analyse_media
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have all the information needed to provide comprehensive answers to all three questions. Here is the complete answer:
Answers to the Three Anatomy Questions
Question 1: Uterine Anomalies - What are these anomalies? Explain the cause.
The Anomalies Shown (Mullerian Duct Anomalies)
The six diagrams depict the spectrum of congenital uterine anomalies arising from failure of proper Mullerian (paramesonephric) duct development:
| Diagram | Name | Description |
|---|---|---|
| Normal | Normal uterus | Single cavity, single cervix, single vagina |
| Subseptate | Subseptate/arcuate uterus | Partial internal septum; shallow fundal indentation; mildest anomaly |
| Septate | Septate uterus | Complete internal septum dividing the cavity, single cervix |
| Unicornuate | Unicornuate uterus | Only one Mullerian duct developed; single horn with one tube/ovary |
| Bicornuate | Bicornuate uterus | Two uterine horns with a fundal cleft, single cervix |
| Didelphys | Uterus didelphys | Complete duplication - two uterine horns AND two cervices |
Cause / Embryological Basis
During female embryonic development, the paired paramesonephric (Mullerian) ducts elongate, migrate toward each other, and fuse in the midline. This is followed by resorption of the intervening septum to form the upper vagina, cervix, uterus, and fallopian tubes - this process is complete by week 20 of gestation.
Failure at different stages produces different anomalies:
- Failure of fusion of the two Mullerian ducts → uterus didelphys or bicornuate uterus
- Failure of septal resorption after fusion → septate uterus (the most common anomaly associated with pregnancy loss)
- Failure of one duct to develop entirely → unicornuate uterus
- Partial fusion defects → arcuate or subseptate forms
Important associated anomaly: Because the paramesonephric ducts develop in close proximity to the mesonephric (Wolffian) system, renal anomalies coexist in ~30% of women with Mullerian anomalies (e.g., absent kidney on the same side). Urologic imaging should always be performed when a Mullerian anomaly is diagnosed.
- Berek & Novak's Gynecology, p. 2064; Creasy & Resnik's Maternal-Fetal Medicine
Question 2: Cardiac Anomaly - What is it? Name the features.
Diagnosis: Tetralogy of Fallot (ToF)
This is the most common cyanotic congenital heart disease.
The Four Features (numbered 1-4 in the diagram):
| Number | Feature | Explanation |
|---|---|---|
| 1 | Ventricular Septal Defect (VSD) | Opening in the interventricular septum allowing shunting of deoxygenated blood |
| 2 | Right Ventricular Hypertrophy | Compensatory thickening of the RV wall due to increased pressure from outflow obstruction |
| 3 | Overriding (Dextropositioned) Aorta | Aorta straddles the VSD, receiving blood from both ventricles |
| 4 | Pulmonary Stenosis | Obstruction of the right ventricular outflow tract (infundibular or valvular) |
Cause / Embryology
Tetralogy results from unequal division of the truncus arteriosus during development - the pulmonary trunk is stenotic. This single developmental error causes all four defects simultaneously (the "tetralogy" is really one morphological defect with four consequences).
Hemodynamic consequence: The pulmonary stenosis creates high right-sided pressure, causing right-to-left shunting through the VSD - deoxygenated blood bypasses the lungs and enters the systemic circulation, producing cyanosis ("blue baby"). Cyanosis is not always present at birth; mild cases are called "pink tets."
- Moore's Clinically Oriented Anatomy / The Developing Human, per embryology textbook
Question 3: Clinical Condition - What is it? Explain the reason.
Diagnosis: Hydrocephalus
The left image shows a normal infant for comparison. The right image shows an infant with a dramatically enlarged, dome-shaped cranium - the classic presentation of hydrocephalus in a neonate.
The "setting sun" sign (eyes deviated downward) is a hallmark clinical feature from raised intracranial pressure.
Definition
Hydrocephalus is a dilation of the cerebral ventricular system due to:
- Obstruction to CSF flow (most common)
- Overproduction of CSF (rare - choroid plexus tumors)
- Failure of CSF reabsorption
Normal CSF Pathway (how to explain obstruction)
CSF is secreted by the choroid plexus in the lateral, 3rd, and 4th ventricles. It flows:
Lateral ventricles → (Foramina of Monro) → 3rd Ventricle → (Cerebral Aqueduct of Sylvius) → 4th Ventricle → (Foramen of Magendie + Foramina of Luschka) → Subarachnoid space → absorbed at arachnoid granulations in dural venous sinuses
Why the head enlarges in infants
In infants, the cranial sutures are not yet fused. When CSF accumulates and ventricular pressure rises, the brain and skull expand outward - leading to the dramatic macrocephaly seen in the images. (In adults with fused sutures, the same obstruction would cause raised ICP without skull expansion.)
Common causes in neonates/children
-
Congenital aqueductal stenosis (stenosis of the Aqueduct of Sylvius) - most common congenital cause
-
Arnold-Chiari malformation with obstruction at the foramina
-
Post-hemorrhagic (intraventricular hemorrhage in premature infants)
-
Tumors obstructing the ventricular pathway
-
Meningitis scarring blocking arachnoid granulations
-
Gray's Anatomy for Students; Guyton and Hall Textbook of Medical Physiology
analyse_media
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
I have all the content needed. Here is the complete answer:
Answers to the Three Anatomy Questions (Pages 10-12/27)
Question 1 (Top of image): Cardiac Anomaly - What is it? Explain the reason.
