Let’s study everything in detail in crisp, concise and conceptual way fromCOPD guidelines or gold that is required in MBBS level Especially from diagnosis and management
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Now I have everything I need. Let me compile the comprehensive, crisp MBBS-level COPD guide.
COPD — Complete MBBS-Level Study Guide (GOLD Framework)
Sources: Goldman-Cecil Medicine, Washington Manual of Medical Therapeutics, Textbook of Family Medicine
1. DEFINITION (Conceptual Core)
COPD = persistent airflow limitation that is NOT fully reversible with bronchodilators, caused by airway/alveolar abnormalities from noxious exposures.
It encompasses two entities that coexist in most patients:
| Entity | Core Defect | Classic Type |
|---|---|---|
| Chronic Bronchitis | Mucus hypersecretion, inflammation | "Blue Bloater" |
| Emphysema | Alveolar wall destruction, loss of elastic recoil | "Pink Puffer" |
Chronic bronchitis definition (clinical): Productive cough ≥3 months/year for ≥2 consecutive years.
2. RISK FACTORS
- Cigarette smoking — far and away the #1 risk factor (dose = pack-years)
- Biomass fuel combustion (cooking/heating in poorly ventilated spaces)
- Occupational dust (mines, grain, cotton mills)
- α₁-antitrypsin (A1AT) deficiency — genetic cause; screen ALL COPD patients at least once
- Childhood respiratory infections → impaired lung growth → lower peak FEV₁
- Secondhand smoke, maternal smoking during pregnancy
3. PATHOPHYSIOLOGY (Conceptual)
Trigger: Noxious inhalation → chronic inflammation
Key imbalance: Protease > Antiprotease → alveolar destruction (emphysema)
- Normal: Neutrophil elastase balanced by A1AT
- In COPD/smoking: A1AT overwhelmed → unchecked elastase → alveolar wall breakdown
Consequences:
- Loss of elastic recoil → dynamic collapse of small airways during expiration → air trapping
- Mucus gland hypertrophy + goblet cell hyperplasia → chronic bronchitis physiology
- V/Q mismatch → hypoxemia
- Late: hypercapnia, cor pulmonale, polycythemia
4. CLINICAL FEATURES
Typical patient: >40 years, significant smoking history
Symptoms (progressive over years):
- Dyspnea on exertion (cardinal symptom)
- Chronic cough + sputum production
- Wheezing
Classic phenotypes:
| Feature | Pink Puffer (Emphysema) | Blue Bloater (Chronic Bronchitis) |
|---|---|---|
| Build | Thin, cachexic | Obese/overweight |
| Cyanosis | Absent | Present |
| Cough | Minimal | Productive, chronic |
| PaCO₂ | Normal/low | High (CO₂ retention) |
| PaO₂ | Near normal | Low |
| Cor pulmonale | Late | Early |
| Breathing | Pursed-lip, tripod | Labored |
Signs:
- Barrel chest (↑AP diameter), hyperresonance
- Diminished breath sounds, prolonged expiration
- Use of accessory muscles
- Pursed-lip breathing
5. DIAGNOSIS
Step 1: Clinical suspicion
Any patient >40 years with dyspnea, chronic cough/sputum, or risk factor exposure.
Step 2: Spirometry — THE GOLD STANDARD
Diagnostic criterion (post-bronchodilator):
FEV₁/FVC < 0.70
This confirms fixed (irreversible) airflow obstruction.
Additional findings:
- ↑ TLC, FRC, RV (hyperinflation, air trapping)
- ↓ DLCO in emphysema (alveolar destruction)
Step 3: GOLD Spirometric Severity Grading
(Based on post-bronchodilator FEV₁ % predicted, in patients with FEV₁/FVC < 0.70)
| GOLD Grade | Severity | FEV₁ % Predicted |
|---|---|---|
| 1 | Mild | ≥80% |
| 2 | Moderate | 50–79% |
| 3 | Severe | 30–49% |
| 4 | Very Severe | <30% |
Step 4: GOLD ABCD Classification (combines symptoms + exacerbation risk)
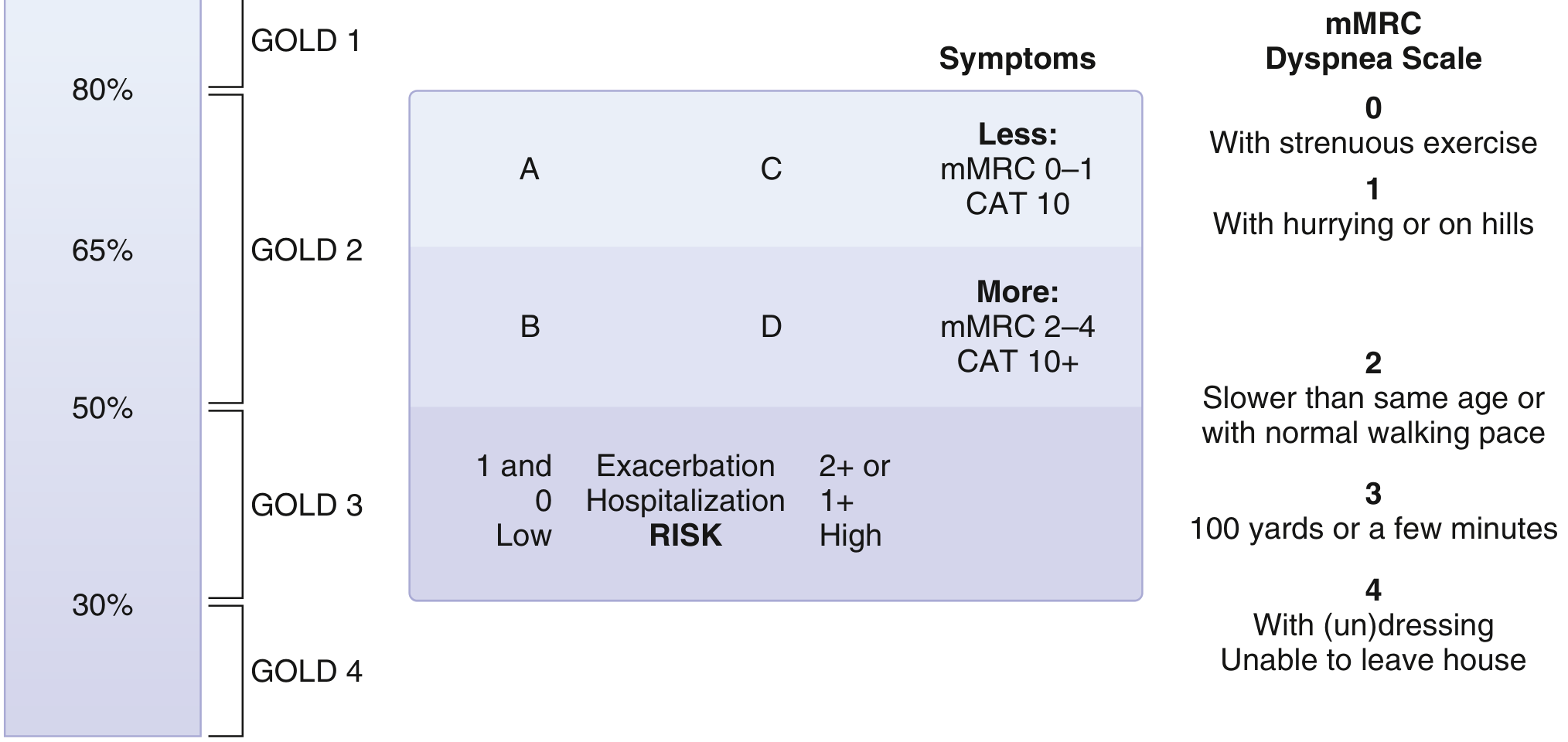
| Group | Exacerbations | Symptoms | Spirometry |
|---|---|---|---|
| A | 0–1 (no hospitalization) | Mild (mMRC 0–1 or CAT <10) | Any |
| B | 0–1 (no hospitalization) | More (mMRC ≥2 or CAT ≥10) | Any |
| C | ≥2 or ≥1 hospitalization | Mild (mMRC 0–1 or CAT <10) | Any |
| D | ≥2 or ≥1 hospitalization | More (mMRC ≥2 or CAT ≥10) | Any |
Key concept: ABCD groups guide therapy; GOLD 1–4 grades guide prognosis.
