Exam oriented note Long Essay KUHS
cd /tmp/workspace/attachments/7b24e837-0e2e-4f0e-9c6a-ca7fc6831039/ && python3 -c " import pdfplumber with pdfplumber.open('CN 7.pdf') as pdf: print(f'Total pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages[:5]): text = page.extract_text() if text: print(f'--- PAGE {i+1} ---') print(text[:2000]) "
CRANIAL NERVE VII - FACIAL NERVE
Exam-Oriented Long Essay Notes (KUHS Format)
INTRODUCTION
- The facial nerve is the 7th cranial nerve.
- It is a mixed nerve (motor + sensory) but predominantly motor.
- It supplies the muscles of facial expression - hence its name.
- It is the most frequently paralyzed of all peripheral nerves.
FUNCTIONAL COMPONENTS AND NUCLEI
| Component | Type | Nucleus | Function |
|---|---|---|---|
| 1 | Special Visceral Efferent (SVE) | Motor nucleus of facial nerve (pons) | Muscles of facial expression |
| 2 | General Visceral Efferent (GVE) | Lacrimatory nucleus + Superior salivatory nucleus | Secretomotor to lacrimal, submandibular, sublingual glands |
| 3 | Special Visceral Afferent (SVA) | Nucleus of tractus solitarius (gustatory nucleus) | Taste from anterior 2/3 of tongue (except vallate papillae) |
| 4 | General Somatic Afferent (GSA) | Spinal nucleus of trigeminal nerve | General sensation from skin of auricle |
COURSE AND RELATIONS
Two Roots
- (a) Motor root - large, medial (facial nerve proper)
- (b) Sensory root - small, lateral (nervus intermedius)
Origin
- Both roots arise from the pontomedullary junction, lateral to the superior end of the olive of the medulla.
- The sensory root (nervus intermedius) lies between the motor root (medially) and the vestibulocochlear nerve (laterally).
Cerebellopontine Angle
- After emerging from the brainstem, both roots pass laterally and forward in the cerebellopontine angle.
- They travel along with the vestibulocochlear nerve and the labyrinthine artery.
- All enter the internal acoustic meatus.
Internal Acoustic Meatus
- Motor root lodges in a groove on the vestibulocochlear nerve; sensory root remains separate.
- At the lateral end (fundus) of the internal acoustic meatus, the two roots unite to form the trunk of the facial nerve.
Facial Canal (Petrous Temporal Bone)
| Segment | Location | Key Feature |
|---|---|---|
| Labyrinthine | Above the vestibule of bony labyrinth | Contains the external genu and geniculate ganglion |
| Tympanic | Runs horizontally backward in medial wall of middle ear | Ends at junction of medial and posterior wall of middle ear |
| Mastoid | Passes vertically downward in posterior wall of middle ear | Ends at stylomastoid foramen |
- The sharp bend at the labyrinthine segment is the external genu - site of the geniculate ganglion.
- The facial nerve exits the cranial cavity through the stylomastoid foramen.
BRANCHES AND DISTRIBUTION
Branches Within the Facial Canal (Before Stylomastoid Foramen)
- Arises from the geniculate ganglion.
- Carries preganglionic parasympathetic (GVE) fibres to the pterygopalatine ganglion.
- Supplies secretomotor fibres to: lacrimal gland, mucous glands of nasal cavity and palate.
- Supplies the stapedius muscle in the middle ear.
- Stapedius dampens ossicular chain vibration - damage causes hyperacusis.
- Contains two types of fibres:
- (a) Preganglionic parasympathetic (GVE) - secretomotor to submandibular and sublingual glands (via submandibular ganglion).
- (b) Special visceral afferent (SVA) - carries taste from anterior 2/3 of tongue.
- Crosses the middle ear, exits through the petrotympanic fissure, joins the lingual nerve.
Branches After Stylomastoid Foramen
- Supplies the occipital belly of occipitofrontalis.
- Supplies the digastric muscle (posterior belly).
- Supplies the stylohyoid muscle.
