All about moxifloxacin for pharma short note
moxifloxacin pharmacology mechanism spectrum uses adverse effects clinical notes
Moxifloxacin - Short Note (Pharmacology)
1. Introduction and Classification
2. Mechanism of Action
- DNA gyrase (Topoisomerase II) - responsible for introducing negative supercoils during DNA replication
- Topoisomerase IV - responsible for decatenation of daughter chromosomes after replication
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 1163
3. Antibacterial Spectrum
| Category | Organisms |
|---|---|
| Gram-positive | S. pneumoniae (excellent), S. aureus (including MSSA), streptococci - MICs 1-2 dilutions lower than levofloxacin |
| Gram-negative | H. influenzae, M. catarrhalis, Enterobacteriaceae - note: poor activity against Pseudomonas aeruginosa |
| Atypical / Intracellular | Chlamydia, Mycoplasma, Legionella, Brucella |
| Anaerobes | Bacteroides fragilis and other intestinal anaerobes (unique among fluoroquinolones) |
| Mycobacteria | M. tuberculosis, M. kansasii, M. fortuitum, M. avium complex |
- Goodman & Gilman's, p. 1162; Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 1318
4. Pharmacokinetics
| Parameter | Details |
|---|---|
| Bioavailability | ~90% oral; IV and oral doses are equivalent |
| Tmax | 1-3 hours after oral dose |
| t½ | ~12 hours - allows once-daily dosing |
| Usual dose | 400 mg once daily (oral or IV) |
| Volume of distribution | Large; penetrates well into lung, prostate, macrophages, bile |
| Metabolism | Hepatic - sulfation and glucuronidation (NOT cytochrome P450) - hence fewer drug interactions |
| Excretion | Mixed: hepatobiliary + renal; <25% excreted unchanged in urine |
| Renal dose adjustment | NOT required (unlike other fluoroquinolones) |
| Hepatic impairment | Use with caution; no specific contraindication for mild-moderate |
- Goodman & Gilman's, p. 1162-1163
5. Therapeutic Uses
- Community-acquired pneumonia (CAP) - first-line option; covers pneumococcus, atypicals, H. influenzae
- Acute bacterial exacerbation of chronic bronchitis (AECB)
- Acute bacterial sinusitis
- Moxifloxacin alone (monotherapy) can be used for intra-abdominal infections due to its anaerobic coverage - unlike other fluoroquinolones that need metronidazole added
- Complicated skin infections, diabetic foot infections (broader spectrum useful here)
- Second-line drug in multidrug-resistant TB (MDR-TB) regimens
- Active against M. kansasii, M. fortuitum, M. avium complex (with other agents)
- Moxifloxacin 0.5% eye drops (Vigamox) - bacterial conjunctivitis
-
UTIs (inadequate urinary levels)
-
Pseudomonas infections
-
Gonorrhea (widespread resistance)
-
Goodman & Gilman's, p. 1164-1165
6. Adverse Effects
Common
- GI: Nausea, vomiting, abdominal discomfort, diarrhea (3-17%); risk of C. difficile colitis
- CNS: Headache, dizziness, insomnia, anxiety (1-11%)
Serious (Fluoroquinolone class effects)
| Adverse Effect | Notes |
|---|---|
