Apasia types
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I have comprehensive data. Here is the full, well-organized answer:
Aphasia: Types and Classification
Aphasia is an acquired disorder of language (not speech mechanics) caused by brain lesions - most commonly stroke in the left (dominant) hemisphere. The two primary axes for classification are: fluency of spontaneous speech, and repetition ability.
Key Examination Parameters
To classify aphasia at bedside, assess:
- Fluency - spontaneous speech (rate, grammar, word choice)
- Comprehension - understanding commands and questions
- Repetition - ability to repeat phrases
- Naming - confrontation naming
- Reading and Writing
The Main Aphasic Syndromes
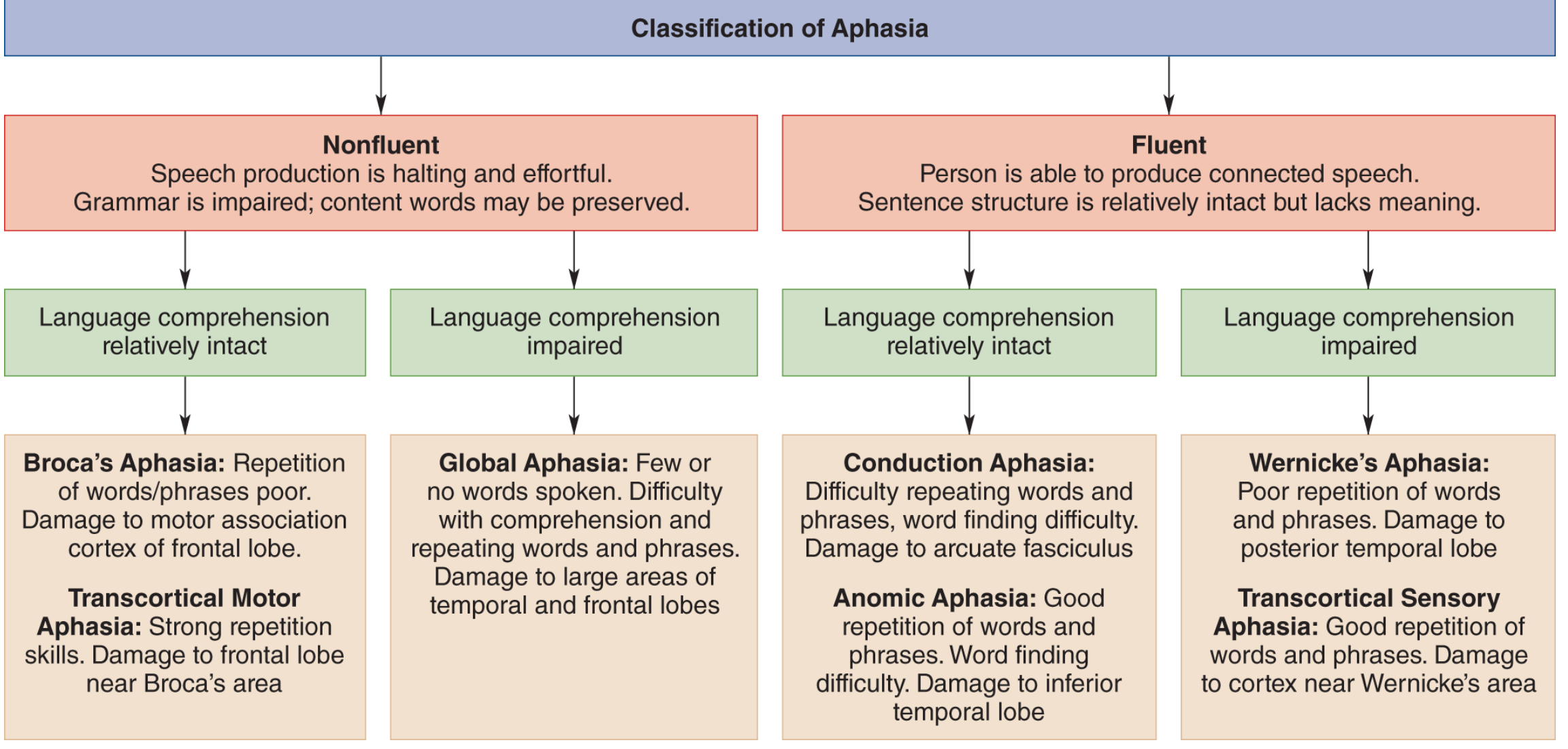
1. Broca Aphasia (Non-fluent, Expressive, Motor)
- Speech: Nonfluent, effortful, telegraphic/agrammatical (omits small grammatical words). Patient may be mute acutely. Example: "wife come hospital."
- Comprehension: Relatively preserved (but mildly impaired for complex syntax)
- Repetition: Impaired
- Naming: Impaired; tip-of-tongue phenomenon common
- Writing: Always impaired, dysmorphic, dysgrammatical
- Associated signs: Right hemiparesis, hemisensory loss, ± limb apraxia
- Lesion: Left inferior frontal gyrus (Brodmann areas 44 & 45 + adjacent subcortical white matter)
2. Wernicke Aphasia (Fluent, Receptive, Sensory)
- Speech: Fluent or even excessive (logorrhea), effortless but empty of meaning. Contains verbal paraphasias, neologisms, and jargon. A foreign listener may notice nothing odd.
