anesthesia and position and intruments of rigid esophagoscopy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Searching the Web
rigid esophagoscopy anesthesia patient position instruments Jackson Negus
Reading Web Page
https://entokey.com/esophagoscopy-and-hypopharyngoscopy
I now have comprehensive information from both the textbook library and web sources. Here is a complete, well-organized answer:
Rigid Esophagoscopy: Anesthesia, Position, and Instruments
1. Anesthesia
Rigid esophagoscopy is performed under general anesthesia with endotracheal intubation. This is mandatory because:
- The rigid scope requires complete relaxation of the pharyngeal and cricopharyngeal muscles to allow safe passage
- The gag reflex makes any significant intervention (foreign body removal, biopsy, dilation) impossible without general anesthesia
- Muscle relaxants facilitate passage through the upper esophageal sphincter (UES) - sedation and anesthesia can also cause relaxation of the esophageal sphincters, sometimes allowing spontaneous migration of a foreign body into the stomach
- Standard cardiopulmonary monitoring with pulse oximetry is required throughout
Note: Flexible esophagoscopy, by contrast, can be performed under topical anesthesia (4% lidocaine spray + 0.5% tetracaine pledgets + 2% lidocaine gel) with or without intravenous sedation, which is why it is generally preferred for purely diagnostic indications.
2. Patient Positioning
There are two approaches described in the literature, and they are not contradictory - the difference depends on the extent of the intended scope passage:
For Upper/Cervical Esophagoscopy (most common rigid procedure)
- Patient is placed supine
- The neck is extended using a head ring and shoulder roll (shoulders on the table, head elevated and supported on a ring)
- This extension brings the cervical spine into a straight line with the thoracic spine, creating a straight channel through which the rigid scope can be advanced
- The table is rotated 90 degrees away from the anesthesia station to give the surgeon room to maneuver
- Assess neck range of motion before induction - patients with trismus, short/wide neck, or limited cervical mobility may not tolerate sufficient extension
Neutral/Sniffing Position Alternative
- Some sources (Ento Key/Cummings) note that neutral position without aggressive head extension may also be used, as excessive extension with a shoulder roll can paradoxically make passage more difficult in some patients
- The posterior pharynx follows the cervical lordosis; aligning the neck avoids a curve that would impede the straight tube
- Prominent cervical osteophytes are a relative contraindication as they impair advancement and increase risk of mucosal trauma
3. Esophagoscope Sizes
| Patient | Scope Size |
|---|---|
| Child | 5 mm × 35 mm or 6 mm × 35 mm |
| Adult | 9 mm × 50 mm |
The adult scope allows the surgeon to pass from the incisor teeth through the following landmarks (distances from upper incisor teeth):