| QT prolongation / Torsades de Pointes | Moxifloxacin carries the HIGHEST risk among fluoroquinolones for QTc prolongation. Avoid in patients with known long QT, hypokalemia, hypomagnesemia, and those on class IA/III antiarrhythmics (quinidine, procainamide, amiodarone, sotalol) |
| Tendinitis / Tendon rupture | Especially Achilles tendon; risk increased in >60 years, corticosteroid users, and solid-organ transplant recipients |
| Peripheral neuropathy | Can be irreversible in some cases |
| CNS effects | Rare: hallucinations, delirium, seizures (risk increased with theophylline or NSAIDs co-administration) |
| Photosensitivity | Advise sun protection; less phototoxic than older quinolones |
| Hepatotoxicity | Rare but reported |
- Goodman & Gilman's, p. 1163-1164
7. Drug Interactions
| Interacting Drug/Substance | Mechanism & Effect |
|---|---|
| Antacids, iron, calcium, sucralfate, zinc | Chelation with divalent/trivalent cations - reduces bioavailability; separate by at least 2 hours |
| Class IA antiarrhythmics (quinidine, procainamide) | Additive QT prolongation - avoid |
| Class III antiarrhythmics (amiodarone, sotalol) | Additive QT prolongation - avoid |
| NSAIDs | Displace GABA from receptors, augmenting CNS/seizure adverse effects |
| Warfarin | May potentiate anticoagulant effect - monitor INR |
| Theophylline | Moxifloxacin (unlike ciprofloxacin) does NOT significantly inhibit CYP1A2, so theophylline interaction is minimal, but caution still advised for CNS effects |
8. Contraindications
- Known hypersensitivity to fluoroquinolones
- QTc prolongation or congenital long QT syndrome
- Uncorrected hypokalemia or hypomagnesemia
- Concurrent use of class IA or III antiarrhythmics
- Pregnancy - avoid (cartilage damage risk in animal studies; limited human data)
- Children and adolescents - generally avoided (risk of arthropathy/cartilage damage), unless no alternatives exist
- NOT for UTIs (inadequate urinary concentration)
9. Bacterial Resistance
- Chromosomal mutations in gyrA/gyrB (DNA gyrase) and parC/parE (Topo IV) genes - reduced binding
- Efflux pump upregulation - active drug expulsion
- Porin downregulation - reduced drug entry (especially gram-negatives)
- Plasmid-mediated resistance - rare; Qnr proteins protect topoisomerases; enzymatic drug modification
10. Comparison with Other Fluoroquinolones (Quick Reference)
| Feature | Ciprofloxacin | Levofloxacin | Moxifloxacin |
|---|---|---|---|
| Generation | 2nd | 3rd | 4th |
| Pseudomonas cover | ✓✓ | ✓ | ✗ |
| Pneumococcal cover | + | ++ | +++ |
| Anaerobic cover | ✗ | ✗ | ✓ (B. fragilis) |
| Urinary use | ✓ | ✓ | ✗ |
| QT risk | Lowest | Low | Highest |
| Dosing | BD | OD | OD |
| Renal dose adj. | Required | Required | Not required |
11. Key Exam Points (Mnemonics)
- MOXY = M-ycobacteria, O-nce daily, X-tra anaerobic cover, Y-ou can't use for UTI
- Among fluoroquinolones, moxifloxacin has: BEST gram-positive + anaerobic coverage, WORST pseudomonal coverage, HIGHEST QT risk
- Metabolism via sulfation/glucuronidation (not CYP) = no dose adjustment in renal impairment, fewer drug interactions
- Brand name: Avelox (systemic), Vigamox (ophthalmic)
