Connection between Ligamentum Teres and Capsular Ligament
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Here is a comprehensive account of the connection between the Ligamentum Teres and the Capsular Ligaments of the hip joint.
Ligamentum Teres and Its Relationship to the Capsular Ligaments
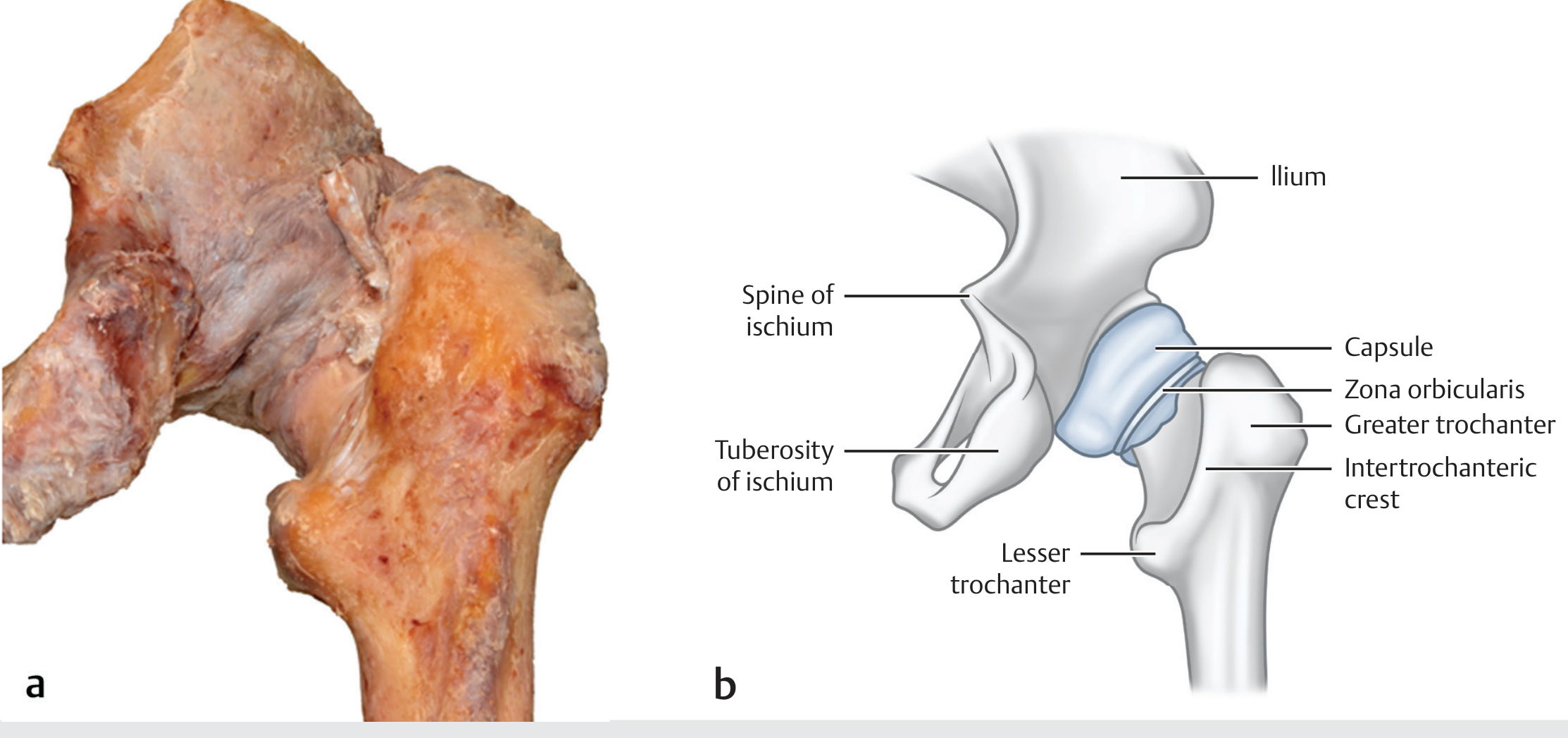
Overview of the Hip Capsule
The hip joint capsule is a strong fibrous structure. Proximally it attaches to the periphery of the acetabulum; distally it attaches to the intertrochanteric line anteriorly and to the femoral neck posteriorly. The capsular (extracapsular) ligaments — the iliofemoral (Y ligament of Bigelow), ischiofemoral, and pubofemoral ligaments — are spirally oriented longitudinal thickenings of this capsule that reinforce and stabilize the hip joint.