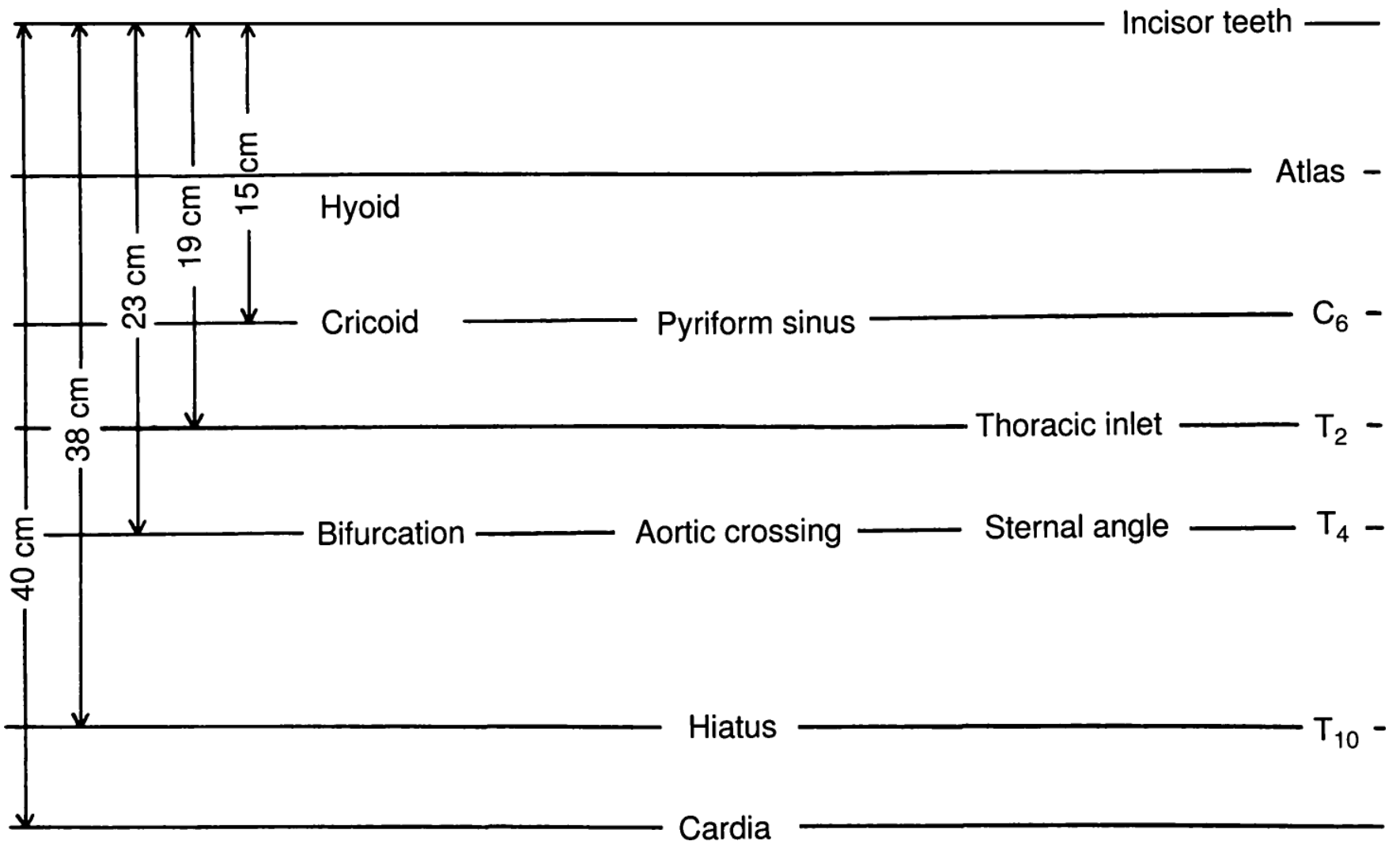
Figure: Relative landmarks for esophagoscopy (from KJ Lee's Essential Otolaryngology)
| Landmark | Distance from Incisors |
|---|---|
| Hyoid | 15 cm |
| Cricoid / Pyriform sinus / C6 | 19-23 cm |
| Thoracic inlet / T2 | 38 cm |
| Bifurcation / Aortic crossing / T4 | 40 cm |
| Hiatus / T10 | ~40+ cm |
4. Instruments and Equipment
The Esophagoscope Itself
- A rigid, hollow, straight metal tube with a beveled distal tip
- Has a proximal light source (fiberoptic illumination)
- A camera head can be attached for projection onto a monitor
- Two major traditional designs:
- Chevalier Jackson esophagoscope - open-tube, no optics, instruments passed alongside the line of sight; the pioneer of modern rigid esophagoscopy in the early 1900s
- Negus esophagoscope - similar design with slight refinements for European practice
Instruments Passed Through or Alongside the Scope
| Instrument | Purpose |
|---|---|
| Grasping/retrieval forceps | Foreign body removal (coin, bone, safety pin, food bolus) |
| Biopsy forceps | Tissue sampling from esophageal lesions |
| Optical forceps | Used under direct vision for foreign body removal |
| Cannula suction | Aspiration of secretions and blood |
| Balloon dilators | Management of strictures |
| Injection needles | Intralesional injection |
Key Advantage of Rigid over Flexible
Rigid esophagoscopy allows larger suction cannulas and larger-caliber instruments - this is particularly important for foreign body retrieval and intervention in the hypopharynx, cricopharyngeal sphincter, and cervical esophagus (the first ~5 cm).
5. Relative Contraindications to Rigid Esophagoscopy
- Aneurysm of the aorta
- Spinal deformities / prominent osteophytes
- Esophageal burns with concurrent steroid treatment
- Trismus or severely limited neck range of motion
- Active cervical instability
6. Technique Summary (Step-by-Step)
- Assess neck range of motion before induction
- Induce general anesthesia and perform endotracheal intubation
- Extend neck with head ring + shoulder roll; rotate table 90° from anesthesia station
- Insert scope with bevel facing posteriorly/downward, directed toward posterior oropharyngeal mucosa in midline
- Advance the scope caudally under direct visualization, staying posterior to the endotracheal tube
- Enter the UES gently - this is the narrowest, most dangerous point
- Advance to the required depth (pathology level)
- Perform the intervention (biopsy, foreign body retrieval, dilation) using appropriate forceps or instruments
- Withdraw while inspecting the mucosa on the way out for perforations, lacerations, or residual pathology
- Document findings and confirm hemostasis
Sources: - KJ Lee's Essential Otolaryngology, p. 184-185 | - Cummings Otolaryngology Head and Neck Surgery | - Entokey Esophagoscopy chapter | - VUMC Global Surgical Atlas - Rigid Upper Esophagoscopy
This is a shared conversation. Sign in to Orris to start your own chat.