Give a short note on flourorquinolones
fluoroquinolones pharmacology classification generations mechanism spectrum adverse effects short note
Fluoroquinolones - Short Note (Pharmacology)
1. Introduction and History
2. Classification by Generations
| Generation | Drugs | Spectrum |
|---|---|---|
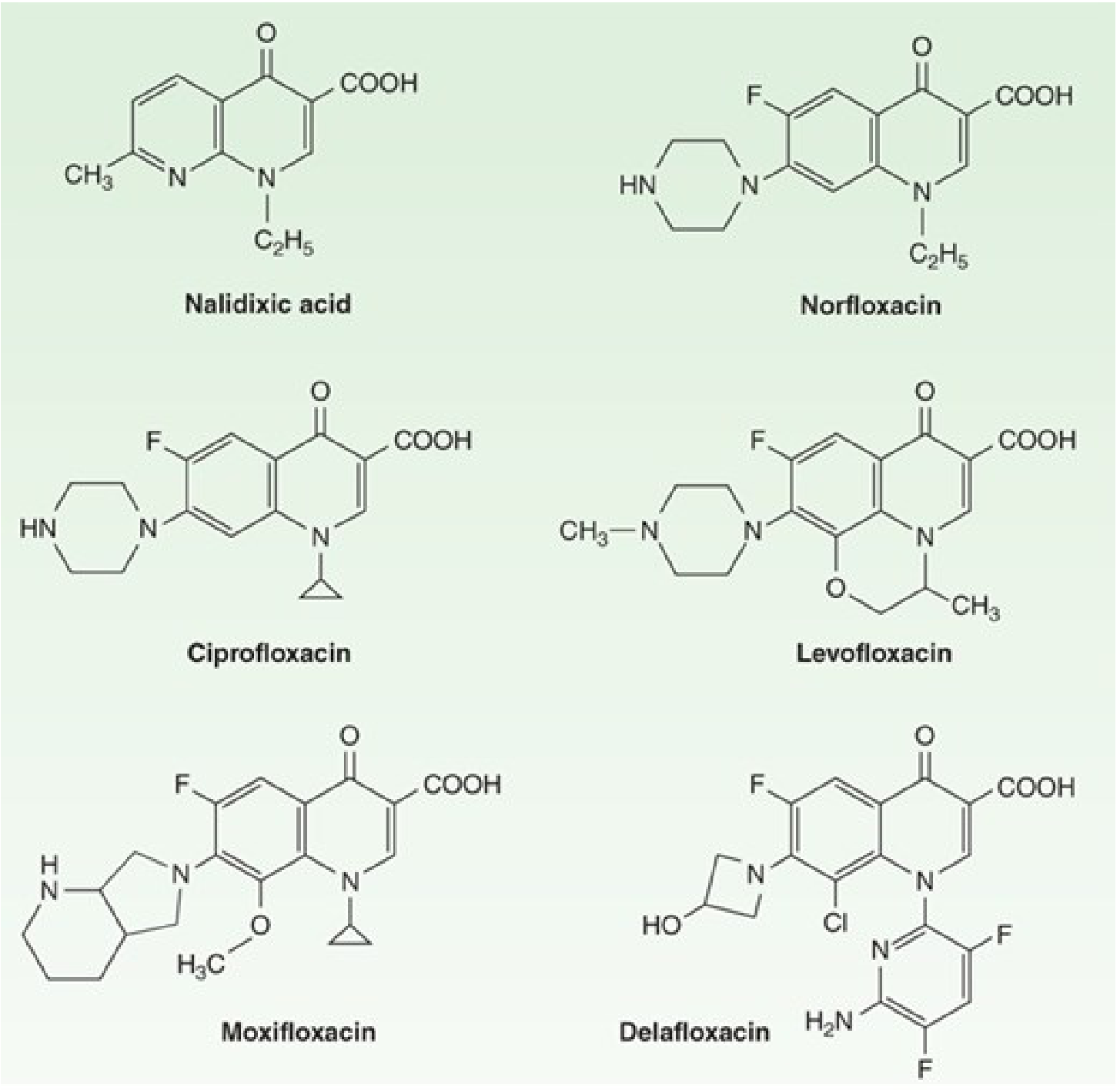
| 1st | Nalidixic acid, cinoxacin | Gram-negative only; limited to UTIs; not systemic |
| 2nd | Norfloxacin, ciprofloxacin, ofloxacin, enoxacin | Broad gram-negative; ciprofloxacin with anti-pseudomonal activity; limited gram-positive |
| 3rd | Levofloxacin, sparfloxacin | Enhanced gram-positive (esp. pneumococci); maintains gram-negative |
| 4th | Moxifloxacin, gemifloxacin, delafloxacin | Best gram-positive + anaerobic; reduced/no anti-pseudomonal; delafloxacin active at acidic pH |
Note: Many early fluoroquinolones were withdrawn post-marketing due to toxicity - lomefloxacin and sparfloxacin (QTc prolongation, phototoxicity), gatifloxacin (dysglycemia), temafloxacin (immune hemolytic anemia), trovafloxacin (hepatotoxicity), grepafloxacin (cardiotoxicity).
- Goodman & Gilman's, p. 1161
3. Mechanism of Action
- Introduces negative supercoils into DNA to relieve positive supercoiling during replication and transcription
- Quinolones inhibit the nicking-closing (strand passage) activity at concentrations of 0.1-10 μg/mL
- Separates interlinked (catenated) daughter chromosomes after DNA replication
- Inhibition blocks cell division
- Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 1303-1304; Goodman & Gilman's, p. 1161
4. Antibacterial Spectrum
| Category | Coverage | Key Points |
|---|---|---|
| Gram-negative aerobes | Excellent | E. coli, Klebsiella, Proteus, Enterobacter, Salmonella, Shigella, Campylobacter, H. influenzae, M. catarrhalis |
| Pseudomonas aeruginosa | Ciprofloxacin > levofloxacin (moxifloxacin is poor) | Anti-pseudomonal activity limited to 2nd/3rd generation |
| Gram-positive aerobes | Variable | 4th gen best; all less active against MRSA; activity against pneumococci best with levofloxacin/moxifloxacin/gemifloxacin |
| Intracellular bacteria | Good | Chlamydia, Mycoplasma, Legionella, Brucella |
| Mycobacteria | Good | M. tuberculosis, M. kansasii, M. fortuitum; used in MDR-TB regimens |
| Anaerobes | Moxifloxacin only | B. fragilis; other FQs are poor against anaerobes |
| NOT active against | - | MRSA (generally), Enterococcus, Treponema pallidum, most anaerobes (except moxifloxacin) |
5. Pharmacokinetics
| Parameter | Details |
|---|---|
| Oral bioavailability | Excellent: ciprofloxacin ~70%, levofloxacin ~99%, moxifloxacin ~90% |
| Tmax | 1-3 hours |
| Distribution | Large Vd; concentrates in urine, kidney, lung, prostate, bile, macrophages, neutrophils - all exceed serum levels |
| Protein binding | Moderate (20-40%) |
| Excretion | Mostly renal (except moxifloxacin - hepatobiliary) |
| Half-lives | Ciprofloxacin 3-5h (BD dosing); levofloxacin ~7h (OD); moxifloxacin ~12h (OD); gemifloxacin ~8h |