Symptom tools:
- mMRC Scale (0–4): 0 = only with strenuous exertion → 4 = too breathless to leave house
- CAT Score (0–40): ≥10 = significant impact
Investigations
| Test | Purpose |
|---|---|
| Spirometry | Diagnosis (essential) |
| CXR | Exclude alternatives; shows hyperinflation, flat diaphragm, bullae, ↓vascular markings |
| CT chest | Detects emphysema, airway thickening, air trapping; guides surgery candidacy |
| ABG | Severe COPD — assess hypoxemia/hypercapnia |
| A1AT level | Screen all COPD patients once |
| Peripheral eosinophils | >300 cells/μL → consider ICS |
| 6-min walk test | Functional capacity, prognosis |
| ECG/Echo | Detect cor pulmonale |
6. STABLE COPD MANAGEMENT
Principle: Goals of treatment
- Reduce symptoms and improve exercise tolerance
- Reduce frequency/severity of exacerbations
- Slow disease progression
- Prolong survival
A. Smoking Cessation — #1 MOST IMPORTANT INTERVENTION
- Only intervention proven to slow FEV₁ decline
- NRT (nicotine patch/gum), Varenicline, Bupropion
- Counseling + pharmacotherapy = best combo
B. Pharmacotherapy — Inhaled Route is Preferred
Classes of drugs:
| Class | Examples | Mechanism | Key Side Effects |
|---|---|---|---|
| SABA | Salbutamol/Albuterol, Levalbuterol | β₂-agonist, bronchodilation | Palpitations, tremor, tachycardia |
| SAMA | Ipratropium | Muscarinic antagonist | Dry mouth, urinary retention |
| LABA | Salmeterol, Formoterol, Indacaterol, Olodaterol | Long-acting β₂-agonist | Palpitations, hypokalemia |
| LAMA | Tiotropium, Umeclidinium, Glycopyrronium | Long-acting muscarinic antagonist | Dry mouth, constipation, glaucoma |
| ICS | Fluticasone, Budesonide, Beclomethasone | Anti-inflammatory | Oral candidiasis, hoarseness, ↑ pneumonia risk |
| PDE-4 inhibitor | Roflumilast | Anti-inflammatory | Diarrhoea, nausea, weight loss, depression |
| Theophylline | Oral | Nonspecific PDE inhibitor, bronchodilator | Narrow therapeutic index; arrhythmias, seizures |
Key rules for ICS:
- Never monotherapy in COPD
- Indicated if eosinophils >300 cells/μL, or persistent exacerbations on LABA+LAMA
- Withdraw if <2 exacerbations/year AND eosinophils <300 cells/μL
C. Initial Pharmacotherapy by ABCD Group
| Group | First Choice |
|---|---|
| A | A bronchodilator (SABA or SAMA as needed) |
| B | LABA or LAMA |
| C | LAMA (preferred over LABA) |
| D | LAMA ± LABA; if CAT >20 → LABA+LAMA; if eosinophils >300 → ICS+LABA |
Escalation concept: A → B = add long-acting agent; C/D = LABA+LAMA → add ICS if still exacerbating and eos >300.
D. Non-Pharmacological Therapy
| Intervention | Notes |
|---|---|
| Pulmonary rehabilitation | All patients (especially post-exacerbation, pre-surgery). Aerobic + strength training. Improves exercise tolerance and quality of life. |
| Long-term oxygen therapy (LTOT) | Improves survival — only non-pharmacological intervention proven to do so |
| Vaccinations | Influenza (annual), Pneumococcal, COVID-19 |
| NIV (BiPAP) | Nocturnal hypercapnia with PaCO₂ ≥52 mmHg |
| LVRS | Lung volume reduction surgery for upper-lobe emphysema + low exercise capacity |
| Lung transplant | End-stage COPD |
LTOT Indications (memorize)
- PaO₂ ≤55 mmHg or SpO₂ ≤88% at rest
- PaO₂ 56–59 mmHg or SpO₂ <89% if cor pulmonale, right heart failure, or polycythemia (Hct >55%)
7. ACUTE EXACERBATION OF COPD (AECOPD)
Definition
Acute worsening of respiratory symptoms beyond normal day-to-day variation → requiring change in therapy.
Triggers:
- Respiratory infection (most common) — viral > bacterial
- Air pollution, non-compliance, cardiac causes
Cardinal symptoms: ↑ dyspnea + ↑ cough + ↑ sputum (volume/purulence)
Assessment
- ABG: assess hypoxemia, hypercapnia, pH
- CXR: exclude pneumonia, pneumothorax, pulmonary edema
- ECG: detect arrhythmias
Treatment (Stepwise)
1. Bronchodilators
- SABA ± SAMA (ipratropium) via nebuliser — first-line
- Combine albuterol + ipratropium in acute setting
2. Systemic Corticosteroids
- Prednisolone 30–40 mg orally for 5 days (not longer — no added benefit >2 weeks)
- Reduces treatment failures by ~46%, shortens hospital stay
- ↑ risk of hyperglycemia
3. Antibiotics
- Indicated if: ≥2 cardinal symptoms (especially purulent sputum), signs of pneumonia, need for mechanical ventilation
- Agents: amoxicillin-clavulanate, azithromycin, doxycycline, or fluoroquinolone
4. Controlled Oxygen
- Target SpO₂ 88–92% (avoid over-oxygenation → suppresses hypoxic drive in CO₂ retainers)
- Recheck ABG 30 minutes after starting O₂
5. NIV (BiPAP)
- Indication: pH <7.35 with PaCO₂ >45 mmHg + RR >25 — reduces need for intubation
6. Mechanical Ventilation
- When NIV fails or is contraindicated
- Indications: pH <7.25, PaO₂ <40 mmHg, mental status change (confusion/lethargy)
Indications for Hospitalization
- Severe dyspnea not responding to initial treatment
- New cyanosis or change in mental status
- Failure of outpatient therapy
- Significant comorbidities (CHF, arrhythmia)
- Underlying pneumonia
Indications for ICU
- pH <7.25 or PaCO₂ >60 mmHg or PaO₂ <40 mmHg
- Hemodynamic instability
- Altered consciousness
8. QUICK DIFFERENTIATORS — COPD vs. ASTHMA
| Feature | COPD | Asthma |
|---|---|---|
| Age of onset | >40 yrs | Any age (often childhood) |
| Smoking | Strong association | Not required |
| Airflow limitation | Fixed (irreversible) | Reversible |
| Post-bronchodilator FEV₁/FVC | <0.70 persists | Normalizes |
| DLCO | Often ↓ (emphysema) | Normal |
| Eosinophilia | Variable | Common |
| Diurnal variation | Minimal | Marked |
9. HIGH-YIELD MNEMONICS / EXAM FACTS
- COPD diagnosis = Spirometry: post-BD FEV₁/FVC <0.70
- GOLD 1–4 = Mild/Moderate/Severe/Very Severe (FEV₁ cutoffs: 80, 50, 30%)
- GOLD A–D = Symptom + exacerbation risk matrix → guides initial inhaler choice
- Only proven survival benefits: Smoking cessation + LTOT (in hypoxemic patients)
- LAMA > LABA for exacerbation prevention (Group C)
- ICS not monotherapy; adds pneumonia risk; use when eos >300 or persistent exacerbations
- AECOPD O₂ target = 88–92% (not 100%)
- Systemic steroids for exacerbations = 5 days (not >2 weeks)
- A1AT screen — every COPD patient at least once
- Roflumilast (PDE-4 inhibitor) = for severe COPD with chronic bronchitis phenotype + frequent exacerbations
- β-blockers are NOT contraindicated in COPD (for CV indications)
10. COMPLICATIONS OF COPD
- Cor pulmonale — RV hypertrophy from pulmonary hypertension (chronic hypoxia → vasoconstriction)
- Polycythemia — compensatory response to chronic hypoxemia
- Spontaneous pneumothorax — bullae rupture
- Respiratory failure — Type 2 (hypercapnic) in advanced disease
- Lung cancer — strong association; screen with low-dose CT if ≥20 pack-years, age 50–80, quit ≤15 years ago
- OSA-COPD overlap — higher risk of hypercapnia and pulmonary hypertension
Sources: Goldman-Cecil Medicine 26e | Washington Manual of Medical Therapeutics | Textbook of Family Medicine 9e
management of copd
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the comprehensive data needed from multiple authoritative sources (Harrison's 22e, Washington Manual, Lippincott Pharmacology, Murray & Nadel). Let me now compile the complete management guide.
