TORASEMIDE
Reading File
Finding Sources
Searching PubMed
torasemide torsemide clinical pharmacology
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to write a thorough response. Let me compile the full answer.
Torasemide (Torsemide)
Torasemide is a sulfonamide-based loop diuretic - the most efficacious class of diuretics currently available. It is structurally a pyridine-sulfonylurea compound, distinct from furosemide's sulfonamide-benzene ring but sharing the same target.
Mechanism of Action
Torasemide inhibits NKCC2 (the Na+/K+/2Cl- cotransporter, encoded by SLC12A1), located at the luminal membrane of the thick ascending limb (TAL) of Henle's loop. It binds from the luminal side (after tubular secretion), blocking cotransport of Na+, K+, and 2 Cl- into tubular cells.
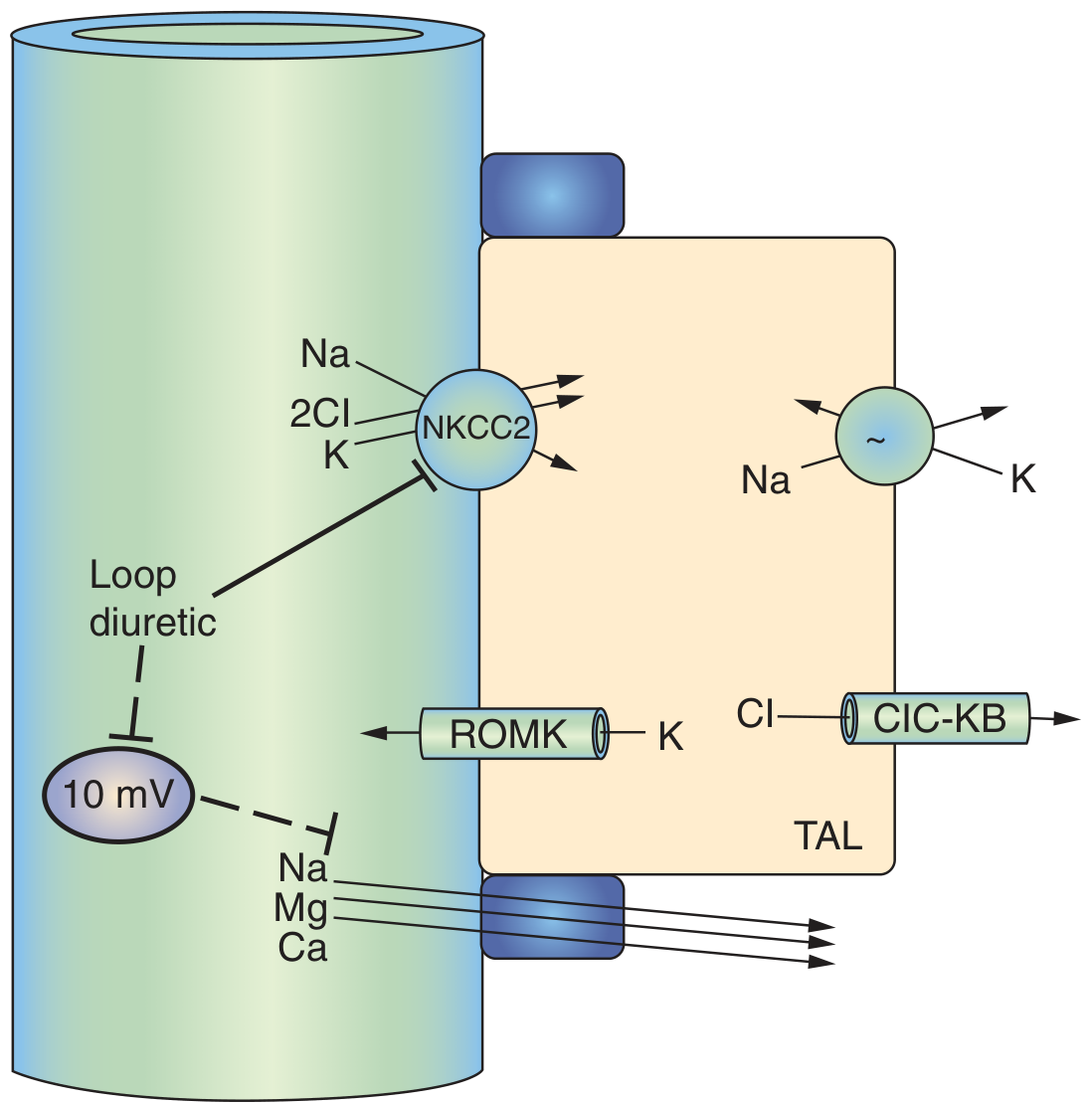
Fig. 50.3 - TAL cell model showing loop diuretic blockade of NKCC2. The transepithelial lumen-positive voltage (10 mV) is also reduced, which normally drives paracellular Na+, Mg2+, and Ca2+ reabsorption. (Brenner & Rector's The Kidney)
Secondary consequences of NKCC2 blockade:
-
Abolishes the lumen-positive transepithelial voltage generated by K+ recycling via ROMK channels
-
This voltage normally drives paracellular reabsorption of Na+, Mg2+, and Ca2+ - so all three are lost in urine
-
Eliminates the corticomedullary osmotic gradient, preventing urinary concentration
-
Stimulates COX-2 at the macula densa → PGE2 release → renin secretion (activates RAAS)
-
Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 406-407
-
Brenner & Rector's The Kidney, p. 2257-2259
Pharmacokinetics - Key Advantages Over Furosemide
| Parameter | Torasemide | Furosemide |
|---|---|---|
| Oral bioavailability | ~80-100% (consistent) | 10-90% (highly variable) |
| Absorption (oral) | Peak ~1 hour | Peak 2-3 hours |
| Duration of action | 4-6 hours | 2-3 hours |
| Elimination | Mainly hepatic (active metabolite with longer half-life) | Mainly renal |
| IV → oral switch | No dose change needed | Double the dose |
| Equivalent dose | 10 mg | 20 mg |
Key point: because torasemide and bumetanide are more completely absorbed than furosemide, switching from IV to oral does not require a dose adjustment - unlike furosemide, which often requires doubling. The variable bioavailability of furosemide is accentuated by food intake, a problem not seen with torasemide.