| Renal impairment | Dose reduction needed for ciprofloxacin, levofloxacin, ofloxacin; NOT for moxifloxacin |
| Metabolism | Minimal CYP450 involvement (except ciprofloxacin inhibits CYP1A2); moxifloxacin by glucuronidation/sulfation |
| Breast milk | Detectable - caution in nursing mothers |
6. Therapeutic Uses
- Mainstay for complicated cystitis and pyelonephritis; superior to TMP-SMX and oral β-lactams
- Not moxifloxacin (inadequate urinary levels); 3 days for uncomplicated cystitis, 5-7 days for pyelonephritis
- "Respiratory fluoroquinolones" (levofloxacin, moxifloxacin, gemifloxacin, delafloxacin) cover pneumococcus + atypicals - used in community-acquired pneumonia (CAP)
- Ciprofloxacin + levofloxacin for Pseudomonas exacerbations in cystic fibrosis
- Traveler's diarrhea (ciprofloxacin, ofloxacin), enteric fever/typhoid, Campylobacter, Shigella
- Moxifloxacin monotherapy for intra-abdominal infections (anaerobic cover); others require metronidazole addition
- Avoid in Shiga toxin-producing E. coli diarrhea (risk of HUS)
- Chronic osteomyelitis (gram-negative; prolonged therapy)
- Levofloxacin, moxifloxacin, delafloxacin for complicated skin/soft tissue infections
- Ofloxacin/levofloxacin for chlamydial urethritis/cervicitis (7 days)
- No longer recommended for gonorrhea (widespread resistance)
- Second-line agents in MDR-TB and XDR-TB (moxifloxacin, levofloxacin)
- Active against atypical mycobacteria (MAC, M. kansasii)
- Prophylaxis for anthrax (Bacillus anthracis) - ciprofloxacin/levofloxacin
- Plague (Yersinia pestis) and tularemia
- Prophylaxis in febrile neutropenia (reduces gram-negative bacteremias)
7. Adverse Effects
Gastrointestinal (Most Common)
- Nausea, vomiting, abdominal discomfort (3-17%)
- Leading cause of Clostridioides (Clostridium) difficile colitis due to spread of quinolone-resistant strains
CNS (1-11%)
- Headache, dizziness, insomnia, anxiety
- Rare but serious: hallucinations, delirium, seizures (risk increased with theophylline or NSAIDs co-use)
- Peripheral neuropathy and possible optic neuritis - may be irreversible
Musculoskeletal
- Tendinitis and tendon rupture (especially Achilles) - most common in:
- Age >60 years
- Concurrent corticosteroid use
- Solid-organ transplant recipients
- Arthralgia; avoided in children due to animal cartilage damage data (though long-term studies show no growth inhibition)
Cardiovascular
- QT interval prolongation and torsades de pointes
- Risk ranking: Moxifloxacin (highest) > gemifloxacin = levofloxacin > ciprofloxacin (lowest)
- Avoid in long QT syndrome, hypokalemia, hypomagnesemia, with class IA/III antiarrhythmics
Other
- Photosensitivity/phototoxicity (advise sun protection)
- Dysglycemia (rare with current agents; was common with withdrawn gatifloxacin)
- Rash, hypersensitivity reactions
- Hepatotoxicity (rare; was cause of trovafloxacin withdrawal)
The FDA issued a Black Box Warning for fluoroquinolones covering: tendinitis/tendon rupture, peripheral neuropathy, CNS effects, and worsening of myasthenia gravis. Routine use in uncomplicated infections is discouraged.