COPD Management — Complete MBBS-Level Guide (GOLD Framework)
Sources: Harrison's Principles of Internal Medicine 22e (2025), Washington Manual of Medical Therapeutics, Lippincott Illustrated Reviews Pharmacology
THE BIG PICTURE — Goals of Management
- Reduce symptoms (dyspnea, cough)
- Improve exercise tolerance and quality of life
- Reduce frequency and severity of exacerbations
- Slow disease progression
- Prolong survival
PART 1: STABLE COPD MANAGEMENT
Step 0: GOLD ABE Classification (guides initial therapy)
The latest GOLD (2024/2025) uses a 3-group ABE system (updated from the older ABCD):
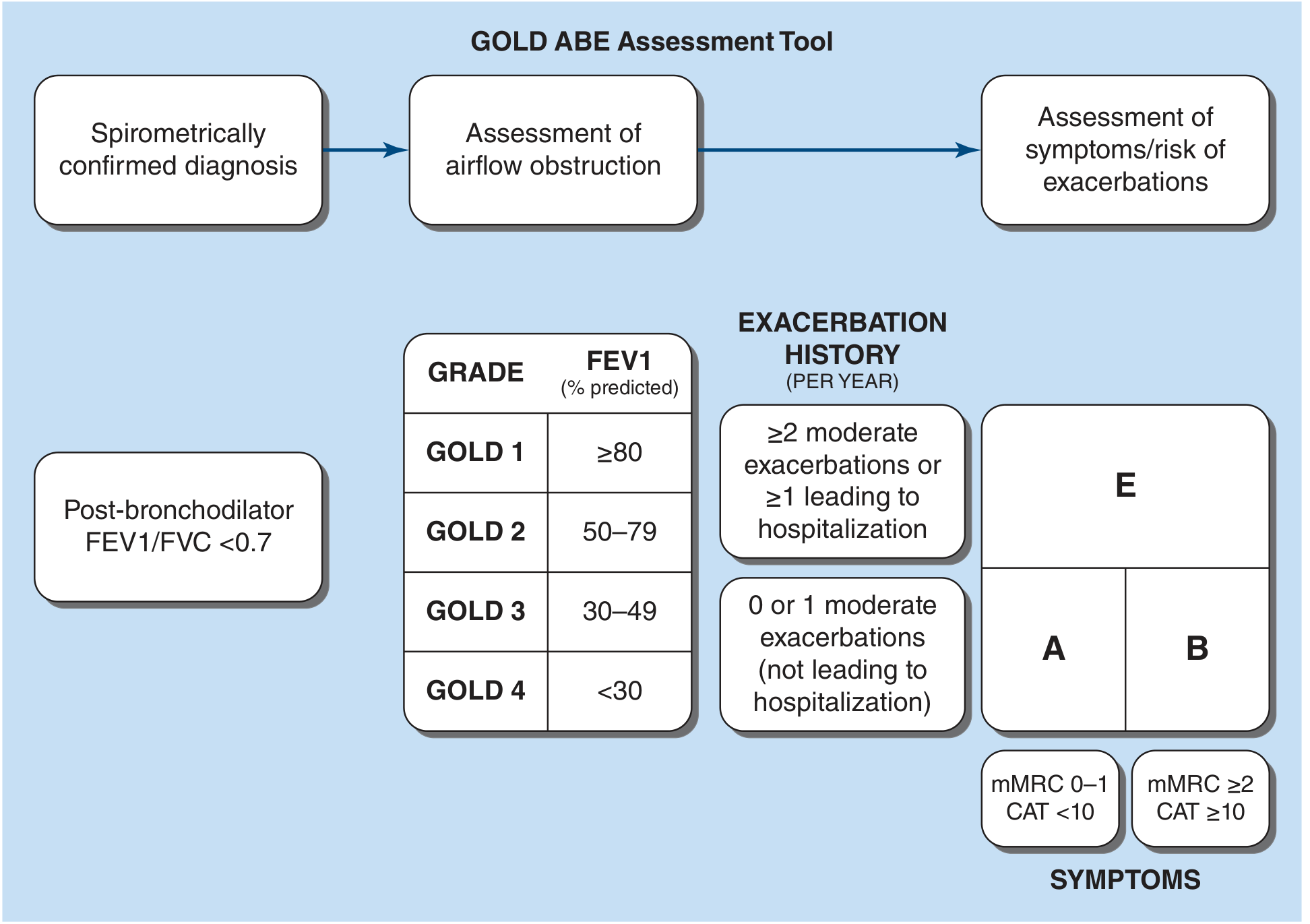
| Group | Exacerbation history | Symptoms |
|---|---|---|
| A | 0 or 1 moderate (not hospitalized) | mMRC 0-1 or CAT <10 (fewer) |
| B | 0 or 1 moderate (not hospitalized) | mMRC ≥2 or CAT ≥10 (more) |
| E | ≥2 moderate, or ≥1 leading to hospitalization | Any symptom level |
Key concept: GOLD 1-4 grades = spirometric severity (FEV₁ %) → tells you prognosis. GOLD A/B/E groups = symptoms + exacerbation risk → tells you what drug to start.