Five Terminal Branches (in the Parotid Gland)
| Branch | Supplies |
|---|---|
| T - Temporal | Frontalis, orbicularis oculi, corrugator supercilii |
| Z - Zygomatic | Orbicularis oculi (lower part) |
| B - Buccal | Buccinator, muscles of upper lip and nose |
| M - Marginal Mandibular | Muscles of lower lip and chin (depressor anguli oris, mentalis) |
| C - Cervical | Platysma |
CLINICAL CORRELATIONS (HIGH YIELD)
1. Lesions of the Facial Nerve
A. SUPRANUCLEAR (Upper Motor Neuron) Lesion
- Lesion is above the facial nerve nucleus (e.g., internal capsule, cortex - as in stroke).
- Upper face is SPARED because the upper face (forehead/frontalis) receives bilateral cortical representation.
- Only the contralateral lower face is paralyzed.
- Emotional movements may be preserved (dissociation between voluntary and emotional).
B. INFRANUCLEAR (Lower Motor Neuron) Lesion
- Lesion at or below the nucleus.
- Entire ipsilateral half of face is paralyzed (both upper and lower face).
- No forehead sparing.
| Site of Lesion | Branches Affected | Clinical Features |
|---|---|---|
| In the pons (nucleus) | All | LMN facial palsy + ipsilateral abducens palsy (CN VI nucleus nearby) |
| Cerebellopontine angle | All + CN VIII | Facial palsy + deafness + tinnitus/vertigo |
| At/proximal to geniculate ganglion | All branches | LMN palsy + loss of lacrimation + hyperacusis + loss of taste |
| Between geniculate ganglion and nerve to stapedius | Below great petrosal | LMN palsy + hyperacusis + loss of taste (lacrimation intact) |
| Between nerve to stapedius and chorda tympani | Below nerve to stapedius | LMN palsy + loss of taste (lacrimation and hearing intact) |
| At/distal to stylomastoid foramen | Only motor | Pure LMN facial palsy (no sensory/autonomic loss) |
2. Bell's Palsy
- Most common cause of LMN facial nerve palsy.
- Etiology: Idiopathic; likely due to HSV-1 reactivation leading to inflammation and edema of the facial nerve in the confined facial canal.
- Self-limited, typically monophasic, acute-subacute onset.
- Features:
- Entire ipsilateral face paralyzed (LMN type - forehead NOT spared).
- Pain in 60% (around the ear/mastoid).
- Impaired lacrimation in 60%.
- Loss of taste (anterior 2/3 tongue) in 30-50%.
- Hyperacusis in 15-30% (stapedius affected).
- Prognosis: 85% spontaneously recover normal facial function within 3 weeks.
- Complications of aberrant regeneration:
- Crocodile tears syndrome (synkinesis - lacrimal gland re-innervated by fibres meant for salivary gland).
- Facial synkinesis (involuntary co-contraction).
3. Crocodile Tears Syndrome (Bogorad Syndrome)
- Paroxysmal lacrimation (tearing from one eye) during eating.
- Results from aberrant regeneration after facial nerve injury proximal to the geniculate ganglion.
- Fibres that originally supplied the submandibular gland (via chorda tympani) regrow and aberrantly innervate the lacrimal gland (via greater petrosal nerve pathway).
- Therefore, salivary stimuli trigger lacrimation.
4. Ramsay Hunt Syndrome (Herpes Zoster Oticus)
- Caused by reactivation of Varicella Zoster Virus (VZV) in the geniculate ganglion.
- Classic triad:
- Facial nerve palsy (LMN type)
- Herpetic vesicles in the external auditory meatus / auricle (sometimes soft palate)
- Otalgia (severe ear pain)
- May also have: tinnitus, vertigo, sensorineural deafness (CN VIII involvement).
- Prognosis is worse than Bell's palsy.
- Treatment: Acyclovir + prednisolone (early diagnosis is key).
5. Other Clinical Conditions
- Hemifacial spasm: Involuntary episodic contractions of facial muscles, usually due to compression of the facial nerve root by an aberrant vascular loop at the brainstem exit.