- Goodman & Gilman's, p. 1163-1164
8. Drug Interactions
| Interacting Drug/Substance | Effect |
|---|---|
| Divalent/trivalent cations (antacids - Al³⁺, Mg²⁺; iron; calcium; sucralfate; zinc) | Chelation - markedly reduces oral bioavailability. Separate administration by ≥2 hours |
| Theophylline | Ciprofloxacin inhibits CYP1A2 - increases theophylline levels - risk of toxicity |
| NSAIDs | Displace GABA from CNS receptors - potentiate seizure risk |
| Class IA antiarrhythmics (quinidine, procainamide) | Additive QT prolongation - avoid |
| Class III antiarrhythmics (amiodarone, sotalol) | Additive QT prolongation - avoid |
| Warfarin | May potentiate anticoagulant effect - monitor INR |
| Sucralfate | Reduces FQ absorption - separate by 2h |
9. Bacterial Resistance
- Chromosomal mutations in gyrA/gyrB (DNA gyrase) and parC/parE (Topo IV) - most common; reduces drug-enzyme binding affinity
- Efflux pump upregulation (e.g., MexAB-OprM in Pseudomonas) - active drug export
- Porin channel downregulation - reduces drug entry across outer membrane (gram-negatives)
- Plasmid-mediated resistance (PMQR) - rare but transferable:
- Qnr proteins protect topoisomerases from quinolone binding
- AAC(6')-Ib-cr enzyme acetylates and inactivates the drug
- Cross-resistance: Mutation in one fluoroquinolone confers cross-resistance to all class members
- Goodman & Gilman's, p. 1162; Katzung's Basic and Clinical Pharmacology, 16th Ed.
10. Contraindications and Cautions
- Pregnancy: Avoid (arthropathy risk in animal studies; limited but concerning human data)
- Children <18 years: Generally avoid; use only when no alternatives exist (AAP guideline)
- Epilepsy: Higher risk for FQ-induced seizures
- Myasthenia gravis: May worsen neuromuscular blockade (FDA Black Box Warning)
- Concurrent QT-prolonging drugs: Avoid especially moxifloxacin
- G6PD deficiency: Use with caution (some members cause hemolysis)
11. Quick Comparison of Key Members
| Drug | Gen | Anti-Pseudo | Pneumococcus | Anaerobes | UTI | Dosing | QT Risk |
|---|---|---|---|---|---|---|---|
| Nalidixic acid | 1st | No | No | No | Only | - | Low |
| Norfloxacin | 2nd | Poor | Poor | No | Yes | BD | Low |
| Ciprofloxacin | 2nd | +++ | + | No | Yes | BD | Lowest |
| Ofloxacin | 2nd | + | + | No | Yes | BD | Low |
| Levofloxacin | 3rd | ++ | ++ | No | Yes | OD | Low |
| Moxifloxacin | 4th | No | +++ | Yes | No | OD | Highest |
| Gemifloxacin | 4th | No | +++ | No | No | OD | Moderate |
| Delafloxacin | 4th | + | +++ | Moderate | Yes | BD | Low |
12. Key Exam Points
- Bactericidal, concentration-dependent killing; parameter = AUC/MIC
- Primary target in gram-negatives = DNA gyrase; gram-positives = Topoisomerase IV
- Quinolones are not active against Treponema pallidum
- Ciprofloxacin = most potent against Pseudomonas among FQs; also drug of choice for anthrax prophylaxis
- Moxifloxacin = only FQ with anaerobic (B. fragilis) cover; also has highest QT risk; no renal dose adjustment; not for UTIs
- FQs are contraindicated in pregnancy and generally in children
- Chelation with antacids/iron/zinc = give 2 hours apart
- FDA Black Box: tendon rupture, peripheral neuropathy, myasthenia gravis worsening, CNS effects
Why flourorquinolones causes tendon rupture and peripheral neuropathy
fluoroquinolone tendon rupture mechanism
fluoroquinolone peripheral neuropathy mechanism mitochondria
PMID: 30811525
PMID: 40005998
PMID: 37501614
fluoroquinolone neuropathy mechanism oxidative stress
PMID: 40558212
fluoroquinolone peripheral neuropathy mechanism mitochondrial DNA damage ion channels tenocytes pathophysiology
Why Fluoroquinolones Cause Tendon Rupture and Peripheral Neuropathy
Overview: A Shared Root
PART 1: Tendon Rupture and Tendinopathy
Why tendons are the target
Five identified mechanisms (from a 2019 systematic review - PMID 30811525):
Mechanism 1: Reactive Oxygen Species (ROS) and Mitochondrial Damage
- FQ enters the mitochondrial matrix
- Inhibits the mitochondrial electron transport chain (specifically Complex I activity)
- Excess electrons leak and react with oxygen → superoxide (O₂⁻) and H₂O₂
- ROS causes oxidative damage to mitochondrial membranes, mitochondrial DNA (mtDNA), and proteins
- Mitochondrial membrane potential (ΔΨm) collapses → opens the permeability transition pore (PTP)
- PTP opening releases cytochrome c → triggers apoptosis of tenocytes
- Loss of tenocytes = loss of collagen maintenance = structurally weakened tendon
A targeted mitochondrial antioxidant (MitoQ) has been shown to prevent FQ-induced oxidative stress and preserve mitochondrial membrane potential in human Achilles tendon cells - confirming mitochondrial ROS as a primary mechanism.