A. SMOKING CESSATION — Single Most Important Intervention
- Only intervention that slows the rate of FEV₁ decline
- Improves survival; reduces exacerbation risk
- Options:
- Nicotine replacement therapy (NRT) - patch, gum, lozenge, inhaler, nasal spray
- Varenicline (nicotinic receptor partial agonist) - most effective
- Bupropion (dopamine/noradrenaline reuptake inhibitor)
- Combine pharmacotherapy + counseling for best results
B. PHARMACOTHERAPY
1. Bronchodilators (Foundation of Treatment)
All COPD patients need at least one bronchodilator. Inhaled route is always preferred - maximizes airway drug levels, minimizes systemic side effects.
| Class | Drugs | Mechanism | Key Side Effects |
|---|---|---|---|
| SABA (Short-Acting β₂-Agonist) | Albuterol/Salbutamol, Levalbuterol | β₂ stimulation → smooth muscle relaxation | Tremor, tachycardia, palpitations, hypokalemia |
| SAMA (Short-Acting Muscarinic Antagonist) | Ipratropium | Block M3 receptor → reduces bronchoconstriction + secretions | Dry mouth, urinary retention, constipation |
| LABA (Long-Acting β₂-Agonist) | Salmeterol (bid), Formoterol (bid), Indacaterol (od), Olodaterol (od), Vilanterol (od) | Long-acting β₂ stimulation | Tremor, tachycardia, hypokalemia |
| LAMA (Long-Acting Muscarinic Antagonist) | Tiotropium (od), Umeclidinium (od), Glycopyrrolate (bid), Aclidinium (bid), Revefenacin (nebulizer) | Long-acting M3 block | Dry mouth, constipation, narrow-angle glaucoma aggravation |
| ICS (Inhaled Corticosteroid) | Fluticasone, Budesonide, Beclomethasone, Mometasone | Anti-inflammatory | Pneumonia (↑ risk), oral candidiasis, hoarseness, osteoporosis |
Memory hook: LAMA > LABA for exacerbation prevention (tiotropium is the prototype)
2. ICS Rules (Critical for Exams)
- Never use ICS as monotherapy in COPD (unlike asthma)
- When to ADD ICS:
- Eosinophils ≥300 cells/μL (strong predictor of ICS response)
- Persistent exacerbations despite dual bronchodilator (LAMA+LABA)
- Asthma-COPD overlap
- History of ≥1 hospitalization or ≥2 moderate exacerbations/year
- When to WITHDRAW ICS: <2 exacerbations/year AND eosinophils <300 cells/μL AND no hospitalizations
- Risk of pneumonia is real - don't use without indication
3. Initial Inhaled Therapy by GOLD Group
| Group | First-Line Treatment | Rationale |
|---|---|---|
| A | Any bronchodilator (SABA or SAMA as-needed) | Few symptoms, low risk |
| B | LABA or LAMA (prefer dual LABA+LAMA if symptoms persist) | Symptomatic, low exacerbation risk |
| E | LAMA (preferred); or LABA+LAMA | High exacerbation risk; LAMA reduces exacerbations more than LABA |
Escalation pathway:
Group A: Short-acting BD as needed
↓ (if symptomatic)
Group B: LABA or LAMA → LABA + LAMA
↓ (if exacerbations)
Group E: LAMA → LABA + LAMA → LABA + LAMA + ICS (if eos ≥100-300)
↓ (still exacerbating)
Add Roflumilast or Azithromycin
4. Triple Therapy (LABA + LAMA + ICS)
- Shown to reduce mortality in selected patients (eosinophils ≥300, exacerbations despite dual BD)
- Single inhaler combinations available (e.g., Fluticasone/Umeclidinium/Vilanterol)
5. Other Pharmacological Agents
| Drug | Indication | Mechanism | Side Effects |
|---|---|---|---|
| Roflumilast (oral) | Severe COPD + chronic bronchitis + frequent exacerbations despite LABA+LAMA | PDE-4 inhibitor → ↑ cAMP → anti-inflammatory | Nausea, diarrhoea, weight loss, depression (caution) |
| Azithromycin (oral, daily) | Frequent exacerbations on max inhaler therapy (nonsmokers) | Anti-inflammatory + antimicrobial | Hearing loss, cardiac arrhythmia (QTc prolongation), antibiotic resistance |
| Theophylline | Largely replaced; used if no access to inhalers | Nonspecific PDE inhibitor | Narrow therapeutic index: arrhythmias, seizures |
| N-acetylcysteine | Mucolytic; evidence weak | Breaks disulfide bonds in mucus | Generally well tolerated |
Roflumilast: not a bronchodilator, not for acute bronchospasm - purely for reducing exacerbation frequency
C. NON-PHARMACOLOGICAL THERAPY
1. Pulmonary Rehabilitation
- When to refer: All patients, especially post-exacerbation discharge, at diagnosis, and pre-surgery
- Consists of: aerobic exercise (60-80% of max capacity) + upper limb strength training + education
- Improves exercise capacity, dyspnea, quality of life
- Does NOT improve FEV₁ or survival directly but reduces hospitalization
2. Long-Term Oxygen Therapy (LTOT) - Improves Survival
Indications (must memorize):
| Condition | Threshold |
|---|---|
| Resting hypoxemia | PaO₂ ≤55 mmHg or SpO₂ ≤88% |
| Resting hypoxemia + complications | PaO₂ 56-59 mmHg or SpO₂ <89% WITH cor pulmonale / right heart failure / polycythemia (Hct >55%) |
- Must be used ≥15 hours/day to improve survival
- Target SpO₂ = 88-92% (avoid over-oxygenation → CO₂ retention)
- Nocturnal-only O₂ does NOT improve survival in isolated nocturnal desaturators
3. Noninvasive Positive Pressure Ventilation (NIV/BiPAP)
- Indication: Stable hypercapnic COPD with resting PaCO₂ ≥52 mmHg
- Improves dyspnea, exercise capacity, time to rehospitalization, possibly survival
4. Surgical Options
| Procedure | Indication |
|---|---|
| Lung Volume Reduction Surgery (LVRS) | Upper-lobe emphysema + low exercise capacity + FEV₁ 20-45% predicted |
| Bronchoscopic lung volume reduction (endobronchial valves) | Heterogeneous emphysema without collateral ventilation |
| Lung transplantation | End-stage COPD (GOLD 4), failed all other therapies |
5. Vaccines (Mandatory)
- Influenza - annually
- Pneumococcal (PCV13/PPSV23)
- COVID-19
- Tdap (pertussis)
6. Nutritional Support
- Low BMI = independent predictor of mortality in COPD
- Small frequent meals; rest before eating (reduces meal-induced dyspnea)
- Nutritional supplementation improves BMI, exercise tolerance, and quality of life in advanced disease
PART 2: ACUTE EXACERBATION OF COPD (AECOPD)
Definition
Acute worsening of respiratory symptoms beyond normal daily variation, requiring a change in medication.