- Acoustic schwannoma (cerebellopontine angle tumor): Facial nerve involvement with sensorineural hearing loss; facial weakness is usually late.
- Parotid surgery: The intimate relationship of the facial nerve with the parotid gland makes parotidectomy a difficult dissection. Injury to its branches results in corresponding muscle weakness.
SUMMARY TABLE - STRUCTURES SUPPLIED
| Branch | Structure Supplied |
|---|---|
| Greater petrosal nerve | Lacrimal gland, nasal glands, palatal glands |
| Nerve to stapedius | Stapedius |
| Chorda tympani (GVE) | Submandibular + sublingual glands |
| Chorda tympani (SVA) | Taste, anterior 2/3 tongue |
| Posterior auricular nerve | Occipital belly of occipitofrontalis |
| Nerve to post. belly of digastric | Digastric (posterior belly) |
| Nerve to stylohyoid | Stylohyoid |
| 5 terminal branches | All muscles of facial expression + platysma |
EXAM TIPS (KUHS Long Essay)
- Draw the diagram of the facial nerve course from pons to stylomastoid foramen, marking all branches.
- Always tabulate the functional components with their nuclei and functions - easy marks.
- For clinical correlations: write Bell's palsy + Ramsay Hunt + Crocodile tears with explanations - these are consistently asked.
- The UMN vs LMN distinction (forehead sparing) is a classic KUHS exam point - always include it.
- Remember: the nerve to stapedius, chorda tympani, and greater petrosal nerve all branch within the facial canal (before the stylomastoid foramen) - use this for lesion localization.
- Mention the geniculate ganglion prominently - it is the sensory ganglion of the facial nerve and the site of herpes zoster reactivation in Ramsay Hunt.
Make a flow chart for course and relation
A detailed medical flowchart showing the course and relations of the Facial Nerve (CN VII). The flowchart flows vertically from top to bottom with connected boxes and arrows. Include the following steps in order: 1. TOP: "PONTOMEDULLARY JUNCTION" (large header box) - "Two roots emerge lateral to superior end of olive of medulla: Motor Root (large, medial) + Sensory Root / Nervus Intermedius (small, lateral)" 2. Arrow down to: "CEREBELLOPONTINE ANGLE" - "Both roots pass laterally & forward alongside Vestibulocochlear nerve (CN VIII) + Labyrinthine artery" 3. Arrow down to: "INTERNAL ACOUSTIC MEATUS" - "Motor root: lies in groove on CN VIII / Sensory root: remains separate / At FUNDUS (lateral end): Two roots UNITE → Trunk of Facial Nerve" 4. Arrow down to: "FACIAL CANAL" (in Petrous Temporal Bone) - Three sub-segments shown side by side: [LABYRINTHINE SEGMENT: Above vestibule of bony labyrinth → EXTERNAL GENU → GENICULATE GANGLION (sensory ganglion)] → [TYMPANIC SEGMENT: Runs horizontally backward in medial wall of middle ear] → [MASTOID SEGMENT: Runs vertically downward in posterior wall of middle ear] 5. Arrow down to: "STYLOMASTOID FORAMEN" - "Exits skull base" 6. Arrow down to: "PAROTID GLAND" - "Divides into Upper trunk & Lower trunk → Five terminal branches emerge from parotid borders: Temporal, Zygomatic, Buccal, Marginal Mandibular, Cervical" Show branches leaving the facial canal: Greater Petrosal Nerve (from geniculate ganglion), Nerve to Stapedius, Chorda Tympani, Posterior Auricular Nerve, Nerve to Post. Belly of Digastric, Nerve to Stylohyoid — each as small side arrows branching off at the correct level. Use a clean white background, navy blue boxes for main steps, light blue for sub-segments, yellow highlighted boxes for key landmarks (geniculate ganglion, stylomastoid foramen), red side arrows for branches. Clear readable medical font. Professional anatomy textbook style.
