What is tenea and how we treat it?
Reading File
Finding Sources
Searching the Web
tinea fungal infection types treatment 2024
Searching PubMed
"tinea" AND "treatment"
Reading File
Reading File
Searching Images
tinea ringworm fungal skin infection
Reading File
Reading File
Reading File
I now have enough information for a thorough answer. Let me compile everything:
Tinea (Ringworm) — Fungal Skin Infections
Tinea (you may have meant tinea, also called ringworm) is a group of superficial dermatophyte fungal infections of the skin, hair, and nails. Despite the name "ringworm," no worm is involved — it is caused by three genera of fungi: Trichophyton, Microsporum, and Epidermophyton.
Clinical Types (by body site)
Tinea is named by the Latin term for the body part affected:
| Type | Site | Common Pathogens |
|---|---|---|
| Tinea capitis | Scalp & hair | T. tonsurans (USA), M. canis (Europe) |
| Tinea corporis | Body (glabrous skin) | T. rubrum, M. canis, T. mentagrophytes |
| Tinea cruris ("jock itch") | Groin, inner thighs | T. rubrum, E. floccosum |
| Tinea pedis ("athlete's foot") | Feet | T. rubrum, T. interdigitale |
| Tinea unguium / Onychomycosis | Nails | T. rubrum |
| Tinea barbae | Beard area | T. interdigitale, T. verrucosum |
| Tinea versicolor | Trunk (patchy) | Malassezia spp. |
Clinical Features
Tinea Corporis (most classic presentation)
Characterized by annular (ring-shaped), sharply circumscribed, erythematous, scaly plaques with an advancing raised border and central clearing. Multiple polycyclic or psoriasiform patterns may develop in immunocompromised patients. The classic "ringworm" appearance results from this progressive central clearing.

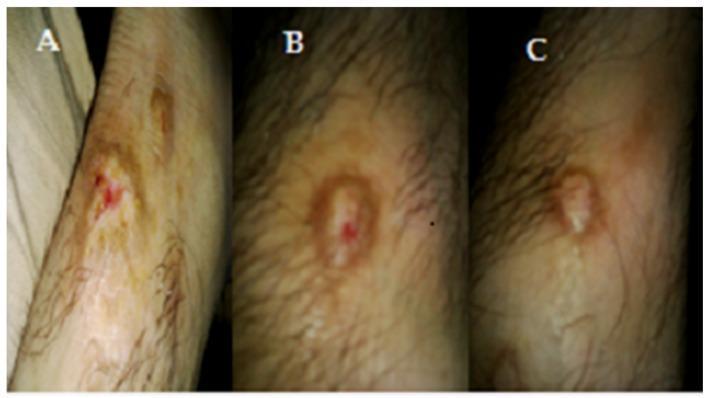
Treatment progression of tinea corporis over 2 weeks:
Tinea Capitis (scalp)
Most common in children aged 3–14. Presents with hair loss and scaling with varying inflammation:
- Gray patch type: circumscribed scaly alopecia with broken-off gray hairs
- Black dot type: hair broken at scalp level leaves black dots; caused by endothrix organisms (T. tonsurans)
- Kerion: boggy, inflamed, crusted mass with pustules and sinus tracts — can cause scarring alopecia if untreated
Tinea Cruris ("Jock itch")
Well-marginated annular plaque extending from the inguinal fold to the inner thigh (often bilateral), with a raised scaly border. Pruritus is prominent. Three times more common in men. Scrotum typically spared (helps distinguish from candidiasis).
Tinea Pedis (Athlete's Foot)
Commonly presents in the web spaces between toes with maceration, scaling, and fissuring. Can form vesicles and bullae (bullous tinea). Most prevalent dermatophyte infection worldwide.
Diagnosis
- KOH preparation: skin/hair scraping under microscope — shows branching hyphae
- Fungal culture: identifies species within 1–2 weeks
- Wood's lamp: some Microsporum species fluoresce green (ectothrix infections)
- Biopsy: useful for chronic refractory cases (tinea incognita)
Treatment
Topical Antifungals (first-line for localized tinea corporis, cruris, pedis)
| Drug | Class | Dosing |
|---|---|---|
| Terbinafine (Lamisil) | Allylamine | Once daily × 1–2 weeks |
| Clotrimazole (Lotrimin) | Azole | Twice daily × 2–4 weeks |
| Miconazole (Monistat) | Azole | Twice daily × 2–4 weeks |
| Ketoconazole (Nizoral) | Azole | Once daily |
| Econazole (Spectazole) | Azole | Once daily |
| Naftifine (Naftin) | Allylamine | Once/twice daily |
| Ciclopirox olamine (Loprox) | Hydroxypyridinone | Twice daily |
Most topical courses last 2–4 weeks; terbinafine can be effective in just 1 week.
⚠️ Avoid combination products with potent corticosteroids (e.g., clotrimazole/betamethasone) — they frequently cause widespread tinea and fungal folliculitis.
Systemic Antifungals (oral — for extensive, follicular, or scalp disease)
| Drug | Main Indication |
|---|---|
| Griseofulvin | Tinea capitis (traditional first-line in children) |
| Terbinafine (oral) | Tinea capitis, onychomycosis, extensive tinea |
| Itraconazole | Tinea capitis, onychomycosis, extensive tinea |
| Fluconazole | Alternative for tinea corporis/cruris |
Tinea capitis requires systemic therapy — topical agents cannot penetrate the hair follicle adequately.
Onychomycosis (nail tinea) also requires systemic or specialized topical therapy (e.g., efinaconazole/ciclopirox lacquer).
Prevention
- Keep skin dry; change socks and underwear daily
- Avoid sharing towels, combs, or clothing
- Treat infected household contacts and pets (M. canis from cats/dogs is a common source)
- Miconazole powder can help prevent recurrence in high-risk individuals (hyperhidrosis, obesity)
⚠️ Emerging Resistance Alert (2025)
Recent systematic reviews (PMID 39082800 and PMID 40704771) highlight the emergence of terbinafine-resistant Trichophyton indotineae spreading in Europe and Australia. This strain, originally from South Asia, can fail standard terbinafine therapy. When standard treatment fails, testing for resistance and alternative agents (itraconazole, voriconazole) should be considered.
Sources: Andrews' Diseases of the Skin (9780323547536); Fitzpatrick's Dermatology, 8th ed. (9780071837781)
This is a shared conversation. Sign in to Orris to start your own chat.