This question (carried over from the previous page) refers to Tetralogy of Fallot (ToF) - already covered in detail in my previous answer. For completeness:
The cardiac anomaly is Tetralogy of Fallot.
Four features:
- Pulmonary stenosis - obstruction of right ventricular outflow
- Ventricular Septal Defect (VSD) - opening in the interventricular septum
- Overriding aorta - aorta straddles the VSD, receiving blood from both ventricles
- Right ventricular hypertrophy - compensatory thickening due to outflow obstruction
Cause: Unequal division of the truncus arteriosus during embryological development causes the pulmonary trunk to be stenotic. This single defect produces all four components simultaneously. The result is a right-to-left shunt causing cyanosis ("blue baby").
Question 2 (Middle - rotated): Cleft Lip and Cleft Palate
Identification
The two images show:
- Left (Image A): Unilateral cleft lip - a cleft/gap in the upper lip
- Right: Cleft palate - a wide fissure through the hard palate exposing the oral-nasal communication
Cause / Embryological Basis
The face forms from the fusion of five embryonic facial processes during weeks 4-8 of gestation:
- One frontonasal process (gives medial and lateral nasal processes)
- Two maxillary processes (paired, from 1st pharyngeal arch)
- Two mandibular processes (paired, from 1st pharyngeal arch)
Cleft lip results from failure of fusion of the medial nasal segment with the ipsilateral maxillary swelling (process). This normally occurs around week 6-7.
Cleft palate results from failure of the lateral palatine shelves to fuse with each other in the midline (secondary palate), or failure to fuse with the nasal septum/primary palate. This normally occurs around weeks 8-12.
The two defects can occur together or independently:
- Cleft lip alone (primary palate defect)
- Cleft palate alone (secondary palate defect - failure of palatine shelf elevation and fusion)
- Cleft lip + cleft palate (both processes fail; more severe cleft lip increases likelihood of palate involvement)
Etiology is multifactorial - genetic predisposition combined with environmental factors (teratogens, maternal folate deficiency, alcohol, anticonvulsants such as phenytoin, maternal smoking). Incidence is approximately 1/1,000 live births.
- Creasy & Resnik's Maternal-Fetal Medicine; Thompson & Thompson Genetics and Genomics in Medicine
Question 3 (Bottom - rotated): Identify the Clinical Condition and Explain the Underlying Cause
Clinical Condition: Congenital Hydrocephalus
The infant shows the classic features:
- Markedly enlarged, dome-shaped cranium (macrocephaly)
- Prominent, bulging forehead (frontal bossing)
- Stretched, thinned scalp with visible superficial veins
- "Setting-sun sign" - eyes deviated downward with visible sclera above the iris (due to pressure on the superior colliculus / Parinaud's phenomenon)
Underlying Cause
Hydrocephalus = abnormal accumulation of CSF within the cerebral ventricles, causing ventricular dilation and raised intracranial pressure.
CSF Pathway (normal):
Choroid plexus (lateral ventricles) → Foramina of Monro → 3rd ventricle → Aqueduct of Sylvius → 4th ventricle → Foramen of Magendie + Foramina of Luschka → Subarachnoid space → Absorbed at arachnoid granulations
Mechanisms of hydrocephalus:
- Obstruction to CSF flow (most common) - e.g., congenital stenosis of the Aqueduct of Sylvius (most common congenital cause), Arnold-Chiari malformation blocking the foramina of exit
- Impaired CSF reabsorption - e.g., scarring of arachnoid granulations from hemorrhage or meningitis
- CSF overproduction - rare; choroid plexus papilloma
Why the head enlarges in infants specifically: The cranial sutures are not yet fused in neonates and infants. Rising ventricular pressure pushes the ventricles outward, expanding the brain, which then forces the unfused skull bones apart - producing the dramatic macrocephaly visible in the image. In adults with fused sutures, the same process would cause life-threatening raised ICP without cranial enlargement.