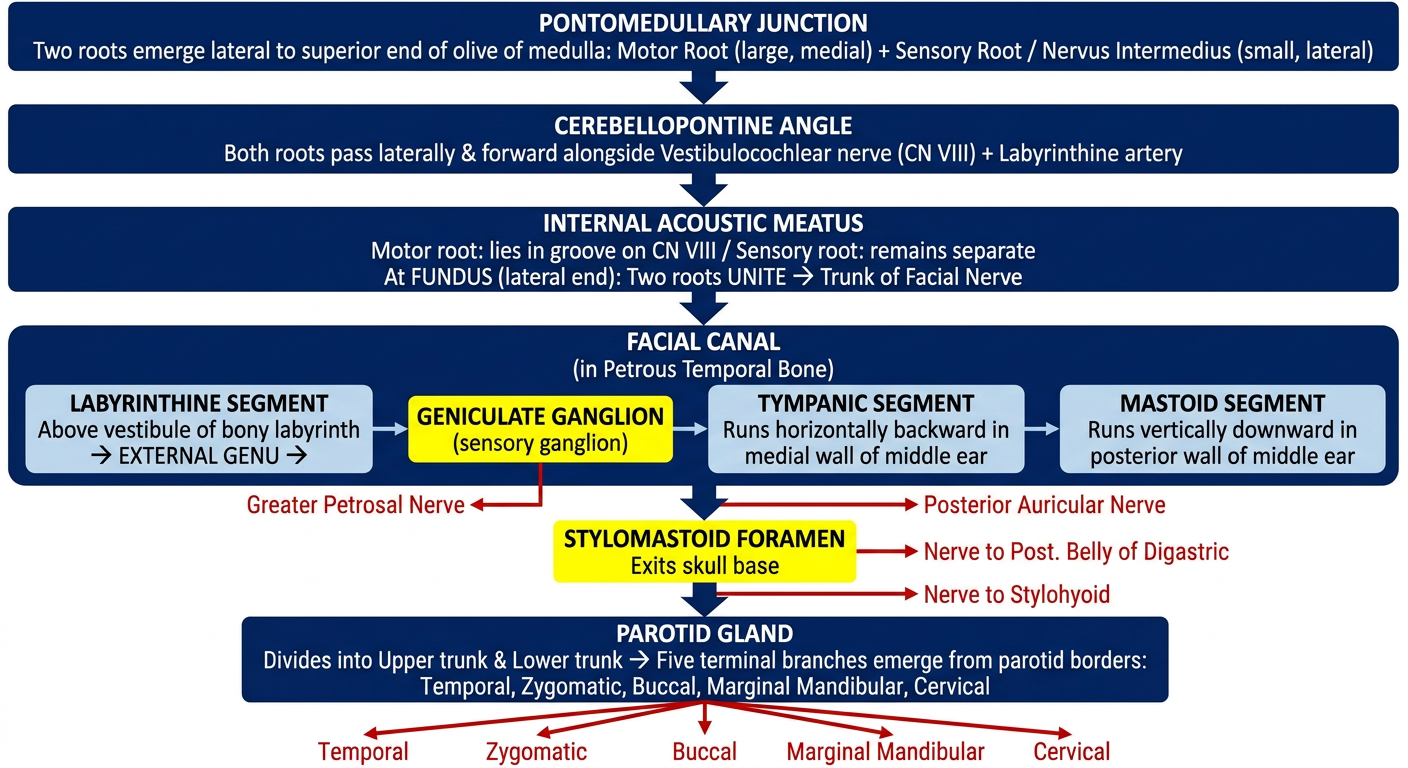
- Pontomedullary Junction - Two roots (motor + sensory) emerge
- Cerebellopontine Angle - Travel with CN VIII + labyrinthine artery
- Internal Acoustic Meatus - Roots unite at the fundus to form the trunk
- Facial Canal (3 segments):
- Labyrinthine → external genu → Geniculate ganglion (branches: Greater Petrosal Nerve)
- Tympanic → branches: Nerve to Stapedius, Chorda Tympani
- Mastoid → branches: Posterior Auricular, Nerve to Digastric, Nerve to Stylohyoid
- Stylomastoid Foramen - Exits the skull
- Parotid Gland - Divides into 5 terminal branches (T, Z, B, M, C)