Mechanism 2: Inhibition of Type I Collagen Synthesis and MMP Upregulation
- Reduced synthesis: Ciprofloxacin inhibits tenocyte production of type I collagen, elastin, proteoglycans, and fibronectin
- Increased degradation: FQs upregulate matrix metalloproteinases (MMP-1, MMP-2, MMP-13) - enzymes that break down the extracellular matrix (ECM)
Mechanism 3: Inhibition of Tenocyte Proliferation (Cell Cycle Arrest)
- Decreasing activity of Cyclin B and CDK-1 (Cyclin-dependent kinase 1) - essential for G2/M phase progression
- Decreasing CHK-1 (Checkpoint kinase 1) activity
- Increasing PK-1 expression
Mechanism 4: Inhibition of Tenocyte Migration (FAK Pathway)
- Decreasing phosphorylation of FAK (Focal Adhesion Kinase) - a signaling molecule that mediates cell migration and attachment to ECM
- Tenocytes fail to migrate to injury sites → healing is impaired
Mechanism 5: Metal Ion Chelation and Epigenetic Effects
- Essential cofactors for collagen cross-linking enzymes (lysyl oxidase requires Cu²⁺)
- Required for DNA repair enzymes
- Critical for antioxidant enzymes (SOD requires Zn²⁺/Cu²⁺, glutathione peroxidase requires Se)
- Impair collagen crosslinking → weakened tensile strength
- Disable antioxidant defenses → worsened ROS damage
- Inhibit DNA repair mechanisms in tenocytes
Structural changes seen in tendons (animal studies)
- Swelling with infiltration of mononuclear cells
- Disruption of collagen deposition in synovial membranes and tendon sheaths
- Mucoid degeneration and fragmentation of tenocyte nuclei
- Detachment of tenocytes from the ECM
- Swelling of mitochondria and endoplasmic reticulum within tenocytes
Risk factors for tendon rupture
| Risk Factor | Why it matters |
|---|---|
| Age >60 years | Baseline reduced tenocyte activity and vascularity |
| Concurrent corticosteroids | Also inhibit collagen synthesis + additive tenocyte apoptosis |
| Solid organ transplant recipients | Immunosuppressants impair tendon repair; often on corticosteroids |
| Chronic renal failure | Reduced FQ clearance → higher tissue concentrations |
| Male sex | Higher baseline tendon load |
| Achilles tendon | Poorest blood supply of any tendon; highest mechanical load |
- Campbell Walsh Wein Urology; Goodman & Gilman's, p. 1163
PART 2: Peripheral Neuropathy
Why nerves are vulnerable
Mechanisms of FQ-induced peripheral neuropathy:
Mechanism 1: Mitochondrial DNA Damage - The Core Mechanism
- FQs inhibit human mitochondrial topoisomerase II (a eukaryotic enzyme present in mitochondria)
- This causes mitochondrial DNA (mtDNA) strand breaks and impairs mtDNA replication
- Reduced mtDNA → reduced synthesis of mitochondrial respiratory chain proteins
- Progressive mitochondrial dysfunction → energy failure in peripheral axons
- Na⁺/K⁺-ATPase cannot maintain resting membrane potential → axonal depolarization and dysfunction
- Axonal degeneration ensues, producing a sensorimotor neuropathy
Note: Ciprofloxacin has been specifically shown to inhibit mitochondrial topoisomerase II and impair mitochondrial DNA replication initiation. This is the same basic mechanism by which FQs kill bacteria (inhibiting bacterial topoisomerase II/DNA gyrase), but applied to human mitochondria - which evolutionarily descend from bacteria and share similar topology.