UMN vs LMN Facial Palsy Diagram (from the textbook):
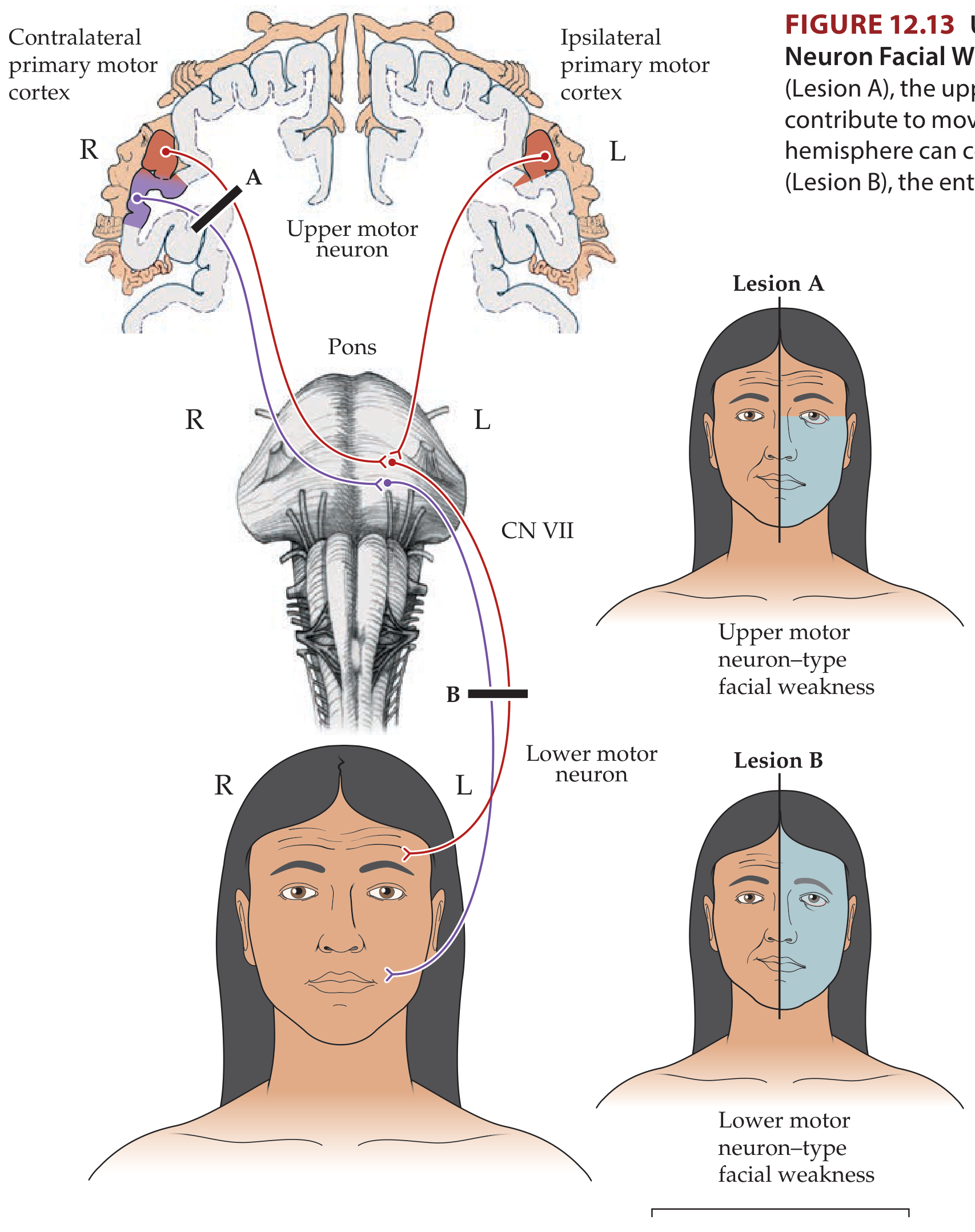
(This diagram is relevant to the first image on this page - Bell's palsy is a lower motor neuron lesion affecting the entire face including the forehead, distinguishing it from a stroke or other UMN lesion which spares the forehead.)
- Neuroanatomy through Clinical Cases, 3rd Edition; Gray's Anatomy for Students
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have everything needed. Here are the complete answers for all four questions.
Answers to the Four Anatomy Questions (Pages 14-16/27)
Question 1 (Slide 1 - rotated): Splenomegaly
Clinical Condition: Splenomegaly (Enlarged Spleen)
The image shows a visible left upper quadrant / hypochondriac bulge in the abdomen - the classic presentation of a massively enlarged spleen extending below the costal margin.
Defensive (Protective) Mechanisms of the Spleen
The spleen has four main defensive/protective functions:
1. Filtration (Red Pulp function)
The spleen filters blood through an "open circulation" system - blood trickles through reticuloendothelial cells (macrophages) in the red pulp. This removes:
- Senescent (old >120 days) red blood cells that have lost their plasticity
- Abnormal RBCs with inclusions - Howell-Jolly bodies (nuclear remnants), Heinz bodies (denatured Hb), Pappenheimer bodies (iron granules)
- Abnormally shaped cells (sickle cells, spherocytes, target cells)
- Blood-borne pathogens, parasites, and cellular debris
- The plasma is directed to lymphoid tissue where antigens stimulate antibody production
2. Immune Surveillance (White Pulp function)
- The white pulp contains the Periarteriolar Lymphoid Sheath (PALS) - T cells surrounding the central artery - and lymphoid follicles (B cells)
- Responds to blood-borne antigens by producing IgM antibodies (primary immune response)
- Produces opsonins (tuftsin and properdin) that enhance phagocytosis
- This is why asplenic patients are at high risk of overwhelming infections by encapsulated bacteria (Streptococcus pneumoniae, Haemophilus influenzae, Neisseria meningitidis)
3. Platelet Reservoir
- Normally one-third of all platelets are stored in the spleen
- In splenomegaly, up to 80% of platelets can be sequestered → thrombocytopenia
4. Fetal Hematopoiesis
- Between weeks 3-5 of fetal life, the spleen produces red and white blood cells (extramedullary hematopoiesis)
- This function can be reactivated in pathological states (myelodysplasia, thalassemia)
Common causes of splenomegaly: infections (malaria, EBV/mononucleosis), haematological malignancies (leukaemia, lymphoma), portal hypertension, haemolytic anaemias, autoimmune diseases.
