Grades of ascites
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Grades of Ascites
The International Club of Ascites (ICA) classifies ascites into three grades based on the amount of fluid and how it is detected clinically.
Grade 1 - Mild
- Ascites detectable only by ultrasound
- Not apparent on physical examination
- No treatment required beyond sodium restriction (~90 mEq/day, i.e., 2 g sodium/day)
- Patients are counseled to reduce dietary salt intake
Grade 2 - Moderate
- Detected by physical examination - causes moderate, symmetric abdominal distension
- Shifting dullness or fluid thrill may be demonstrable
- Treated with sodium restriction + diuretics (spironolactone ± furosemide)
Grade 3 - Large / Tense
- Marked abdominal distension - tense ascites
- The patient is visibly and symptomatically distended
- Treated with large-volume paracentesis (LVP) to relieve discomfort, followed by diuretic maintenance
- LVP is more effective than diuretic therapy alone in reducing hospital stay and electrolyte complications
Refractory Ascites (a special category, not a grade per se)
Refractory ascites is ascites that persists despite adequate medical therapy and is classified into two subtypes:
| Subtype | Definition |
|---|---|
| Diuretic-resistant | Ascites does not respond to sodium restriction + maximum diuretic doses (spironolactone 400 mg/day + furosemide 160 mg/day) |
| Diuretic-intractable | Diuretic-induced side effects (encephalopathy, hyponatremia, renal impairment, hypo/hyperkalemia) prevent use of effective doses |
- Requires at least 3 recurrences within a 12-month period to qualify as "recurrent ascites"
- Management options: repeated LVP, TIPS (transjugular intrahepatic portosystemic shunt), liver transplantation
- Associated with poor prognosis and progression toward hepatorenal syndrome (HRS)
Pathophysiologic Basis
Ascites in cirrhosis results from two key mechanisms:
- Sinusoidal hypertension - hepatic venous pressure gradient (HVPG) must be >12 mmHg for ascites formation
- Sodium and water retention - splanchnic vasodilation decreases effective arterial blood volume, activating the renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system, promoting renal sodium retention
As cirrhosis advances, systemic inflammation worsens vasodilation, leading to dilutional hyponatremia and eventually hepatorenal syndrome - representing a pathogenic continuum from uncomplicated ascites to HRS.
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1799
- Yamada's Textbook of Gastroenterology, 7th ed., p. 2104
- Harrison's Principles of Internal Medicine, 22nd ed. (2025), p. 370
- Sabiston Textbook of Surgery, Biological Basis of Modern Surgical Practice
Hernia surgery incision
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have all the detail needed. Here is a comprehensive answer:
Hernia Surgery Incisions
1. Inguinal Hernia - Open Repair
Skin incision:
An oblique or horizontal incision is made over the groin, beginning two fingerbreadths (2-3 cm) inferior and medial to the anterior superior iliac spine (ASIS), then extended medially for approximately 6-8 cm toward the pubic tubercle, running parallel to the inguinal ligament.
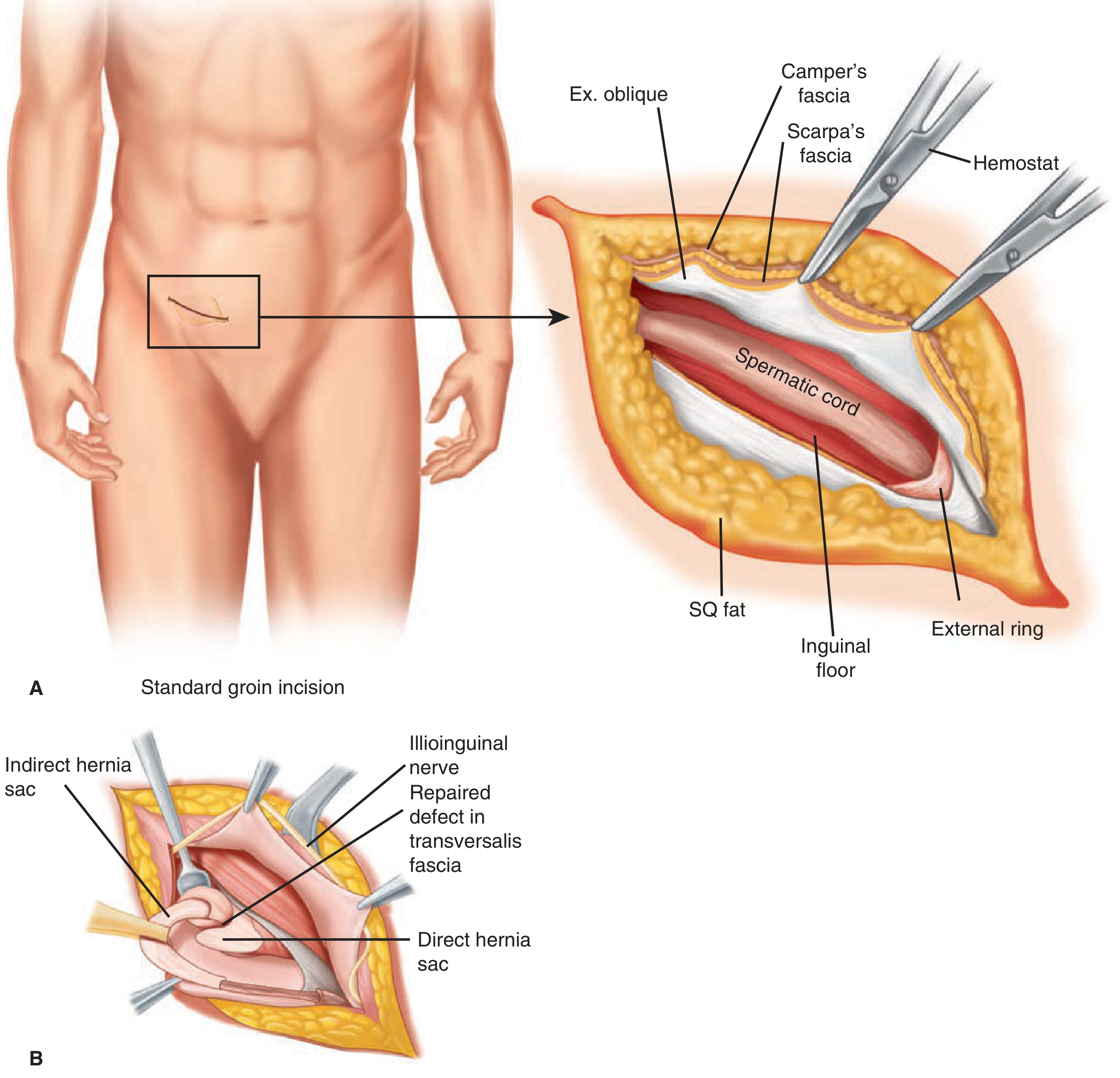
Figure: Standard groin incision (panel A) showing the skin incision site and the deep layers encountered - external oblique aponeurosis, Scarpa's fascia, spermatic cord, inguinal floor, and external ring. Panel B shows identification of indirect and direct hernia sacs.