Cardinal symptoms (Anthonisen criteria):
- ↑ Dyspnea
- ↑ Sputum volume
- ↑ Sputum purulence (change in color)
Pathophysiology of AECOPD (conceptual)
- Trigger (infection/pollution) → bronchospasm + mucosal edema + ↑ secretions
- ↑ Airway resistance + intrinsic PEEP (air trapping) + flattened diaphragm
- Patient can't take adequate tidal volumes → alveolar hypoventilation → ↑ PaCO₂
- Respiratory muscle fatigue → vicious cycle → respiratory acidosis
- NIV breaks this cycle by augmenting tidal volume with less effort
Triggers
- Respiratory tract infection (most common) - viral (rhinovirus, influenza) > bacterial (H. influenzae, S. pneumoniae, M. catarrhalis)
- Air pollution
- Non-compliance with medications
- Pulmonary embolism (always consider if sudden onset)
- Cardiac causes (heart failure, arrhythmia)
Initial Assessment
- ABG - quantify hypoxemia, hypercapnia, pH (pH <7.35 = acute respiratory failure)
- CXR - exclude pneumonia, pneumothorax, pulmonary edema
- ECG - detect arrhythmia, cor pulmonale (P pulmonale, right axis deviation)
- Sputum culture if purulent
- FBC - polycythemia, eosinophilia
- Serum electrolytes - hypokalemia (from SABA use)
Treatment of AECOPD - Stepwise
Step 1: Bronchodilators (Immediate)
- SABA (salbutamol/albuterol) + SAMA (ipratropium) via nebuliser
- Combine both - different mechanisms, additive effect
- Frequency: every 20 min initially in severe cases, then q4-6h
- Some patients respond better to anticholinergics, some to β₂-agonists → give both
Step 2: Controlled Oxygen
- Target: SpO₂ 88-92% (NOT 100%)
- Why? Chronic CO₂ retainers rely partially on hypoxic drive; over-oxygenation → abolishes drive → ↑ CO₂ → CO₂ narcosis
- Recheck ABG 30 minutes after starting O₂ to ensure no CO₂ rise
- Start with 28% Venturi mask (2L/min nasal cannula) and titrate
Step 3: Systemic Corticosteroids
- Prednisolone 30-40 mg orally for 5 days (not longer - no benefit beyond 2 weeks)
- IV methylprednisolone if unable to take oral
- Benefits: reduces treatment failure by ~46%, shortens hospital stay by ~1.4 days, improves FEV₁ and dyspnea faster
- Side effect: hyperglycemia (monitor blood sugar)
Step 4: Antibiotics
When to give (Anthonisen criteria):
- ≥2 of: ↑ dyspnea, ↑ sputum volume, purulent sputum - especially if purulence is one of them
- Signs of pneumonia on CXR
- Requiring mechanical ventilation (invasive or non-invasive)
| Severity | Antibiotic | Duration |
|---|---|---|
| Mild-moderate (outpatient) | Amoxicillin, Doxycycline, Azithromycin | 5-7 days |
| Moderate-severe (inpatient) | Amoxicillin-clavulanate, Cefuroxime | 5-7 days |
| Severe / Pseudomonas risk | Fluoroquinolone (Ciprofloxacin) or Piperacillin-Tazobactam | 7-10 days |
Pseudomonas risk factors: severe airflow obstruction, frequent antibiotic use, recent hospitalization
Step 5: NIV (BiPAP) — Key Decision
Indications for NIV:
- pH <7.35 with PaCO₂ >45 mmHg AND respiratory rate >25/min
- Mild-moderate respiratory acidosis (pH 7.25-7.35)
- Patient is conscious and cooperative
Benefits of NIV (vs invasive MV):
- Reduces need for intubation
- Reduces ICU mortality
- Shorter hospital stay
- Avoids complications of intubation (ventilator-associated pneumonia)
Contraindications to NIV:
- Hemodynamic instability / cardiac arrest
- Loss of consciousness / uncooperative
- Unable to protect airway (↑ aspiration risk)
- Undrained pneumothorax
- Facial trauma / anatomic contraindication
Step 6: Invasive Mechanical Ventilation
Indications:
- NIV failed or contraindicated
- pH <7.25
- PaO₂ <40 mmHg despite O₂
- Severe hypercapnia (PaCO₂ >60 mmHg)
- Hemodynamic instability
- Altered consciousness (confusion, obtundation)
- Respiratory arrest
Mortality with invasive MV for AECOPD = 17-49% for that hospitalization
Indications for Hospitalization
| Criterion | Detail |
|---|---|
| Severe dyspnea not responding to initial BD | Especially at rest |
| Mental status change | Confusion, drowsiness |
| Failure of outpatient treatment | |
| Significant comorbidities | CHF, arrhythmia, renal failure |
| Underlying precipitant | Pneumonia, pneumothorax, PE |
| Inadequate home support |
Indications for ICU Admission
- pH <7.25, severe acidosis
- PaO₂ <40 mmHg, PaCO₂ >60 mmHg
- NIV failure / contraindication
- Hemodynamic instability
- Respiratory arrest
PART 3: SURVIVAL-IMPROVING INTERVENTIONS (High-Yield)
| Intervention | Evidence |
|---|---|
| Smoking cessation | Slows FEV₁ decline; improves survival |
| LTOT (in hypoxemic patients) | Improves survival (≥15 hrs/day) |
| LVRS (selected emphysema) | Improves survival in upper-lobe emphysema + low exercise capacity |
| Triple therapy (LABA+LAMA+ICS) | Reduces mortality in selected (high eos, frequent exacerbations) |
| NIV (severe stable hypercapnia) | Possibly improves survival |
| Lung transplant | Improves quality of life; survival benefit less certain |
Key exam fact: LABAs and LAMAs improve symptoms and reduce exacerbations but do NOT slow FEV₁ decline or improve survival on their own.
PART 4: MANAGEMENT ALGORITHM (Quick Reference)
CONFIRMED COPD (FEV₁/FVC <0.70 post-BD)
|
Assess: GOLD 1-4 (FEV₁ %) + GOLD A/B/E (symptoms + exacerbations)
|
┌────────┴─────────────────────────┐
| |
STABLE COPD AECOPD
| |
Smoking cessation (always) SABA + SAMA nebulised
Vaccinations Controlled O₂ (SpO₂ 88-92%)
| Systemic steroids 5 days
Group A → SABA/SAMA PRN Antibiotics (if criteria met)
Group B → LABA or LAMA NIV if pH <7.35 + hypercapnia
Group E → LAMA → LABA+LAMA IMV if NIV fails or pH <7.25
|
If eos ≥300: add ICS
If persistent exac despite LABA+LAMA+ICS: add Roflumilast
If hypoxemic (PaO₂ ≤55): LTOT
If PaCO₂ ≥52 stable: nocturnal NIV
If upper-lobe emphysema: consider LVRS
EXAM HIGH-YIELD FACTS
- O₂ target in AECOPD = 88-92% (not 100%)
- Steroids in AECOPD = 5 days only (not >2 weeks)
- ICS never as monotherapy in COPD
- ICS adds pneumonia risk - justify before prescribing
- Eosinophil count guides ICS: eos ≥300 → add ICS; eos <100 → no ICS benefit
- LAMA preferred over LABA for exacerbation prevention (Group C/E)
- Only survival benefits: smoking cessation + LTOT + LVRS (selected) + triple therapy (selected)
- Roflumilast = oral anti-inflammatory for severe chronic bronchitis phenotype, NOT a bronchodilator
- Azithromycin daily = exacerbation prevention in nonsmokers; watch for QTc and resistance
- β-blockers are NOT contraindicated in COPD (use for cardiac indications)
- After AECOPD hospitalization: 20% readmitted within 30 days; 45% within 1 year; ~20% mortality in the following year
Sources: Harrison's Principles of Internal Medicine 22e (2025), Washington Manual of Medical Therapeutics, Lippincott Illustrated Reviews: Pharmacology, Murray & Nadel's Textbook of Respiratory Medicine
i am having difficulty remembering all those classifications in copd please help me to remember them for long time with tips tricks or mnemonic
This is a pure memory/learning question - no textbook lookup needed. Here's everything you need to permanently lock COPD classifications in your brain.
