
| Eosinophils | Parasitic infections; allergic/hypersensitivity reactions |
| Basophils | Allergic responses; IgE receptors; release histamine |
Pathological WBC Changes
| Abnormality | Definition | Causes |
|---|---|---|
| Leukocytosis | WBC > 11,000/µL | Infection, inflammation, steroids, leukemia |
| Leukopenia | WBC < 4,500/µL | Viral infections, aplastic anemia, chemotherapy, HIV |
| Neutrophilia | Neutrophils > 7,700/µL | Bacterial infection, stress, steroids, MI |
| Neutropenia | ANC < 1,500/µL | Chemotherapy, aplasia, B12/folate deficiency |
| Lymphocytosis | Lymphocytes > 4,800/µL | Viral infections (EBV, CMV), CLL, pertussis |
| Lymphopenia | Lymphocytes < 1,000/µL | HIV/AIDS, immunosuppression, SLE |
| Eosinophilia | Eosinophils > 400/µL | Parasites, asthma, allergies, Hodgkin lymphoma |
| Basophilia | Basophils > 200/µL | CML, allergic states, hypothyroidism |
| Monocytosis | Monocytes > 900/µL | TB, subacute bacterial endocarditis, inflammatory disorders |
| Left shift | Bands/immature neutrophils in blood | Severe bacterial infection, sepsis |
Note: Neonates and children have a lower total WBC and neutrophil count with a higher percentage of lymphocytes compared to adults.
PART 5: PLATELETS
Normal Values and Physiology
- Normal platelet count: 150,000-400,000 /µL
- Produced by megakaryocytes in the bone marrow
- Lifespan: 7-10 days; destroyed in spleen
- Function: primary hemostasis (platelet plug formation)
- Adhesion via GPIb-von Willebrand factor
- Activation (shape change, granule release)
- Aggregation via GPIIb/IIIa-fibrinogen
Pathological Platelet Changes
| Abnormality | Definition | Causes |
|---|---|---|
| Thrombocytopenia | Platelets < 150,000/µL | ITP, TTP, HUS, DIC, heparin-induced (HIT), hypersplenism, aplasia |
| Thrombocytosis | Platelets > 400,000/µL | Reactive (infection, iron deficiency, post-splenectomy) or primary (ET, CML) |
Bleeding risk by platelet count:
- < 100,000: surgical bleeding risk
- < 50,000: spontaneous bleeding risk
- < 10,000-20,000: risk of spontaneous intracranial hemorrhage
PART 6: CLASSIFICATION OF ANEMIA (CBC-Based)
The MCV is the cornerstone of CBC-based anemia classification:
A. Microcytic Anemia (MCV < 80 fL)
| Cause | Additional CBC Clues | Key Test |
|---|---|---|
| Iron deficiency anemia | Low MCH, high RDW, thrombocytosis | Serum ferritin (low), TIBC (high) |
| Thalassemia | Low MCV but high/normal RBC count, low RDW | Hb electrophoresis |
| Anemia of chronic disease | Normal/low RDW | Serum ferritin (normal/high) |
| Lead poisoning | Basophilic stippling on smear | Blood lead level |
| Sideroblastic anemia | Ring sideroblasts on bone marrow | Bone marrow biopsy |
Thalassemia pathophysiology: Autosomal recessive disorder with decreased globin chain synthesis. Beta-thalassemia has reduced/absent beta-globin -> excess alpha-chains -> reactive oxygen species -> erythroid apoptosis -> hemolytic anemia. Alpha-thalassemia has excess beta-chains forming HbH.