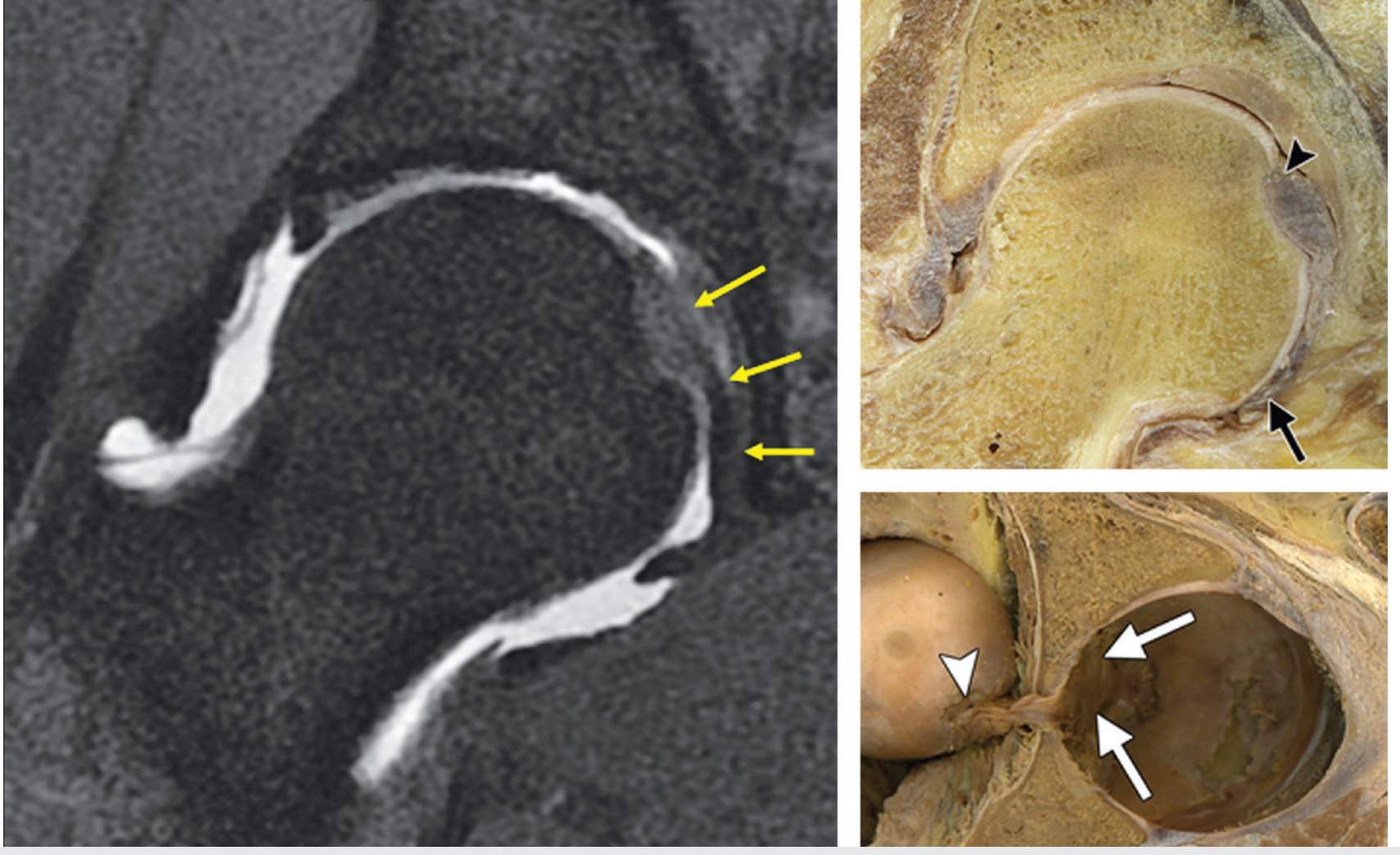
The Ligamentum Teres is Intracapsular but Extrasynovial
This is the most fundamental anatomical distinction:
- The ligamentum teres (also called ligamentum capitis femoris) lies inside the fibrous capsule — it is intracapsular.