COPD Classifications — Memory Master Guide
CLASSIFICATION 1: GOLD Spirometric Grades (1-4)
What it is
Post-bronchodilator FEV₁ % predicted (in patients where FEV₁/FVC <0.70)
The Numbers
| Grade | Severity | FEV₁ % |
|---|---|---|
| 1 | Mild | ≥80% |
| 2 | Moderate | 50-79% |
| 3 | Severe | 30-49% |
| 4 | Very Severe | <30% |
Memory Trick — "The Ladder Going Down"
Think of your FEV₁ falling down a ladder:
GRADE 1 → Still on TOP of the ladder → ≥80% (mostly fine)
GRADE 2 → Halfway down → 50-79% (half-ish)
GRADE 3 → Almost at the bottom → 30-49% (thirty-something)
GRADE 4 → Hit the floor → <30% (below 30, critical)
The "50-30" Rule (easiest anchor)
Just remember two numbers: 50 and 30
- FEV₁ 50% divides Grade 2 from Grade 3
- FEV₁ 30% divides Grade 3 from Grade 4
- Grade 1 starts at 80% (easy — it's the "normal-ish" zone)
Visual Anchor
Imagine a fuel gauge in a car:
- GOLD 1 = Full tank (≥80%)
- GOLD 2 = Half tank (50-79%)
- GOLD 3 = Low fuel warning (30-49%)
- GOLD 4 = Empty, car stops (<30%)
CLASSIFICATION 2: GOLD ABE Groups (Symptom + Exacerbation Risk)
What it is
Determines which drug to start — based on symptoms (CAT/mMRC) + exacerbation history
The Grid
| Group | Exacerbations | Symptoms | Start with |
|---|---|---|---|
| A | 0-1 (not hospitalized) | Few (CAT <10 / mMRC 0-1) | Any bronchodilator |
| B | 0-1 (not hospitalized) | More (CAT ≥10 / mMRC ≥2) | LABA or LAMA |
| E | ≥2 or ≥1 hospitalized | Any | LAMA (± LABA) |
Mnemonic — "ABE = Ants, Bees, Elephants"
🐜 A = Ant — small problem, just an ant bite. Few symptoms, few exacerbations. One quick spray (any bronchodilator) is enough.
🐝 B = Bee — more painful sting, more symptoms. You feel it. Need a proper long-acting bronchodilator (LABA or LAMA).
🐘 E = Elephant — BIG problem. High exacerbation risk. Needs the strongest approach — start LAMA, escalate to dual BD, add ICS if eos ≥300.
Say it once: "Ant, Bee, Elephant — Small, Medium, Dangerous"
Alternate Mnemonic for ABE — "Airport Boarding"
Think of COPD patients boarding a plane by risk level:
- A = Economy class (mild, few symptoms, sit anywhere)
- B = Business class (more symptomatic, needs better seat = long-acting BD)
- E = Emergency exit row (high risk of exacerbation, needs most attention)
CLASSIFICATION 3: mMRC Dyspnea Scale (0-4)
The Scale
| Grade | What triggers breathlessness |
|---|---|
| 0 | Only with strenuous exercise |
| 1 | Hurrying on flat or walking uphill |
| 2 | Walks slower than peers OR stops on flat ground |
| 3 | Stops after 100 yards or a few minutes |
| 4 | Too breathless to leave the house / while dressing |
Mnemonic — "0 to 4 = Gym to Bed"
0 = GYM (only strenuous exercise affects you)
1 = HILL (hurrying or inclines)
2 = FLAT ROAD (can't keep up on flat ground)
3 = 100 YARDS (barely a cricket pitch length)
4 = BED/HOUSE (can't even dress yourself)
The "CAT ≥10 = mMRC ≥2" Bridge
Both mean "symptomatic enough to need a long-acting bronchodilator"
- CAT <10 = mMRC 0-1 = Group A (few symptoms)
- CAT ≥10 = mMRC ≥2 = Group B or E (more symptoms)
CLASSIFICATION 4: Exacerbation Severity
| Type | Definition | Treatment |
|---|---|---|
| Mild | Only needs ↑ BD use | Managed at home |
| Moderate | Needs systemic steroids and/or antibiotics | Outpatient or ED |
| Severe | Requires hospitalization | Inpatient |
| Very Severe | ICU / respiratory failure | ICU |
Mnemonic — "MBA-I"
- More inhaler → Mild
- Budesonide/antibiotics → Moderate
- Admit to hospital → Severe
- ICU → Very Severe
THE MASTER MEMORY FRAMEWORK
Link all 4 systems together in ONE sentence:
"GOLD 1-4 tells you HOW BAD the lungs are. ABE tells you WHAT TO PRESCRIBE. mMRC/CAT tells you HOW BREATHLESS they are. Exacerbation count tells you HOW RISKY they are."
The "Report Card" Analogy
Think of COPD like a student's report card:
| Item | What it measures | Analogy |
|---|---|---|
| GOLD 1-4 | FEV₁ % = lung damage | Subject grade (A to F based on marks) |
| CAT/mMRC | Symptom burden | Attendance (how much it affects daily life) |
| Exacerbation count | Flare-up risk | Detention count (how many times things went wrong) |
| ABE group | Combined symptom + exacerbation risk | Overall grade that decides next steps |
QUICK RECALL TABLE — 30-Second Review
GOLD GRADES (FEV₁%): ≥80 → 50 → 30 → <30
G1 G2 G3 G4
Mild Mod Sev V.Sev
GOLD GROUPS: Symptoms low + low exac = A → any BD
Symptoms HIGH + low exac = B → LABA/LAMA
HIGH exacerbations (any symptoms) = E → LAMA
mMRC: 0=Gym 1=Hill 2=Flat 3=100yards 4=Housebound
CAT: <10 = fewer symptoms (= mMRC 0-1 = Group A)
≥10 = more symptoms (= mMRC ≥2 = Group B/E)
ONE FINAL TRICK — The "1-2-3" Rule
| Threshold | Meaning |
|---|---|
| FEV₁ 80% | GOLD 1 starts here |
| FEV₁ 50% | GOLD 1/2 boundary |
| FEV₁ 30% | GOLD 3/4 boundary |
| CAT 10 | Symptom cutoff for group A vs B/E |
| Exac ≥2 or hosp ≥1 | Group E threshold |
| Eos ≥300 | Add ICS |
| PaO₂ ≤55 or SpO₂ ≤88% | Start LTOT |
| pH <7.35 + hypercapnia | Start NIV |
| pH <7.25 | Consider intubation |
Memorize these 9 numbers and you can answer almost any COPD management MCQ.
SPACED REPETITION TIP
Test yourself in this order:
- Day 1: Draw the ABE grid from memory (groups + what triggers each)
- Day 2: Recite GOLD 1-4 cutoffs without looking
- Day 3: Write the mMRC scale descriptions 0-4 from memory
- Day 7: Draw the full management ladder (A→B→E with drugs at each step)
- Day 14: Do a practice MCQ on a AECOPD case using pH + PaCO₂ values
Each time you revise, say the "Ant-Bee-Elephant" mnemonic out loud — it sticks because it's visual and slightly silly, which is exactly why memory works.
management of asthma
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive data from Katzung pharmacology, Family Medicine textbook, Creasy & Resnik, and Murray & Nadel. I have everything needed to write a thorough, crisp management guide. Let me now compile it.
Management of Asthma — Complete MBBS-Level Guide
Sources: Katzung's Basic & Clinical Pharmacology 16e, Textbook of Family Medicine 9e, Harrison's Principles of Internal Medicine 22e (2025), Murray & Nadel's Textbook of Respiratory Medicine
CORE CONCEPT FIRST
Asthma has two treatment domains - always think in both:
| Domain | Question | Key metric |
|---|---|---|
| Present | Are symptoms controlled NOW? | Symptom frequency, rescue inhaler use, nocturnal awakenings, activity limitation |
| Future | Is the patient at risk of exacerbations? | Past exacerbation history, FEV₁, eosinophilia, FeNO |
Managing only the "present" domain while ignoring "future" risk is incomplete care. A patient comfortable on frequent SABA use may still be at high risk of a fatal attack.