B. Normocytic Anemia (MCV 80-100 fL)
| Cause | Key Features |
|---|---|
| Anemia of chronic disease | Most common; normocytic or microcytic |
| Aplastic anemia | Pancytopenia (low RBC + WBC + platelets) |
| Acute blood loss | Low Hgb, normal MCV initially |
| Hemolytic anemia | Elevated reticulocyte count, elevated LDH, low haptoglobin |
| Renal failure | Low EPO, decreased production |
| Hypothyroidism | May be normocytic or macrocytic |
C. Macrocytic Anemia (MCV > 100 fL)
| Cause | Smear Finding | Key Test |
|---|---|---|
| B12 deficiency | Hypersegmented neutrophils, oval macrocytes | Low serum B12, elevated methylmalonic acid |
| Folate deficiency | Hypersegmented neutrophils, oval macrocytes | Low serum folate |
| Liver disease | Target cells, acanthocytes | LFTs |
| Alcohol | Macrocytes without hypersegmentation | History |
| Myelodysplastic syndrome | Dysplastic cells | Bone marrow biopsy |
| Hydroxyurea/Methotrexate | Drug-induced | Medication history |
PART 7: WBC DISEASE STATES
Leukemia (Malignant WBC Proliferation)
| Type | CBC Features |
|---|---|
| AML (Acute Myeloid) | High WBC with blasts (>20%), Auer rods on smear |
| ALL (Acute Lymphoblastic) | High WBC with lymphoblasts; most common childhood leukemia |
| CML (Chronic Myeloid) | Very high WBC (50,000-200,000), left shift, basophilia, thrombocytosis |
| CLL (Chronic Lymphocytic) | High WBC with mature lymphocytes (>5,000); smudge cells on smear |
Reactive WBC Changes
- Infectious mononucleosis (EBV): Lymphocytosis with atypical lymphocytes
- Sepsis: Leukocytosis with left shift (bands/metamyelocytes); may have leukemoid reaction (WBC > 50,000)
- Viral infections: Leukopenia with relative lymphocytosis
- Allergic reactions/parasites: Eosinophilia
PART 8: PLATELET DISEASE STATES
Thrombocytopenia
ITP (Immune Thrombocytopenic Purpura):
- Autoimmune destruction via anti-platelet IgG antibodies
- Isolated thrombocytopenia; normal WBC, Hgb
- Treatment: steroids, IVIG, anti-D, thrombopoietin receptor agonists, splenectomy
TTP (Thrombotic Thrombocytopenic Purpura):
- ADAMTS13 deficiency -> uncleaved vWF multimers -> platelet microthrombi
- Pentad: thrombocytopenia, MAHA, fever, renal failure, neurological symptoms
- Treatment: plasma exchange (PEX)
HIT (Heparin-Induced Thrombocytopenia):
- Platelet drop >50% after heparin exposure (days 5-10)
- Paradoxically prothrombotic (not bleeding)
- Stop heparin immediately; use alternative anticoagulant (argatroban, bivalirudin)
PART 9: PHARMACOLOGY - DRUGS AFFECTING THE CBC
Drugs That Cause Anemia
| Drug | Mechanism | CBC Pattern |
|---|---|---|
| Methotrexate, hydroxyurea, 5-FU | Folate antagonism/DNA synthesis inhibition | Macrocytic anemia |
| Chloramphenicol | Bone marrow suppression | Aplastic anemia, pancytopenia |
| NSAIDs | GI blood loss | Microcytic (iron deficiency) |
| Dapsone, primaquine | Oxidative hemolysis in G6PD deficiency | Hemolytic anemia |
| Methyldopa, penicillin | Drug-induced autoimmune hemolysis | AIHA - normocytic |
| Ribavirin | Direct hemolysis | Hemolytic anemia |
Drugs That Cause Thrombocytopenia
| Drug | Mechanism |
|---|---|
| Heparin | HIT (immune-mediated platelet activation) |
| Quinine/quinidine | Drug-dependent antibodies |
| Chemotherapy agents | Bone marrow suppression |
| Valproic acid | Dose-dependent thrombocytopenia |
| Linezolid | Myelosuppression |
| TMP-SMX | Immune-mediated |
Drugs That Cause Leukopenia/Agranulocytosis
