Placenta privia for 5 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete, exam-ready 5-mark answer on Placenta Previa:
Placenta Previa
Definition
Placenta previa is the implantation of the placenta over or within 2 cm of the internal cervical os. It is a leading cause of antepartum hemorrhage (APH) in the second half of pregnancy.
- Low-lying placenta: placental edge within 2 cm of the internal os but not covering it
- Placenta previa (proper): placenta covers the internal os completely or partially
Modern classification (per NICHD) has replaced the older terms "complete," "partial," and "marginal" - the preferred terms are simply "placenta previa" (covering the os) and "low-lying placenta" (within 2 cm).
- Creasy & Resnik's Maternal-Fetal Medicine, p. 611
Incidence
- Affects approximately 0.5% (1 in 200) of all third-trimester pregnancies
- Diagnosed incidentally in ~10% of mid-trimester sonograms, but ~90% resolve before delivery (placental migration/trophotropism toward the fundus)
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1018
Risk Factors
| Risk Factor | Relative Risk Increase |
|---|---|
| Previous placenta previa | 8x |
| Previous cesarean section | 1.5-15x |
| Age > 35 years | 4.7x; age >40 = 9x |
| Multiparity | 1.1-1.7x |
| Prior curettage/abortion | 1.3x |
| Smoking, IVF conception | Elevated |
Underlying mechanism: prior endometrial damage and uterine scarring predisposes implantation to the lower segment.
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1018
Pathophysiology
Bleeding occurs because marginal placental vessels in the lower uterine segment are torn as:
- The lower uterine segment develops and elongates with advancing gestation
- The cervix effaces and dilates (labor or prelabor contractions)
- Intercourse or inadvertent vaginal examination disrupts vessels
Once labor begins, significant hemorrhage occurs as the cervix dilates and the placenta separates from the underlying decidua.
- Rosen's Emergency Medicine, p. 3356
Clinical Features
- Painless, bright-red vaginal bleeding in the second/third trimester - the hallmark
- Bleeding is sudden and recurrent ("herald bleeds" before major hemorrhage)
- Uterus is soft and non-tender (unlike abruptio placentae)
- Fetal lie may be abnormal (transverse/oblique) - the placenta prevents engagement
- Up to 10% of cases have no bleeding until onset of labor
- Rosen's Emergency Medicine, p. 3355
Important: Never perform digital vaginal examination in suspected placenta previa - this can precipitate catastrophic hemorrhage. Limit to atraumatic speculum examination only.
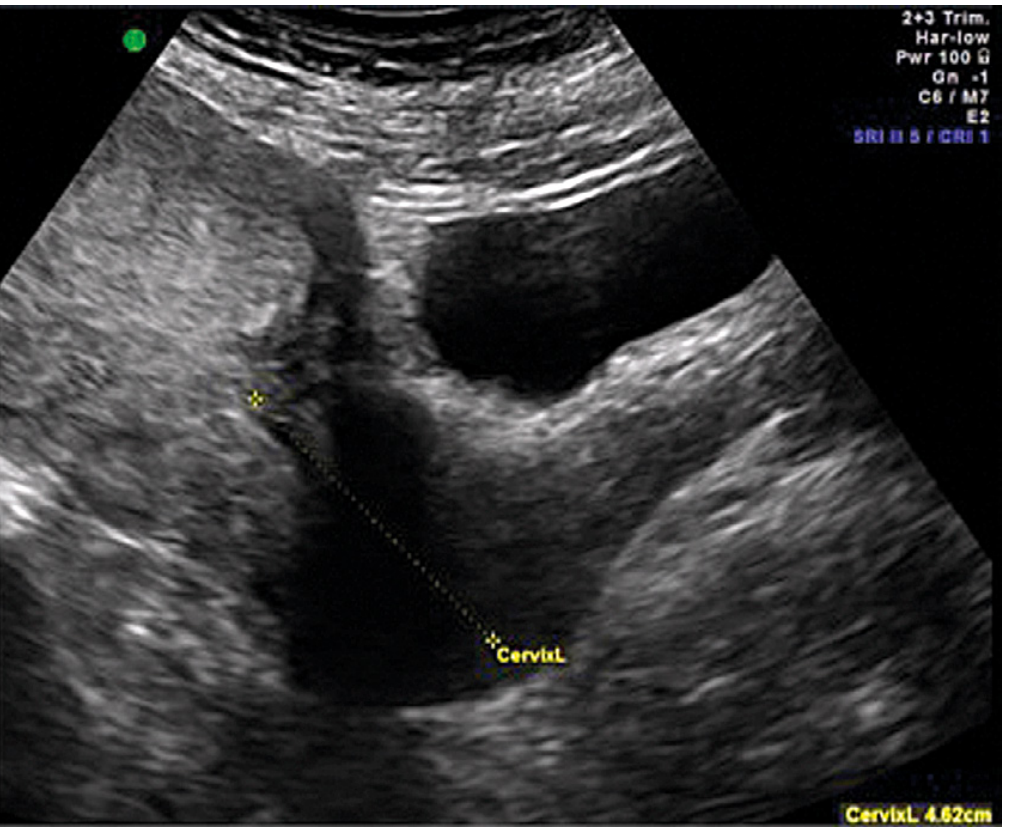
Diagnosis
Transvaginal ultrasound (TVUS) is the gold standard:
- More accurate than transabdominal US for placental-os relationship
- Bladder must be emptied before transabdominal scan to avoid false-positive diagnosis
- Placental edge >20 mm from internal os = normal
- Placental edge <20 mm but not covering os = low-lying placenta
- Placenta covering os = placenta previa
Management
Expectant (Conservative) Management
- Indicated if bleeding is not life-threatening and gestation < 36 weeks
- Hospital admission, two large-bore IV lines, fluid resuscitation, continuous fetal monitoring
- Baseline Hb, type and crossmatch, coagulation studies (fibrinogen <300 mg/dL = coagulopathy)
- Betamethasone (corticosteroids for lung maturity) if <34 weeks gestation
- Tocolytics (MgSO4 or beta-mimetics) may be used cautiously
- Rh-negative patients: 300 mcg anti-D immunoglobulin within 72 hours
- Bed rest, pelvic rest; avoid intercourse
- Cervical cerclage is NOT recommended
Definitive Management - Delivery
- All women with placenta within 2 cm of os → cesarean section (CS)
- Elective CS planned at 36-37 weeks (risk of sudden hemorrhage outweighs fetal benefit of continuing)
- Amniocentesis for lung maturity confirmation is not needed
- CS should be performed by the most experienced surgeon given high risk of intraoperative hemorrhage
- If anterior placenta: clamp umbilical cord immediately on entry
- Postpartum hemorrhage control: oxytocin, Methergine, carboprost (15-methyl PGF2α), B-Lynch suture, Bakri balloon; in refractory cases - hysterectomy
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1019-1020
Complications
- Maternal: antepartum/postpartum hemorrhage, DIC, shock, hysterectomy
- Fetal: prematurity, IUGR, fetal distress, perinatal mortality
- Associated conditions: placenta accreta spectrum (especially with prior CS + anterior previa), vasa previa
Key exam points to remember:
- Painless APH = placenta previa until proven otherwise
- NO digital vaginal examination
- TVUS is diagnostic
- Delivery by CS if placenta within 2 cm of os
- Plan elective CS at 36 weeks if asymptomatic
This is a shared conversation. Sign in to Orris to start your own chat.