CLASSIFICATION OF ASTHMA SEVERITY
(For patients NOT yet on long-term controller therapy — used to decide where to START)
| Severity | Symptom Frequency | Nighttime Awakenings | SABA Use | FEV₁ % predicted | Start at Step |
|---|---|---|---|---|---|
| Intermittent | ≤2 days/week | ≤2x/month | ≤2 days/wk | >80% | Step 1 |
| Mild Persistent | >2 days/wk (not daily) | 3-4x/month | >2 days/wk (not daily) | >80% | Step 2 |
| Moderate Persistent | Daily | >1x/week (not nightly) | Daily | 60-80% | Step 3 |
| Severe Persistent | Throughout the day | Often 7x/week (nightly) | Several times/day | <60% | Step 4-5 |
Two numbers to anchor this: FEV₁ 60% separates moderate from severe. "Daily symptoms" = at minimum moderate.
CLASSIFICATION OF ASTHMA CONTROL
(For patients already ON therapy — used to decide whether to step UP, step DOWN, or maintain)
| Control Level | Symptoms | Nighttime | SABA use | Activity | Exacerbations |
|---|---|---|---|---|---|
| Well controlled | ≤2 days/wk | ≤2x/month | ≤2 days/wk | None | 0-1/year |
| Not well controlled | >2 days/wk | 3-4x/month | >2 days/wk | Some | ≥2/year |
| Very poorly controlled | Throughout the day | 7x/week | Several times/day | Extremely limited | ≥2/year |
PART 1: STABLE ASTHMA — GINA/NAEPP STEPWISE THERAPY
Principle: Step Up / Step Down
- Step Up if not well controlled
- Step Down after ≥3 months of good control (to find minimum effective dose)
- Reassess every 2-6 weeks when stepping up, 3 months when stepping down
THE 5-STEP LADDER
STEP 1 — Intermittent Asthma (mildest)
- Reliever only: SABA (salbutamol/albuterol) as-needed
- No daily controller needed
- GINA update: Low-dose ICS-formoterol as-needed preferred over SABA alone (reduces exacerbation risk even in mild asthma)
- Educate on action plan for severe attacks: up to 4 puffs albuterol every 20 min x1 hour
STEP 2 — Mild Persistent
- Add daily controller: Low-dose ICS (e.g., budesonide 200-400 mcg/day, fluticasone 100-250 mcg/day)
- Alternative to ICS: Leukotriene receptor antagonist (LTRA) - montelukast, zafirlukast (less effective than ICS but useful in patients with nasal polyps, aspirin sensitivity, or exercise-induced asthma)
- Continue SABA as-needed reliever
STEP 3 — Moderate Persistent
Two equally valid options:
- Low-dose ICS + LABA (preferred - most effective) - e.g., fluticasone + salmeterol (Seretide/Advair), budesonide + formoterol (Symbicort)
- Medium-dose ICS alone
- LABA should NEVER be used as monotherapy in asthma (black-box warning - increased asthma deaths with LABA alone; warning removed for ICS-LABA combinations)
- Alternative additions: LTRA, theophylline, tiotropium (LAMA)
STEP 4 — Severe Persistent (not controlled on Step 3)
- Medium-to-high dose ICS + LABA (core)
- Add-on options:
- LAMA (tiotropium) - improves lung function and reduces exacerbations in patients with persistent obstruction, high symptom burden, exacerbation history
- LTRA (montelukast)
- Sustained-release theophylline
- Refer to specialist
STEP 5 — Severe Refractory Asthma
- High-dose ICS + LABA +/- LAMA
- Biologics (targeted therapy) based on phenotype:
| Biologic | Target | Indication | Key Point |
|---|---|---|---|
| Omalizumab | Anti-IgE | Allergic asthma, IgE ≥30-700 IU/mL | For atopic (allergic) phenotype |
| Mepolizumab, Reslizumab | Anti-IL-5 | Eosinophilic asthma | Blood eos ≥300 |
| Benralizumab | Anti-IL-5Rα | Eosinophilic asthma | Depletes eosinophils |
| Dupilumab | Anti-IL-4Rα | Type 2 (T2-high) asthma | Blocks IL-4 and IL-13 signaling |
| Tezepelumab | Anti-TSLP | Broadest indication - any phenotype | Works in T2-high AND T2-low |
- Oral corticosteroids (low-dose) as last resort — significant toxicity with long-term use
SMART Strategy (Single Maintenance And Reliever Therapy)
Budesonide-formoterol used as BOTH the daily controller AND the rescue inhaler
- Works because formoterol has rapid onset (like SABA) + long duration
- Patient uses the same inhaler for scheduled doses AND PRN relief
- Evidence: as effective as higher-dose ICS + separate SABA
- Now in both US (NAEPP 2020) and GINA guidelines
- Available devices: Symbicort (budesonide/formoterol), Breztri, Airsupra (budesonide/albuterol)
KEY DRUGS IN DETAIL
| Drug Class | Examples | Mechanism | Side Effects | Notes |
|---|---|---|---|---|
| SABA | Salbutamol (albuterol), Terbutaline, Levalbuterol | β₂-agonist → bronchial smooth muscle relaxation | Tremor, tachycardia, palpitations, hypokalemia | Drug of choice in acute bronchospasm |
| LABA | Salmeterol (slow onset), Formoterol (fast onset), Vilanterol, Indacaterol | Long-acting β₂-agonist | Same as SABA | Never use as monotherapy; only with ICS |
| ICS | Fluticasone, Budesonide, Beclomethasone, Mometasone, Ciclesonide | Reduce airway inflammation (alter gene expression) | Oral candidiasis, hoarseness, dysphonia (local); at high doses: adrenal suppression, osteoporosis, growth retardation (children) | Rinse mouth after use to prevent candidiasis |
| SAMA | Ipratropium | M3 receptor block | Dry mouth, urinary retention | Additive with SABA in acute severe asthma (ED use); not preferred over β₂-agonists for chronic use |
| LAMA | Tiotropium | Long-acting M3 block | Dry mouth | Add-on at Step 4-5; not first-line in asthma |
| LTRA | Montelukast, Zafirlukast, Zileuton | Block cysteinyl leukotriene receptors (CysLT1) | Mood changes, depression (montelukast - FDA warning) | Good for aspirin-exacerbated asthma, exercise-induced, allergic rhinitis co-morbidity |
| Theophylline | Aminophylline (IV), Theophylline (oral) | Nonspecific PDE inhibitor; also adenosine antagonist | Narrow therapeutic index: nausea, arrhythmias, seizures | Largely replaced; monitor serum levels (target 5-15 mcg/mL) |
| Cromolyn | Cromolyn sodium, Nedocromil | Mast cell stabilizer | Very safe; cough | Largely replaced by ICS; used in exercise-induced asthma |
PART 2: ACUTE SEVERE ASTHMA (ASTHMA ATTACK / STATUS ASTHMATICUS)
Definition of Severity
| Feature | Moderate | Severe | Life-Threatening |
|---|---|---|---|
| Speech | Sentences | Words/phrases | Cannot speak |
| Respiratory rate | Increased | >25/min | Slow or absent |
| Pulse | <110 | ≥110 | Bradycardia |
| SpO₂ | >95% | 92-95% | <92% |
| PEFR | >50% | 33-50% | <33% |
| PaCO₂ | Normal | Normal-raised | >45 mmHg (exhaustion) |
| Mental status | Alert | Agitated | Altered/drowsy |