Mechanism 2: Oxidative Stress in Neurons
- FQ-generated ROS in neurons (same pathway as in tenocytes)
- Neurons are particularly ROS-sensitive due to high oxygen consumption, abundant polyunsaturated fatty acids in membranes, and limited antioxidant capacity
- ROS causes lipid peroxidation of the axonal membrane and myelin sheath
- Oxidative damage to nerve proteins and axonal transport machinery
- Schwann cell dysfunction → impaired myelin synthesis and maintenance → demyelination
Mechanism 3: GABA-A Receptor Antagonism and Neuronal Hyperexcitability
- FQs are competitive antagonists at GABA-A receptors (gamma-aminobutyric acid type A)
- Reducing GABAergic inhibition causes neuronal hyperexcitability
- While primarily explaining CNS effects (seizures, anxiety), this contributes to dysesthesias and neuropathic pain of peripheral neuropathy
- NSAIDs potentiate this effect by also displacing GABA from its receptor (explains why NSAID + FQ is high risk)
Mechanism 4: Ion Channel Disruption
- FQs may directly inhibit voltage-gated potassium channels (Kv1.5) on peripheral nerve axons
- K⁺ channel inhibition → abnormal repolarization → sustained membrane depolarization → axonal excitability and firing abnormalities
- This contributes to burning, tingling, and paresthesias characteristic of FQ neuropathy
- Also contributes to ROS cascade (altered K⁺ channels trigger downstream oxidative events)
Mechanism 5: Inhibition of Protein Synthesis in Neurons
- At high tissue concentrations, FQs reduce protein synthesis in neural tissue
- Disrupts axonal transport proteins and structural proteins of the cytoskeleton
- Impairs ability of neurons to maintain long axons → dying-back neuropathy (distal axonopathy)
Clinical pattern of FQ-induced neuropathy
-
Type: Primarily sensory or sensorimotor; may be axonal or demyelinating (including rare Guillain-Barré-like presentations)
-
Onset: Can occur days to weeks after starting treatment, or even after stopping
-
Symptoms: Burning pain, numbness, tingling (paresthesias), weakness, proprioception loss
-
Severity: Usually mild-moderate; may be irreversible in some cases (FDA Black Box 2013)
-
Course: Some patients worsen months or years after completing the antibiotic course - consistent with ongoing mitochondrial dysfunction
-
Adams and Victor's Principles of Neurology; Goodman & Gilman's, p. 1163
PART 3: The Unified Mitochondrial Toxicity Model
Fluoroquinolone enters cell
│
▼
Inhibits mitochondrial Topo II → mtDNA damage
│
▼
Mitochondrial respiratory chain dysfunction
│
┌─────┴─────┐
▼ ▼
In TENOCYTES In PERIPHERAL AXONS
│ │
ROS ↑ Energy failure (ATP ↓)
MMP ↑ Na⁺/K⁺-ATPase failure
Collagen ↓ Axonal degeneration
Tenocyte Demyelination
apoptosis
│ │
▼ ▼
TENDON PERIPHERAL
RUPTURE NEUROPATHY
Summary Table
| Feature | Tendon Rupture | Peripheral Neuropathy |
|---|---|---|
| Primary mechanism | ROS + mitochondrial damage in tenocytes; MMP upregulation | mtDNA damage → energy failure in axons |
| Cell target | Tenocytes | Peripheral neurons + Schwann cells |
| Molecular target | Mitochondrial Complex I; MMPs; FAK; Cyclin B/CDK1 | Mitochondrial Topo II; GABA-A receptor; Kv channels |
| Collagen role | ↓ synthesis + ↑ degradation | Not applicable |
| Reversibility | Often irreversible once ruptured | May be irreversible (FDA warning) |
| Most affected tendon | Achilles (worst blood supply) | Distal extremities (longest axons) |
| Risk amplifier | Corticosteroids | Concurrent NSAIDs |
| Time course | Days to weeks; even after stopping | Days to months; can worsen post-course |
Why mannitol and hydrochloride is added with moxifloxacin
why mannitol added moxifloxacin IV formulation Avelox role excipient pharmaceutical
moxifloxacin hydrochloride mannitol tablet formulation inactive ingredients role
https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/02…
moxifloxacin mannitol role filler diluent tablet pharmaceutical why chosen over lactose
Why Mannitol and Hydrochloride Are Added with Moxifloxacin
1. Moxifloxacin Hydrochloride - Why the HCl Salt?
The problem: Poor aqueous solubility of the free base
The solution: Salt formation (acid-base chemistry)
Moxifloxacin (free base) + HCl → Moxifloxacin hydrochloride
(sparingly soluble) (freely soluble)
Monohydrochloride salt of 1-cyclopropyl-7-[(S,S)-2,8-diazabicyclo[4.3.0]non-8-yl]-6-fluoro-8-methoxy-1,4-dihydro-4-oxo-3-quinoline carboxylic acid Empirical formula: C₂₁H₂₄FN₃O₄ · HCl | MW = 437.9 g/mol
Specific benefits of the HCl salt form:
| Benefit | Explanation |
|---|---|
| Improved aqueous solubility | The ionized (protonated) form dissolves readily in water - essential for both tablet dissolution and IV solution preparation |
| Chemical stability | Salt forms are generally more physically and chemically stable than free bases; better shelf life |
| Consistent bioavailability | Reliable dissolution → predictable absorption → consistent plasma levels |
| Manufacturability | The salt crystallizes well into a uniform, stable powder suitable for tablet compression |
| IV compatibility | The HCl salt dissolves completely in aqueous solution, enabling a clear, stable injectable solution at a pH of 4.1-4.6 |
The hydrochloride form is the active pharmaceutical ingredient (API) itself - it is not an excipient. The drug is always described as "moxifloxacin hydrochloride" in prescribing information because this is what is actually present in the formulation.