- However, it is extrasynovial: the synovial membrane ensheaths it but does not include it within its lining, analogous to the anterior cruciate ligament in the knee.
- The fibrous capsule of the hip is thus lined by synovium, which reflects over and around the ligamentum teres, covering it without engulfing it into the synovial cavity proper.
"The fibrous capsule of the hip joint is lined by a synovial membrane. It ensheaths the ligamentum teres, which is intracapsular but extrasynovial, similar to the anterior cruciate ligament in the knee." — Imaging Anatomy: Bones, Joints, Vessels and Nerves
Proximal Attachment: Shared with the Capsule at the Acetabulum
The ligamentum teres arises from the transverse acetabular ligament, with attachments to the periosteum along the ischial and pubic margins of the acetabular notch by two bands (fasciculi). Critically, the transverse acetabular ligament itself is continuous with the periosteum and the joint capsule dorsally — meaning the proximal root of the ligamentum teres shares a common bony and connective tissue foundation with the capsular complex.
Functional Interaction in Hip Stability
| Structure | Location | Role |
|---|---|---|
| Capsular ligaments (iliofemoral, ischiofemoral, pubofemoral) | Extracapsular thickenings of the fibrous capsule | Primary stabilisers; tightest in extension and internal rotation |
| Ligamentum teres | Intracapsular, extrasynovial | Secondary stabiliser; most taut in flexion, adduction, and external rotation; lax in abduction and internal rotation |
Both structures must be disrupted for a hip dislocation to occur: "For the hip to dislocate, the ligamentum teres and at least a portion of the capsule must be disrupted." — Rockwood & Green's Fractures in Adults, 10th ed.
Vascular Connection Through the Capsule
The ligamentum teres carries the foveal artery (anterior branch of the posterior division of the obturator artery), which supplies the femoral head. In children (birth to ~4 years), this is a significant source of femoral head blood supply. In adults, the capsular retinacular vessels (from the medial femoral circumflex artery) are the dominant supply, with the ligamentum teres contribution becoming minimal. Elevated intracapsular pressure (from joint effusion) can impede capsular retinacular flow — a key mechanism in avascular necrosis after intracapsular fractures.
Summary
| Relationship | Detail |
|---|---|
| Position within capsule | Ligamentum teres is intracapsular but extrasynovial |
| Proximal root | Shares origin via transverse acetabular ligament, which is continuous with the joint capsule |
| Stabilisation | Both structures required for hip stability; rupture of both = dislocation |
| Capsular ligament type | Ligamentum teres is a separate intra-articular ligament, not a thickening of the capsule (unlike the three extracapsular ligaments) |
| Blood supply relationship | Ligamentum teres carries foveal artery; capsular retinacular vessels are the dominant adult supply |
Sources: Imaging Anatomy: Bones, Joints, Vessels and Nerves, Vol. 3, pp. 737–740; Miller's Review of Orthopaedics, 9th ed., p. 183–184; Rockwood & Green's Fractures in Adults, 10th ed.
superior pubic ramus
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Searching Images
superior pubic ramus anatomy pelvic bone
Finding Sources
Here is a comprehensive anatomy of the Superior Pubic Ramus.
Superior Pubic Ramus — Anatomy
Position and Overview
The pubis forms the anterior and inferior part of the pelvic (hip) bone. It consists of:
- A body (medial, forms the pubic symphysis)
- A superior pubic ramus (projects posterolaterally)
- An inferior pubic ramus (projects laterally and inferiorly to meet the ischial ramus)
The superior pubic ramus projects posterolaterally from the body, and at its base (directed toward the acetabulum) joins with the ilium and ischium — contributing to the formation of the acetabulum.