- Sabiston Textbook of Surgery, pp. 1470-1471
Question 2 (Slide 2 - rotated): Paranasal Air Sinuses
Name the Paranasal Air Sinuses
There are four paired paranasal sinuses (all lined by respiratory epithelium, continuous with the nasal mucosa):
| Sinus | Location |
|---|---|
| Frontal sinuses | Within the frontal bone above the orbits |
| Maxillary sinuses | Largest sinuses; within the maxillary bone (cheeks), below the orbits |
| Ethmoidal sinuses | Honeycomb-like labyrinth between orbits and nasal cavity; divided into anterior, middle, and posterior groups |
| Sphenoidal sinuses | Within the sphenoid bone posteriorly; adjacent to optic nerves, carotid arteries, and sella turcica |
Where They Open in the Lateral Wall of the Nose
| Sinus | Opening Site on Lateral Wall |
|---|---|
| Frontal sinus | Middle nasal meatus - drains via the frontonasal duct → ethmoidal infundibulum → anterior end of semilunar hiatus |
| Maxillary sinus | Middle nasal meatus - opens into the semilunar hiatus (near the roof of the sinus - clinically relevant: poor drainage when upright) |
| Anterior ethmoidal cells | Middle nasal meatus - drain into the ethmoidal infundibulum or frontonasal duct |
| Middle ethmoidal cells | Open onto or just above the ethmoidal bulla (in the middle meatus) |
| Posterior ethmoidal cells | Superior nasal meatus - via the sphenoethmoidal recess |
| Sphenoidal sinus | Does NOT drain into a meatus on the lateral wall; opens onto the sloping posterior roof of the nasal cavity (sphenoethmoidal recess) |
| Nasolacrimal duct (not a sinus, but related) | Inferior nasal meatus - under the anterior lip of the inferior concha |
Memory aid: "Most sinuses → Middle meatus; Posterior ethmoid → Superior meatus; Sphenoid → Roof"
- Gray's Anatomy for Students, p. 1218-1219; Sabiston Textbook of Surgery, p. 1338
Question 3 (Slide 3): Identify the Clinical Condition
Clinical Condition: Anencephaly
The photograph shows a newborn with complete absence of the cerebral hemispheres, vault of the skull, and overlying skin - the classic appearance of anencephaly.
Underlying Cause
Anencephaly is a neural tube defect (NTD) - the most severe form.
Embryological basis: The neural tube normally closes between days 22-28 post-fertilization. Anencephaly results from failure of closure of the rostral (cranial) neuropore (the head end of the neural tube) during week 4 of development. Without closure:
- The forebrain fails to develop (absent cerebral hemispheres)
- The overlying meninges, skull vault (cranial bones), and scalp are all absent
- The brain tissue that does form remains exposed and degenerates
Key features:
- ~2/3 of affected infants are female
- Incompatible with sustained life - most are stillborn; live-born infants survive only hours
- Associated with polyhydramnios (fetus cannot swallow amniotic fluid normally due to lack of brain control)
Causes - multifactorial:
- Folic acid deficiency - the single greatest environmental factor. Maternal serum folate <200 μg/L significantly increases NTD risk. Supplementation with 400-800 μg/day before conception and through the first 2 months reduces NTD incidence by >75%
- MTHFR gene variant - a common missense variant makes methylenetetrahydrofolate reductase unstable, impairing folate recycling; homozygotes are at doubled risk
- Teratogens - valproic acid, methotrexate, some anticonvulsants
- Chromosomal abnormalities and single-gene defects (minority)
- Hyperthermia, maternal diabetes
- Thompson & Thompson Genetics and Genomics in Medicine, 9th ed.; Medical Physiology
Question 4 (Slide 4): Lumbar Puncture Diagram
What the Diagram Shows
This is an illustration of a lumbar puncture (spinal tap) procedure, showing:
- Patient in lateral decubitus (fetal) position - knees drawn to chest, spine fully flexed to widen the interspinous spaces
- A spinal needle being inserted in the lumbar region (between L3-L4 or L4-L5)
- Zoomed inset showing the needle passing between two vertebrae into the subarachnoid space
Anatomical Basis
Why the lumbar region (L3/4 or L4/5)?
- The spinal cord ends at L1-L2 (conus medullaris) in adults
- Below this, only the cauda equina (nerve roots floating in CSF) remains - these move aside rather than being pierced by the needle, making it safe
- The dural sac continues to S2
Layers the needle passes through (superficial to deep):
- Skin and subcutaneous fat
- Supraspinous ligament
- Interspinous ligament
- Ligamentum flavum
- Epidural space
- Dura mater
- Arachnoid mater
- Subarachnoid space → CSF is obtained here
Clinical uses of lumbar puncture:
- Diagnosis of meningitis, encephalitis, subarachnoid hemorrhage
- Measurement of CSF pressure
- Administration of spinal anaesthesia or intrathecal drugs
- CSF sampling for multiple sclerosis, Guillain-Barré syndrome
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the information needed. Here are comprehensive answers to all five clinical conditions shown.
Answers to the Hand/Upper Limb Anatomy Questions
Slide 1 (Top): Palmar Thickening with Flexion Contracture
Clinical Condition: Dupuytren's Contracture
The image shows thickening and cord-like bands of the palmar fascia pulling the ring and little fingers into fixed flexion at the MCP and PIP joints, preventing full extension.