- Avelox FDA Prescribing Information; DailyMed
2. Mannitol - Role as a Pharmaceutical Excipient
Where mannitol appears
The Avelox IV injection does NOT contain mannitol - it uses sodium chloride 0.8% as the tonicity agent/vehicle.
What is mannitol?
Roles of mannitol in tablet formulation:
A. Diluent / Filler (Primary role, 10-90% of tablet weight)
- A 400 mg moxifloxacin tablet would be too small to handle without bulk-adding excipients
- Mannitol adds the necessary physical mass to make a tablet of practical, compressible size
- Ensures uniform mixing and consistent drug content per tablet
B. Why mannitol instead of lactose?
| Property | Mannitol | Lactose |
|---|---|---|
| Lactose intolerance | Suitable for intolerant patients | Contraindicated |
| Hygroscopicity | Non-hygroscopic - does not absorb moisture | Slightly hygroscopic |
| Chemical reactivity | Chemically inert; no Maillard reaction | Can react with amine groups (Maillard reaction causes browning, degradation) |
| Taste | Mild sweetness, pleasant mouthfeel | Also sweet but less preferred |
| Stability | Better for moisture-sensitive drugs | Less protective |
Moxifloxacin's primary amine/piperazine group is susceptible to Maillard reaction with reducing sugars like lactose. Mannitol, being a non-reducing sugar alcohol, does not react with amines - making it chemically compatible and preventing drug degradation.
C. Diluent for Direct Compression
- Spray-dried mannitol has excellent flowability and compressibility
- Allows direct compression manufacturing (no wet granulation needed) → faster, simpler, more economical production
- Produces tablets with good hardness, low friability, and rapid disintegration
D. Moisture Protection (Non-hygroscopic nature)
- Mannitol does not attract atmospheric moisture
- Protects the moisture-sensitive drug substance from hydrolysis during shelf life
- Particularly valuable in hot/humid climates (important for a globally distributed antibiotic)
E. Disintegration Aid
- Mannitol contributes to tablet wettability - as the tablet enters GI fluid, mannitol draws water in
- Facilitates faster tablet disintegration → faster drug release → faster onset
- Works in concert with croscarmellose sodium (the formal disintegrant in the tablet)
3. Complete Formulation Summary
Moxifloxacin Tablet 400 mg (Generic, per FDA DailyMed)
| Ingredient | Class | Function |
|---|---|---|
| Moxifloxacin hydrochloride | Active ingredient | Drug (as HCl salt for solubility) |
| Mannitol | Inactive (excipient) | Diluent/filler; non-hygroscopic; no Maillard reaction |
| Microcrystalline cellulose | Inactive | Binder + filler; compressibility |
| Croscarmellose sodium | Inactive | Disintegrant - rapid tablet breakup |
| Magnesium stearate | Inactive | Lubricant - prevents sticking to machinery |
| Hypromellose (HPMC) | Inactive | Film coat binder |
| Titanium dioxide | Inactive | Opacifier in film coat (white colour) |
| Polyethylene glycol | Inactive | Plasticizer in film coat |
Moxifloxacin IV Injection 400 mg/250 mL (Avelox brand)
| Ingredient | Function |
|---|---|
| Moxifloxacin hydrochloride | Active ingredient |
| Sodium chloride 0.8% | Tonicity agent - makes solution isotonic (not mannitol) |
| Water for injection | Vehicle/solvent |
| Hydrochloric acid / Sodium hydroxide | pH adjustment to 4.1-4.6 |
4. Key Exam Points
- Moxifloxacin HCl = the drug itself in salt form; HCl improves aqueous solubility and stability (not an excipient)
- Mannitol in tablets = inert filler/diluent; chosen over lactose because:
- Non-hygroscopic (protects moisture-sensitive drug)
- No Maillard reaction with moxifloxacin's amine group
- Suitable for lactose-intolerant patients
- Excellent direct compression properties
- Avelox IV uses sodium chloride as tonicity agent, not mannitol
- The yellow colour of moxifloxacin solution is from the drug itself (inherent chromophore), not any dye - "the color does not affect, nor is it indicative of, product stability" (FDA label)