Key Surfaces and Landmarks
| Feature | Description |
|---|---|
| Pecten pubis (Pectineal line) | Sharp superior margin of the superior pubic ramus; triangular surface facing superiorly; part of the linea terminalis and the pelvic inlet |
| Pubic crest | Rounded ridge on the superior surface of the body; continuous anteriorly with the pectineal line; also part of the linea terminalis |
| Pubic tubercle | Lateral projection from the superior pubic ramus; attachment of the inguinal ligament, rectus abdominis, and pyramidalis |
| Obturator groove | Groove on the inferior surface; forms the upper margin of the obturator canal |
| Iliopubic eminence | Junction of the superior pubic ramus with the ilium; landmark for the iliopectineal arch |
The pecten pubis is the key component of the linea terminalis (pelvic brim) — running from the sacral promontory → arcuate line → pecten pubis → pubic crest → pubic symphysis, forming the boundary of the pelvic inlet.
Obturator Canal and Foramen
At the top of the obturator foramen lies the obturator canal, bordered by:
- The obturator membrane
- The obturator muscles
- The superior pubic ramus (superiorly, via the obturator groove)
The obturator nerve and vessels pass from the pelvic cavity to the thigh through this canal.
The obturator ring itself is formed by: pubis medially → superior pubic ramus (superiorly) → inferior pubic ramus (inferiorly) → ischium.
Muscle Attachments
| Muscle | Attachment on Superior Pubic Ramus |
|---|---|
| Pectineus | Pecten pubis (pectineal line) |
| Adductor longus | Superior pubic ramus and anterior symphysis |
| Adductor brevis | Inferior pubic ramus (adjacent) |
| Puborectalis | Superior pubic ramus, both sides of symphysis |
| Rectus abdominis / Pyramidalis | Pubic crest / pubic tubercle |
Ligament Connections
- Inguinal ligament: attaches to the pubic tubercle laterally
- Lacunar ligament (Gimbernat's): curves downward from the medial attachment of the inguinal ligament
- Pectineal ligament (Cooper's ligament): extension of the lacunar ligament running along the superior pubic ramus; forms the medial boundary of the femoral ring — clinically important in femoral hernia entrapment
- Pubofemoral ligament: arises from the obturator crest and superior pubic ramus; thickening of the hip joint capsule inferiorly
Nerve Relations
The accessory obturator nerve (present in ~30% of individuals, L3–L4) descends along the medial border of psoas major, crosses the superior pubic ramus behind pectineus, supplies pectineus, and gives articular branches to the hip joint — a key variant in regional analgesia.
Vascular Relations
The corona mortis ("crown of death") is an anastomosis between the obturator artery and the external iliac / inferior epigastric artery — it courses behind the superior pubic ramus and is at risk of unrecognized hemorrhage in anterior pelvic fractures. The aberrant obturator artery variant arises near the superior pubic ramus from the deep inferior epigastric artery in a significant proportion of individuals.
Clinical Importance
| Scenario | Relevance |
|---|---|
| Pelvic ring fractures | Superior pubic ramus fracture = Tile type A (stable); disrupted with lateral compression (LC) injuries; avulsion fractures of the ischial spine + superior pubic ramus on CT = evidence of rotational pelvic instability |
| Femoral hernia | Cooper's ligament along the superior pubic ramus = key repair landmark |
| Corona mortis injury | Vessel behind the ramus → life-threatening haemorrhage in pelvic trauma |
| PENG block (hip analgesia) | Linear US probe placed along inguinal crease between pubic ramus and ASIS; targets femoral, accessory obturator, and obturator nerve branches |
| Transobturator sling (TVT-O) | Inferior pubic ramus and obturator foramen are the landmarks; the superior ramus defines the superior boundary |
Sources: Gray's Anatomy for Students, pp. 518–519; Berek & Novak's Gynecology, p. 149–150; THIEME Atlas of Anatomy: General Anatomy & Musculoskeletal System; Imaging Anatomy: Bones, Joints, Vessels and Nerves, Vol. 3; Barash Clinical Anesthesia, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.