Key features:
- Fibroproliferative disease of the palmar fascia (not a nerve injury)
- Most commonly affects the 4th (ring) and 5th (little) fingers
- Progressive nodules develop first in the palm, then cords form that contract the fingers
- More common in males, those of Northern European descent, diabetics, alcoholics, epileptics
Pathophysiology: Myofibroblast proliferation in the palmar aponeurosis → collagen deposition → contracture. Not directly caused by nerve damage, but severe cases can compress digital nerves.
Slide 2: Wrist Drop
1. Clinical Condition: Wrist Drop (Radial Nerve Palsy)
The hand hangs limply with inability to extend the wrist or fingers - the hallmark of radial nerve injury.
2a. Nerve Involved: Radial Nerve (CN - Brachial Plexus)
Motor deficits from radial nerve injury:
- Wrist drop - inability to extend the wrist (extensor carpi radialis longus/brevis, extensor carpi ulnaris are paralysed)
- Loss of extension at all 5 MCP joints
- Loss of extension and abduction of thumb
- At high lesion (spiral groove or above): loss of elbow extension (triceps) too
- Supination weakness
Sensory loss: Dorsum of the hand and first 4 digits (lateral aspect); posterior surface of arm and forearm
Common causes:
- "Saturday night palsy" - compression in the spiral groove of the humerus (arm draped over a chair while asleep/intoxicated)
- Humeral shaft fracture (mid-shaft, at spiral groove)
- Crutch compression in the axilla (high radial palsy)
- Shoulder dislocation
2b. Cord of Brachial Plexus: Posterior Cord
The radial nerve arises from the posterior cord of the brachial plexus (roots C5, C6, C7, C8, T1). The posterior cord also gives off the axillary nerve.
Brachial Plexus summary for the radial nerve:
Roots C5-T1 → Trunks → Divisions → Posterior Cord → Radial Nerve
- Localization in Clinical Neurology, 8th ed.
Slide 3: The Marked Area on the Hand (rotated)
Identify the Marked Area: Anatomical Snuffbox
The red-outlined triangular depression on the dorsolateral (radial) aspect of the wrist at the base of the thumb is the anatomical snuffbox.
Boundaries:
| Border | Structure |
|---|---|
| Radial (lateral) border | Tendons of abductor pollicis longus + extensor pollicis brevis |
| Ulnar (medial) border | Tendon of extensor pollicis longus |
| Floor | Scaphoid and trapezium bones; radial artery passes through it |
| Roof | Skin |
Contents: Radial artery (passing deep to enter the palm), superficial branch of the radial nerve, cephalic vein origin
Which Carpal Bone Injury Can Be Identified in This Area?
Scaphoid fracture
Tenderness on palpation of the anatomical snuffbox following a fall on outstretched hand (FOOSH) is the classic clinical sign of a scaphoid fracture. The scaphoid waist lies directly in the floor of the snuffbox.
Why it matters:
-
The scaphoid has a retrograde blood supply (enters distally); a fracture at the waist can interrupt blood supply to the proximal pole → avascular necrosis if missed/untreated
-
Often missed on initial X-ray; if snuffbox tenderness is present, treat as scaphoid fracture until proven otherwise (CT or MRI)
-
Bailey and Love's Short Practice of Surgery; Campbell's Operative Orthopaedics
Slide 4: Claw Hand Deformity
Clinical Condition: Claw Hand (Ulnar Nerve Palsy - Main en Griffe)
The image shows hyperextension at the MCP joints of the ring and little fingers, with flexion at the PIP and DIP joints - the classic ulnar claw.
Nerve involved: Ulnar Nerve (C8, T1)
Mechanism of claw deformity:
The intrinsic hand muscles (interossei + medial two lumbricals) normally flex the MCP joints and extend the IP joints. When the ulnar nerve is injured:
- Interossei and medial two lumbricals are paralysed
- Extensor digitorum pulls the MCPs into hyperextension (unopposed)
- Flexor digitorum profundus (still intact) pulls the IPs into flexion (unopposed)
- Result: MCP hyperextension + IP flexion = "clawing"
Why only ring and little fingers? The index and middle finger lumbricals are supplied by the median nerve (not ulnar), so they partially compensate and claw less. This is the "ulnar paradox" - a wrist-level (distal) lesion causes more severe clawing than an elbow-level (proximal) lesion, because at the elbow level the FDP (ring and little) is also paralysed, reducing the IP flexion component.
Additional features of ulnar nerve palsy:
- Hypothenar wasting and first dorsal interosseous space wasting
- Froment's sign (positive = flexes thumb IP joint when gripping paper - uses FPL to compensate for paralysed adductor pollicis)
- Sensory loss: ulnar 1.5 fingers (little + ulnar half of ring) and ulnar palm
Common causes: Compression at the cubital tunnel (elbow) - most common; laceration at wrist; Guyon's canal compression at the wrist
Cord of Brachial Plexus: Ulnar nerve arises from the medial cord (roots C8, T1)
- THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
Slide 5 (partially visible): Winged Scapula
Clinical Condition: Winged Scapula
The posterior view of the patient shows the medial border and inferior angle of the scapula protruding outward (posteriorly), like a wing - most pronounced when the patient pushes against a wall or raises the arms.