| Drug | Notes |
|---|---|
| Clozapine | Requires mandatory WBC monitoring weekly for 6 months |
| Methimazole/carbimazole | Monitor in hyperthyroid patients |
| Carbamazepine, phenytoin | Rare but serious |
| Chemotherapy (any) | Expected dose-dependent |
| Colchicine (overdose) | Bone marrow suppression |
Drugs That Treat CBC Abnormalities
| Drug | Use | Mechanism |
|---|---|---|
| Erythropoietin (EPO, darbepoetin) | Anemia of CKD | Stimulates erythropoiesis |
| Ferrous sulfate 325mg TID | Iron deficiency anemia | Iron replacement |
| B12 (cyanocobalamin) | B12 deficiency anemia | Cofactor for DNA synthesis |
| Folic acid 1-5mg/day | Folate deficiency | DNA synthesis |
| G-CSF (filgrastim) | Chemotherapy-induced neutropenia | Stimulates neutrophil production |
| Eltrombopag, romiplostim | ITP, low platelets | Thrombopoietin receptor agonists |
| IVIG | ITP | Blocks Fc receptor-mediated platelet destruction |
| Prednisone | ITP, AIHA | Immunosuppression |
| Hydroxyurea | Sickle cell disease | Increases HbF production |
PART 10: COMPLICATIONS OF CBC ABNORMALITIES
Complications of Anemia
| Severity | Complication |
|---|---|
| Mild (Hgb 10-12) | Fatigue, dyspnea on exertion, tachycardia |
| Moderate (Hgb 8-10) | High-output cardiac failure, pallor, impaired cognition |
| Severe (Hgb < 8) | Cardiac failure, myocardial ischemia, shock |
| Chronic severe | Tissue hypoxia, organ dysfunction, impaired wound healing |
| Pregnancy | Preterm birth, low birth weight, maternal mortality |
Compensatory failure: When plasma volume expansion overwhelms cardiac capacity, edema and heart failure develop.
Complications of Leukopenia/Neutropenia
| ANC Level | Risk |
|---|---|
| ANC < 1,000/µL | Increased infection risk |
| ANC < 500/µL | Severe risk (fever = oncologic emergency) |
| ANC < 100/µL | Life-threatening infections (pseudomonas, fungal, gram-negative sepsis) |
Febrile neutropenia: Temperature > 38.3°C with ANC < 500 -> empirical broad-spectrum antibiotics (piperacillin-tazobactam or cefepime) immediately.
Complications of Thrombocytopenia
- Platelet 50,000-100,000: Post-surgical/traumatic bleeding
- Platelet 10,000-50,000: Spontaneous mucosal bleeding (petechiae, purpura, epistaxis, GI bleeding)
- Platelet < 10,000: Spontaneous intracranial hemorrhage risk
Complications of Thrombocytosis
- Platelet > 1,000,000 (extreme): Paradoxical bleeding (acquired vWF deficiency)
- Primary thrombocytosis (ET, CML): Arterial/venous thrombosis, stroke, MI, Budd-Chiari syndrome
SUMMARY TABLE - CBC Normal Reference Ranges
| Parameter | Normal Range |
|---|---|
| Hemoglobin (Men) | 13.5-17.5 g/dL |
| Hemoglobin (Women) | 12.0-16.0 g/dL |
| Hematocrit (Men) | 41-53% |
| Hematocrit (Women) | 36-46% |
| RBC (Men) | 4.5-5.9 × 10⁶/µL |
| RBC (Women) | 4.0-5.2 × 10⁶/µL |
| MCV | 85-95 fL |
| MCH | 28.5-32.3 pg |
| MCHC | 33.8-34.2 g/dL |
| RDW | 11.5-14.5% |
| WBC | 4,500-11,000/µL |
| Neutrophils | 50-70% (ANC 1,800-7,700) |
| Lymphocytes | 20-40% (1,000-4,800/µL) |
| Monocytes | 2-8% |
| Eosinophils | 1-4% |
| Basophils | 0.5-1% |
| Platelets | 150,000-400,000/µL |
| Reticulocytes | 0.5-1.5% (absolute: 25,000-75,000/µL) |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 66 - Anemia, pp. 488-491
- Rosen's Emergency Medicine - Chapter 109, Anemia
- Washington Manual of Medical Therapeutics - Hematology
This is a shared conversation. Sign in to Orris to start your own chat.