- Comprehension: Impaired - sometimes even simple commands fail
- Repetition: Impaired
- Naming: Impaired, often with bizarre paraphasic substitutions
- Writing: Fluent but paragraphic (spelling errors, paraphasias in writing)
- Associated signs: ± Right homonymous hemianopia; no hemiparesis (key distinguishing feature from Broca)
- Lesion: Posterior superior temporal gyrus (Wernicke area, Brodmann area 22)
3. Global Aphasia
- Speech: Mute or severely non-fluent
- Comprehension: Severely impaired
- Repetition: Impaired
- All language modalities are affected - essentially Broca + Wernicke combined
- Associated signs: Dense right hemiplegia, hemisensory loss, hemianopia
- Lesion: Large left perisylvian lesion covering both frontal and temporal regions - most of the left MCA territory
4. Conduction Aphasia
- Speech: Fluent, but with frequent literal (phonemic) paraphasic errors and self-correction attempts
- Comprehension: Relatively preserved
- Repetition: Severely impaired out of proportion to other deficits - the hallmark. Patient who can converse may be unable to repeat a single word.
- Naming: Moderately impaired
- Associated signs: ± Hemisensory loss, ± hemianopia; hemiparesis usually absent
- Lesion: Arcuate fasciculus (disconnects Broca and Wernicke areas) or supramarginal gyrus / insula
5. Transcortical Motor Aphasia
- Speech: Nonfluent, reduced output
- Comprehension: Relatively good
- Repetition: Preserved (key differentiator from Broca aphasia)
- Tendency to echolalia (automatically repeats examiner's words)
- Lesion: Anterior or superior to Broca area (supplementary motor area or its connections), sparing perisylvian cortex
6. Transcortical Sensory Aphasia
- Speech: Fluent, paraphasic
- Comprehension: Impaired (like Wernicke)
- Repetition: Preserved (key differentiator from Wernicke aphasia) - may repeat in an echolalic manner
- Lesion: Posterior to Wernicke area (watershed zone of temporal-parietal cortex)
7. Anomic Aphasia (Nominal / Amnesic Aphasia)
- Speech: Fluent; only deficit is word-finding difficulty (anomia) with circumlocutions
- Comprehension: Normal
- Repetition: Normal
- Isolated loss of naming ability; other language functions relatively spared
- Often the residual syndrome after partial recovery from other aphasia types
- Lesion: Various locations; typically angular gyrus, inferior temporal lobe, or diffuse
8. Pure Word Deafness (Auditory Verbal Agnosia)
- Isolated inability to comprehend spoken language; speech, reading, and writing are intact or near normal
- Patient hears sounds but cannot decode spoken words
- Lesion: Bilateral (or left-sided) middle superior temporal gyrus - disconnection of Wernicke area from bilateral primary auditory cortex
9. Pure Word Blindness (Alexia without Agraphia)
- Unable to read despite normal speech, comprehension, repetition, and writing
- Can write but cannot read their own writing
- Lesion: Left calcarine cortex + splenium of corpus callosum (disconnects right visual cortex from left language areas)
10. Aphemia (Pure Word Mutism)
- Transient muteness with preserved writing
- Some argue it is not a true aphasia since language (writing) is intact
- Lesion: Isolated small lesion in or near Broca area
Summary Table
| Type | Fluency | Comprehension | Repetition | Lesion |
|---|---|---|---|---|
| Broca | Nonfluent | Relatively intact | Impaired | Inferior frontal (L) |
| Wernicke | Fluent | Impaired | Impaired | Superior temporal (L) |
| Global | Nonfluent | Impaired | Impaired | Large perisylvian (L) |
| Conduction | Fluent | Relatively intact | Severely impaired | Arcuate fasciculus |
| Transcortical Motor | Nonfluent | Good | Preserved | Anterior to Broca |
| Transcortical Sensory | Fluent | Impaired | Preserved | Posterior to Wernicke |
| Anomic | Fluent | Normal | Normal | Inferior temporal / angular gyrus |
| Pure Word Deafness | Normal/mild | Impaired (auditory) | Impaired | Bilateral superior temporal |
| Pure Word Blindness | Normal | Normal | Normal | Occipital + corpus callosum |
| Aphemia | Mute → recovery | Normal | - | Near Broca area |
Quick Clinical Memory Aid
- Preserved repetition = transcortical aphasia (motor or sensory type) - the perisylvian arc is intact
- Non-fluent + good comprehension = Broca (anterior lesion)
- Fluent + poor comprehension = Wernicke (posterior lesion)
- Fluent + good comprehension + poor repetition = Conduction
- Everything impaired = Global
Sources: Bradley and Daroff's Neurology in Clinical Practice, Ch. 13; Adams and Victor's Principles of Neurology, 12th Ed., Ch. 22; Neuroscience: Exploring the Brain, 5th Ed., Ch. 20
This is a shared conversation. Sign in to Orris to start your own chat.