Nerve Involved: Long Thoracic Nerve (C5, C6, C7)
Muscle paralysed: Serratus anterior
Why this produces winging:
Serratus anterior normally holds the medial border of the scapula flush against the thoracic wall, and protracts the scapula (needed for shoulder elevation above 90°). When paralysed:
- The medial border "wings" away from the chest wall
- The inferior angle points posteriorly and laterally
- Shoulder abduction above 90° is impossible
Common causes of long thoracic nerve injury:
- Axillary lymph node dissection (mastectomy - most common iatrogenic cause; nerve runs down lateral thoracic wall, just deep to skin)
- Stabbing or direct trauma to the lateral chest wall
- Neuralgic amyotrophy (Parsonage-Turner syndrome)
- Carrying heavy loads on the shoulder
- First rib fracture
Origin of long thoracic nerve: Direct branches from C5, C6, C7 nerve roots (not from a cord) - it arises from the roots before they form the trunks of the brachial plexus. This is why it is not protected within the plexus sheath.
- Gray's Anatomy for Students; Fischer's Mastery of Surgery
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
All information gathered. Here are the complete answers.
Answers to the Upper Limb & Lower Limb Anatomy Questions
Image 1 (Top): Posterior Back View with Prominent Scapula
Clinical Condition: Winged Scapula
The medial border and inferior angle of the left scapula project backwards (posteriorly) away from the thoracic wall, appearing like a "wing."
Nerve Injured: Long Thoracic Nerve (of Bell)
- Arises directly from roots C5, C6, C7 (before they form the trunks of the brachial plexus)
- Runs down the lateral thoracic wall on the external surface of the serratus anterior muscle, just deep to the skin - making it vulnerable to injury in axillary surgery
Muscle Involved: Serratus Anterior
- Origin: outer surfaces of ribs 1-8 (digitations)
- Insertion: medial border (costal surface) of the scapula
- Action: protracts the scapula and holds its medial border against the thoracic wall; essential for elevating the arm above 90°
When paralysed: The medial border of the scapula loses its anchorage → wings away from the chest wall. Pushing against a wall accentuates the winging.
Common causes of long thoracic nerve injury:
-
Axillary lymph node dissection (mastectomy) - most common iatrogenic cause
-
Stab wounds to the lateral chest wall
-
Carrying heavy loads on the shoulder
-
Neuralgic amyotrophy (Parsonage-Turner syndrome)
-
Gray's Anatomy for Students
Image 2: Palpation of the Dorsum of the Foot (rotated)
Arterial Pulsation Shown: Dorsalis Pedis Artery
The examiner's fingers are placed just lateral to the extensor hallucis longus tendon on the dorsum of the foot (at the first intermetatarsal space). This is the dorsalis pedis pulse - a continuation of the anterior tibial artery.
How to locate it: The extensor hallucis longus tendon is clearly visible when the patient dorsiflexes the great toe. The dorsalis pedis pulse is felt 1 cm lateral to this tendon.
Other Arteries of the Lower Limb Where Pulsations Can Be Felt:
| Artery | Site of Palpation |
|---|---|
| Femoral artery | Femoral triangle - midway between the anterior superior iliac spine (ASIS) and the pubic tubercle (mid-inguinal point) |
| Popliteal artery | Popliteal fossa - knee flexed to 45°, bimanual compression; fingers deep between gastrocnemius heads against posterior tibia |
| Posterior tibial artery | 2 cm posterior to the medial malleolus |
| Dorsalis pedis artery | Dorsum of foot, lateral to extensor hallucis longus tendon |
(Note: Popliteal pulse is normally the hardest to feel due to deep location)
- Schwartz's Principles of Surgery; S. Das Manual on Clinical Surgery
Image 3: Dropped Foot (rotated)
Clinical Condition: Foot Drop
The foot hangs in fixed plantarflexion (pointing downward), with inability to dorsiflex or evert the foot. The patient would have a high-stepping gait (steppage gait) to clear the floor when walking.
Nerve Involved: Common Peroneal (Fibular) Nerve
This is a branch of the sciatic nerve (L4, L5, S1, S2). It winds around the neck of the fibula - where it is most superficial and vulnerable to injury.
Muscles paralysed (anterior and lateral compartments):
- Tibialis anterior - dorsiflexion of ankle
- Extensor digitorum longus/brevis - toe extension
- Extensor hallucis longus - great toe extension
- Peroneus (fibularis) longus and brevis - eversion of foot
Result: Foot drop + loss of eversion → talipes equinovarus (foot points down and inward)
Sensory loss: Anterior and lateral aspects of the lower leg, dorsum of the foot and toes (except the first web space, which is supplied by the deep peroneal nerve)
Common causes:
- Fracture of the neck of fibula - most common
- Prolonged pressure (crossing legs, plaster cast, prolonged squatting)
- Knee dislocation
- Diabetic neuropathy
- Iatrogenic (knee surgery, hip replacement)
- S. Das Manual on Clinical Surgery
Image 4: Infant with Arm Held at Side in Abnormal Posture
Clinical Condition: Erb-Duchenne Palsy (Erb's Palsy)
The infant holds the arm in the classic "waiter's tip" / "bellman's tip" position:
- Arm adducted and internally rotated at the shoulder
- Forearm extended and pronated
- Wrist flexed
- Fingers relatively spared
Cause: Upper Brachial Plexus Injury - C5 and C6 nerve roots (upper trunk)
In neonates: caused by excessive lateral traction on the head/neck during a difficult delivery (e.g., shoulder dystocia), or downward traction on the shoulder.