Layers divided (deep to skin):
- Skin and subcutaneous fat
- Camper's fascia (superficial fatty layer)
- Scarpa's fascia (deeper membranous layer) - divided to expose external oblique aponeurosis
- External oblique aponeurosis - incised with a small cut parallel to its fibers, splitting open the external inguinal ring
- Metzenbaum scissors are spread beneath the fibers to sweep away the underlying ilioinguinal nerve (preserved)
- The inferior flap reveals the shelving edge of the inguinal ligament
- The spermatic cord (or round ligament in females) is encircled and elevated with a Penrose drain
Important nerves to identify and protect:
- Ilioinguinal nerve
- Iliohypogastric nerve
- Genital branch of the genitofemoral nerve (runs along the inferolateral cord surface)
2. Inguinal Hernia - Open Repair Techniques and Their Incisions
| Repair | Incision/Approach |
|---|---|
| Bassini | Standard oblique groin incision; external oblique opened; posterior wall reinforced by suturing conjoint tendon to inguinal ligament |
| Shouldice | Same groin incision; transversalis fascia additionally opened from deep ring to pubic tubercle ("central incision"), then double-breasted closure |
| Lichtenstein (tension-free mesh) | Same oblique groin incision; mesh sutured to inguinal ligament and conjoint tendon - no tension on tissues |
| McVay (Cooper's ligament repair) | Same incision; conjoint tendon sutured to Cooper's ligament; requires a relaxing incision in the anterior rectus sheath to reduce tension |
3. Femoral Hernia - Open Repair
Three incision approaches are used:
- Crural (low/Lockwood) approach: Transverse incision below the inguinal ligament over the femoral triangle in the upper thigh. Hernia approached from below and reduced; defect closed by suturing inguinal ligament to Cooper's ligament.
- Inguinal (high/Lotheissen) approach: Incision is identical to inguinal hernia repair (oblique groin). The inguinal canal is opened, cord mobilized, and hernia reduced from above the inguinal ligament.
- Preperitoneal approach: Access through an abdominal midline or lower transverse incision, or laparoscopically.
4. Umbilical Hernia
- Subumbilical "smile" incision - a curvilinear incision placed just below the umbilicus (Mayo repair). The hernia sac is excised and a "waistcoat" (vest-over-pants) overlap closure is performed.
- Alternatively, a circumumbilical incision encircling the umbilicus may be used.
- Larger defects (>3 cm) or recurrences: laparoscopic or robotic approach preferred.
5. Epigastric Hernia
- A small vertical or transverse midline incision directly over the defect in the linea alba. Simple closure of the defect ± mesh underlay.
6. Laparoscopic Inguinal Hernia Repair
Two main approaches - both avoid the anterior groin incision:
TAPP (Transabdominal Preperitoneal):
- 3 port sites: 10-12 mm port at the umbilicus (camera), plus two 5 mm ports placed laterally in the lower abdomen
- Peritoneum incised, mesh placed in the preperitoneal space, peritoneum closed over mesh
TEP (Totally Extraperitoneal):
- Small horizontal incision just inferior to the umbilicus - subcutaneous tissue dissected to anterior rectus sheath, which is incised lateral to the linea alba
- Rectus muscle retracted; dissecting balloon advanced toward pubic symphysis and inflated to create the preperitoneal space
- 12 mm balloon trocar at umbilicus + 5 mm port suprapubically in midline + one further 5 mm port inferior to the camera port
- Peritoneal cavity never entered
Key Anatomical Landmark Summary
| Hernia Type | Incision Location |
|---|---|
| Inguinal (open) | Oblique, 2-3 cm above and parallel to inguinal ligament, ASIS to pubic tubercle |
| Femoral (crural) | Transverse, below inguinal ligament over femoral triangle |
| Femoral (inguinal approach) | Same as inguinal hernia |
| Umbilical | Subumbilical curved "smile" or circumumbilical |
| Epigastric | Small midline over defect in linea alba |
| Laparoscopic (TAPP/TEP) | Periumbilical + lower abdominal port sites |
Sources:
- Schwartz's Principles of Surgery, 11th ed., pp. 1636-1643
- Bailey and Love's Short Practice of Surgery, 28th ed., pp. 1087, 2063-2076
- Mulholland and Greenfield's Surgery, 7th ed., pp. 3703-3725
- Fischer's Mastery of Surgery, 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.