Silent chest + cyanosis + bradycardia + PaCO₂ rising = near-fatal asthma - act immediately
Treatment of Acute Severe Asthma — Stepwise
1. Oxygen
- Target SpO₂ ≥94-95% (unlike COPD, aim higher in asthma)
- Humidified oxygen via face mask
- Unlike COPD, there is no concern about suppressing hypoxic drive
2. Inhaled SABA (First-Line, Immediate)
- Salbutamol (albuterol) 2.5-5 mg via nebuliser every 20 minutes × 3 doses in the first hour, then as needed
- MDI with spacer is equally effective as nebuliser (2-4 puffs every 20 min)
- In severe/life-threatening: continuous nebulisation
- Can use IV salbutamol if inhaled route is inadequate (rarely)
3. Inhaled SAMA (Add to SABA)
- Ipratropium 0.5 mg nebulised combined with salbutamol
- Additive effect - reduces hospitalisation rates in severe acute asthma
- Most beneficial in first 24-48 hours of presentation
4. Systemic Corticosteroids (Give Early - Within 1 Hour)
- Prednisolone 40-50 mg orally OR Hydrocortisone 200 mg IV if unable to swallow
- Duration: 5 days (no benefit to longer courses in most patients)
- Reduces: inflammation, relapse, need for hospitalisation
- Effect takes 4-6 hours to manifest - give EARLY
5. IV Magnesium Sulphate
- 2g IV over 20 minutes (single dose)
- Mechanism: Mg²⁺ blocks calcium entry into smooth muscle → bronchodilation
- Indications:
- Severe asthma not responding to bronchodilators after 1 hour
- SpO₂ <92% / life-threatening features
- Dose in children: 50 mg/kg (max 2g)
- Monitor: BP and cardiac rhythm during infusion
6. Controlled Oxygen + Monitoring
- Pulse oximetry continuous
- Peak flow before and after each treatment
- ABG if SpO₂ <92% or severe attack
7. IV Aminophylline / Theophylline (Controversial, Rarely Used)
- Used if inadequate response to all above
- Load: 5-6 mg/kg IV over 20-30 min (do not give loading dose if already on theophylline)
- Maintenance: 0.5 mg/kg/hr infusion
- Monitor ECG (arrhythmias), serum levels
- Largely fallen out of favour given poor benefit-risk ratio
8. Heliox
- Helium-oxygen mixture (70:30)
- Lower density reduces turbulent flow in narrowed airways
- Used as bridge therapy in refractory severe asthma
- Limited evidence, not widely available
9. Intubation and Mechanical Ventilation (Last Resort)
Indications:
- Respiratory arrest or near-arrest
- Altered consciousness
- Exhaustion, rising PaCO₂ despite treatment
- SpO₂ <92% not improving
- Silent chest
Intubation in asthma is high-risk: risk of barotrauma, tension pneumothorax, haemodynamic instability. Use lowest tidal volumes, long expiratory time, and permissive hypercapnia strategy.
10. Discharge Criteria and Follow-up
- PEFR ≥75% predicted on discharge
- SpO₂ ≥95% on room air
- Prescribe ICS at discharge (for all except mild intermittent asthma)
- Oral prednisolone course to complete
- Written asthma action plan
- Review inhaler technique
- Follow-up within 48 hours
PART 3: TRIGGERING FACTORS — ALWAYS ADDRESS
| Trigger Category | Examples |
|---|---|
| Allergens | House dust mite, animal danders, pollen, mould, cockroach excreta |
| Infections | Viral URTI (most common trigger for acute attacks) |
| Exercise | Exercise-induced bronchoconstriction (EIB) |
| Irritants | Tobacco smoke, strong odours, air pollutants |
| Drugs | Aspirin/NSAIDs (aspirin-exacerbated respiratory disease), β-blockers (even eye drops!) |
| Occupational | Isocyanates, flour dust, latex |
| Emotional stress | Laughter, crying |
| GERD | Acid reflux triggers reflex bronchoconstriction |
| Cold air / weather |
Always ask about aspirin and β-blocker use. β-blockers (including topical eye drops for glaucoma) can precipitate fatal bronchospasm in asthmatics.
PART 4: SPECIAL SITUATIONS
Exercise-Induced Asthma
- Pre-treatment: SABA 15-20 min before exercise
- Alternatives: LTRA (montelukast), cromolyn, warm-up exercises
- ICS reduces airway hyperresponsiveness over time
Aspirin-Exacerbated Respiratory Disease (AERD)
- Triad: Asthma + nasal polyps + aspirin/NSAID sensitivity (Samter's Triad)
- Avoid all NSAIDs, aspirin
- LTRA (montelukast) particularly useful
- Aspirin desensitization possible in specialized centers
Asthma in Pregnancy
- Poorly controlled asthma is more dangerous than well-treated asthma for the fetus
- ICS are safe in pregnancy (all categories) - do not stop
- SABA is safe
- Systemic steroids: use when needed (risk of uncontrolled asthma > risk of steroid)
- Monitor PEFR regularly throughout pregnancy
PART 5: MANAGEMENT ALGORITHM — Quick Reference
ASTHMA CONFIRMED (reversible airflow obstruction)
|
Assess SEVERITY (if not on treatment)
or CONTROL (if already on treatment)
|
┌────────────────────────────────────────────┐
STABLE ACUTE ATTACK
| |
Step 1: Intermittent → SABA PRN O₂ → target SpO₂ ≥94%
Step 2: Mild persist → + low ICS Nebulised SABA q20min x3
Step 3: Mod persist → ICS + LABA Add ipratropium (severe)
Step 4: Severe → medium-high ICS Systemic steroids EARLY
+ LABA + LAMA/LTRA IV Mg²⁺ if not improving
Step 5: Refractory → biologics Aminophylline (rarely)
Omalizumab/Mepolizumab/ Intubate if life-threatening
Dupilumab/Tezepelumab
|
SMART strategy: Budesonide-formoterol
as both controller AND reliever
HIGH-YIELD EXAM FACTS
- Drug of choice for acute bronchospasm: Inhaled SABA (salbutamol)
- First-line controller: Low-dose ICS
- LABA NEVER monotherapy in asthma (risk of asthma death)
- Most effective add-on to ICS: LABA (better than doubling ICS dose)
- ICS side effect: Rinse mouth to prevent oral candidiasis
- SMART regimen: Budesonide-formoterol as both controller + reliever
- IV Mg²⁺ dose: 2g over 20 min for acute severe asthma
- O₂ target in acute asthma: ≥94-95% (NOT 88-92% as in COPD)
- Rising PaCO₂ in acute asthma = danger sign (patient is tiring out)
- β-blockers contraindicated in asthma (even topical)
- Aspirin + asthma + nasal polyps = Samter's Triad → use LTRA
- Montelukast black-box warning: Neuropsychiatric events (depression, suicidal ideation)
- Omalizumab: Anti-IgE biologic → for allergic asthma
- Tezepelumab: Broadest biologic → anti-TSLP → works in both T2-high and T2-low asthma
- Theophylline target serum level: 5-15 mcg/mL
Sources: Katzung's Basic & Clinical Pharmacology 16e | Textbook of Family Medicine 9e | Harrison's Principles 22e | Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.