In adults: motorcycle accidents (forceful separation of the neck from the shoulder).
Muscles affected (C5, C6 innervated):
| Muscle | Function lost |
|---|---|
| Deltoid | Shoulder abduction |
| Biceps brachii | Elbow flexion, supination |
| Brachialis | Elbow flexion |
| Supraspinatus | Shoulder abduction initiation |
| Infraspinatus | External rotation of shoulder |
| Wrist extensors (partial) | Wrist extension |
Reflexes lost: Biceps reflex (C5, C6), brachioradialis reflex (C5)
The characteristic posture occurs because the UNOPPOSED muscles pull the arm into:
- Internal rotation (subscapularis, pectoralis major - still intact via C5-T1 via median/anterior cord)
- Adduction (pectoralis major, latissimus dorsi)
- Pronation (pronator teres - partially intact)
Contrast with Klumpke's palsy (lower trunk, C8-T1): causes claw hand and intrinsic muscle weakness (the opposite end of the brachial plexus).
Prognosis: Most neonatal Erb's palsies (80-90%) recover fully. Surgical exploration if no recovery by 3-6 months.
- Neuroanatomy through Clinical Cases, 3rd Ed.
Image 5: Prominent Tortuous Leg Veins
Clinical Condition: Varicose Veins
Dilated, tortuous, engorged superficial veins of the lower limb - most prominently along the posteromedial calf and medial thigh (distribution of the great saphenous vein).
Anatomical Basis / Cause: Venous Valve Incompetence
Normal venous drainage of the lower limb:
- Deep veins (femoral, popliteal, tibial) drain the majority of blood
- Superficial veins (great saphenous, small saphenous) drain the skin and subcutaneous tissue
- Perforating veins connect the two systems; their valves only allow flow from superficial → deep
- Valves in all veins prevent retrograde flow when the calf muscle pump contracts
Pathophysiology of varicose veins:
- Valvular incompetence at the sapheno-femoral junction (where the great saphenous vein drains into the femoral vein) is the most common site
- High pressure from the deep system refluxes back into the superficial system
- Raised venous pressure → progressive dilation and tortuosity of superficial veins
- Other incompetent sites: sapheno-popliteal junction (small saphenous) and perforating vein valves
Key sites of valve incompetence:
- Sapheno-femoral junction (great saphenous → femoral vein)
- Perforating veins in the mid-thigh
- Sapheno-popliteal junction (small saphenous → popliteal vein)
Complications if untreated:
- Venous eczema (skin breakdown from chronic high pressure)
- Haemosiderin skin pigmentation (brown staining)
- Lipodermatosclerosis
- Venous ulcers (gaiter area, medial malleolus) - most serious complication
Risk factors: female sex, pregnancy, prolonged standing, obesity, family history, previous DVT (destroys valves during recanalization)
- Gray's Anatomy for Students; Pfenninger and Fowler's Procedures for Primary Care
analyse_media
analyse_media
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Excellent - the nerve diagram from Gray's Anatomy is perfect. Here are the complete answers for this final page (27/27).
Answers to the Final Two Anatomy Questions (Page 27/27)
Slide 1: Identify the Bone and Name the Nerves Closely Related to It
The Bone: Humerus
The two specimens shown are the left and right humeri - the single long bone of the arm, articulating proximally with the glenoid fossa of the scapula (glenohumeral joint) and distally with the radius and ulna (elbow joint).
Key anatomical landmarks:
Proximal end:
- Head - articulates with the glenoid cavity
- Anatomical neck - immediately distal to the head
- Greater tubercle (lateral) - insertions of supraspinatus, infraspinatus, teres minor
- Lesser tubercle (anterior) - insertion of subscapularis
- Intertubercular (bicipital) groove - lodges the tendon of the long head of biceps
- Surgical neck - most common site of fracture; the constriction just below the tubercles
Shaft:
- Deltoid tuberosity (lateral mid-shaft) - attachment of deltoid
- Radial (spiral) groove - runs obliquely across the posterior shaft
Distal end:
- Capitulum (lateral) - articulates with head of radius
- Trochlea (medial) - articulates with trochlear notch of ulna
- Medial epicondyle (prominent)
- Lateral epicondyle
- Olecranon fossa (posterior) - receives olecranon in extension
- Coronoid fossa (anterior) - receives coronoid process in flexion
Nerves Closely Related to the Humerus
Three major nerves lie in direct contact with specific parts of the humerus and are endangered by fractures at those sites:
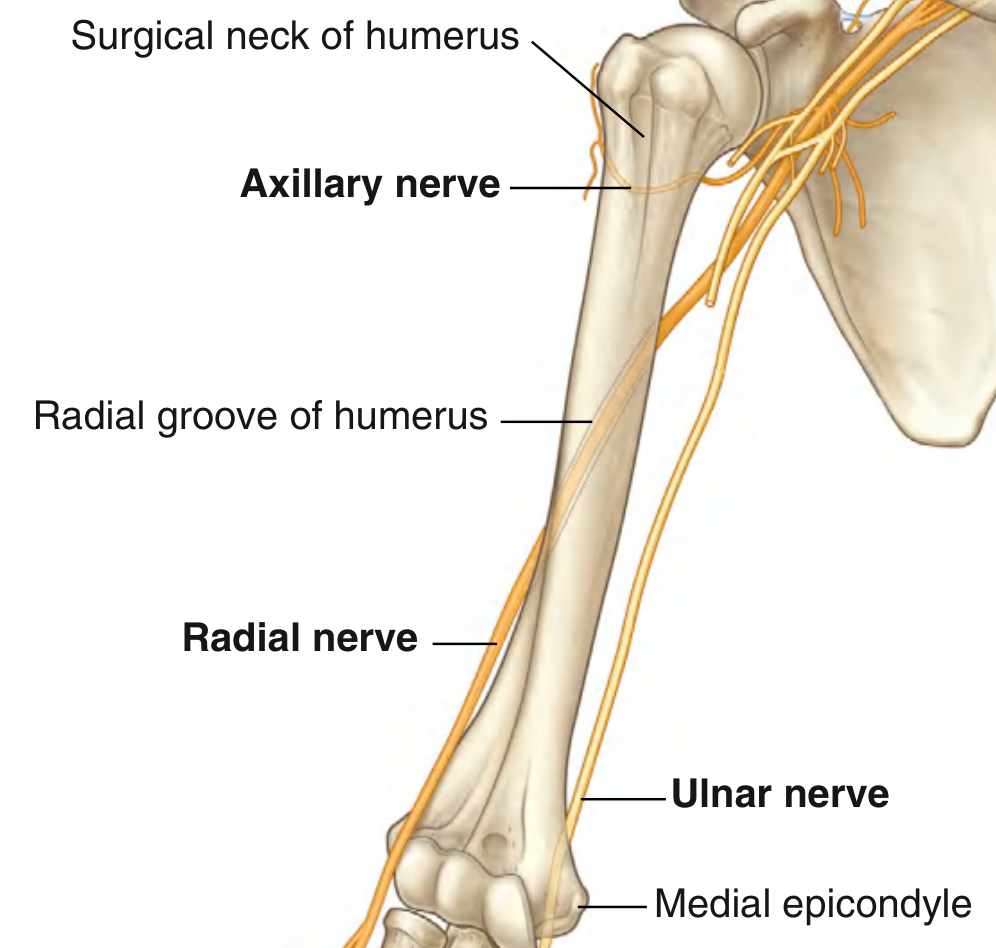
| Nerve | Site of Relation | Fracture Risk | Consequence if Damaged |
|---|---|---|---|
| Axillary nerve (C5, C6) | Winds posteriorly around the surgical neck | Fracture of surgical neck / shoulder dislocation | Paralysis of deltoid (loss of shoulder abduction) + teres minor; sensory loss over "regimental badge" area of lateral shoulder |
| Radial nerve (C5-T1) | Passes diagonally through the radial (spiral) groove on the posterior shaft | Fracture of mid-shaft humerus ("Holstein-Lewis fracture") | Wrist drop + loss of finger extension; sensory loss on dorsum of hand |
| Ulnar nerve (C8, T1) | Passes posteriorly behind the medial epicondyle | Fracture of medial epicondyle; elbow injuries | Claw hand (ring + little); loss of hypothenar, interossei, medial lumbricals; sensory loss ulnar 1.5 fingers |
Mnemonic: "At Surgical neck - Axillary; Radial Groove - Radial; Medial Epicondyle - ulNar"
- Gray's Anatomy for Students, p. 818
Slide 2: X-ray - Explain the Radiological Finding and Deformity in the Hand
Diagnosis: Colles' Fracture
Radiological Findings (X-ray Analysis)
Two views are shown:
PA (Posteroanterior) view:
- Transverse fracture of the distal radius, approximately 2 cm proximal to the radiocarpal joint
- Lateral (radial) displacement of the distal fragment (arrow pointing laterally)
- Radial shortening relative to the ulna
- Often associated with ulnar styloid fracture
- May show intraarticular extension into the radiocarpal or radioulnar joint
Lateral view:
- Dorsal displacement of the distal radial fragment (arrow pointing dorsally toward "dorsum of hand")
- Dorsal angulation - loss of the normal volar (palmar) tilt of the distal radial articular surface
- The distal fragment tilts backwards relative to the shaft
Clinical Deformity: "Dinner Fork" Deformity
The clinical photograph shows a lateral view of the wrist with:
- A dorsal hump/prominence at the wrist (the dorsally displaced distal fragment)
- A corresponding depression on the volar (palmar) side
- The appearance resembles a dinner fork seen from the side - hence the name
Mechanism of Injury
Fall on an outstretched hand (FOOSH) with the wrist in dorsiflexion. The ground reaction force drives the distal radius dorsally and radially. Most common in:
- Postmenopausal women with osteoporosis (most classic demographic)
- After age 40
Key Displacements in Colles' Fracture (the "DROLL" mnemonic):
- Dorsal displacement of distal fragment
- Radial displacement
- Osteoporosis (common background)
- Loss of volar tilt
- Lengthening lost (radial shortening)
Complications
- Median nerve injury - most common nerve complication (compressed in the carpal tunnel by displaced fragment → acute carpal tunnel syndrome)
- Malunion → persistent deformity
- Extensor pollicis longus tendon rupture (late)
- Complex regional pain syndrome (Sudeck's atrophy)
- Radiocarpal/radioulnar joint stiffness
Note: Always test median nerve function (sensation over radial 3.5 fingers, thumb opposition) before AND after fracture reduction.
- Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.