- Katzung's, p. 407; Brenner & Rector's, p. 2259
Dosage
| Route | Dose |
|---|---|
| Oral/IV | 5-20 mg/day (typical) |
| Equivalent dose | 10 mg torsemide ≈ 20 mg furosemide ≈ 0.5 mg bumetanide |
Pharmacodynamics & Unique Features
-
Anti-aldosterone effect: Torasemide (unlike furosemide) has a documented anti-aldosterone action, which may contribute to its lower incidence of hypokalemia at usual doses and potential benefit in cardiac remodeling.
-
Independent antihypertensive effect: May lower blood pressure beyond its diuretic action.
-
Prostaglandin interaction: Loop diuretics induce COX-2 expression → PGE2 synthesis, which participates in their tubular actions. NSAIDs (e.g., indomethacin) blunt this prostaglandin pathway and can reduce the diuretic response - significant in patients with nephrotic syndrome or cirrhosis.
-
Probenecid/NSAIDs interaction: Both compete for weak acid secretion in the proximal tubule, reducing tubular delivery of torasemide to its luminal site of action.
Clinical Indications
- Heart failure (acute and chronic) - drug of choice in many guidelines; superior to furosemide in two landmark clinical trials (TORIC study)
- Hepatic cirrhosis with ascites
- Nephrotic syndrome and edema
- Hypertension (less common - thiazides preferred as first-line)
- Hypercalcemia - combined with IV saline, enhances Ca2+ excretion
- Pulmonary arterial hypertension - used with anti-aldosterone agents
The TORIC study showed superior outcomes for torasemide vs. furosemide in chronic heart failure patients. A 2024 systematic review of torasemide pharmacokinetics confirmed its favorable and consistent PK profile (PMID 38176856).
Adverse Effects
| Effect | Mechanism | Notes |
|---|---|---|
| Hypokalemic metabolic alkalosis | Increased Na+ delivery to collecting duct → enhanced K+/H+ secretion | Most common; potassium supplementation may improve survival |
| Ototoxicity | Inhibits NKCC1 in the inner ear → disturbs endolymph ion composition | Dose-related, usually reversible; worse with concurrent aminoglycosides or renal failure |
| Hyperuricemia / Gout | Volume depletion → enhanced proximal tubule uric acid reabsorption | Prevented by avoiding hypovolemia |
| Hypomagnesemia | Loss of lumen-positive voltage → Mg2+ wasting | Occurs with chronic use; reversed by oral Mg2+ supplementation |
| Hypercalciuria / mild hypocalcemia | Loss of paracellular Ca2+ reabsorption | Can unmask occult hypercalcemia (e.g., malignancy) in volume-depleted patients |
| Allergic reactions | Sulfonamide base - rash, eosinophilia, rare interstitial nephritis | Less common than furosemide; note: ethacrynic acid is the non-sulfonamide alternative for true sulfonamide allergy |
| Severe dehydration/hypovolemia | Abolishes medullary concentration gradient | "Niagara effect" - torrential diuresis with short-duration dosing |
| Thiamine deficiency | Long-term use; relevant in heart failure patients | Worsens pre-existing deficiency |
| Renin/RAAS activation | Direct macula densa effect + volume depletion | Promotes secondary hyperaldosteronism |
- Katzung's, p. 408-409
Comparison: Torsemide vs. Furosemide
| Feature | Torsemide | Furosemide |
|---|---|---|
| Bioavailability | Consistent (~80%) | Variable (10-90%) |
| Half-life | Longer (active metabolite) | Shorter |
| Hypokalemia risk | Lower (anti-aldosterone effect) | Higher |
| IV→oral dose adjustment | Not needed | Double the dose |
| Heart failure outcomes | Superior (TORIC, DiNicolantonio) | Reference standard |
| Metabolism | Hepatic | Renal |
| Cost/availability | More expensive | Widely available |
Note: Although torsemide shows benefits in decreasing hospitalizations and possibly reducing AKI episodes in heart failure patients, no mortality benefit has been definitively shown compared to furosemide. - Katzung's, p. 407
Drug Interactions
- NSAIDs: Reduce diuretic efficacy via COX-2 inhibition and competition for proximal tubule secretion
- Aminoglycosides: Additive ototoxicity
- Probenecid: Reduces tubular secretion of torasemide
- ACE inhibitors/ARBs: Synergistic effect on BP; risk of first-dose hypotension
- Digoxin: Hypokalemia from loop diuretics potentiates digoxin toxicity
- Lithium: Reduce tubular reabsorption → reduce lithium levels (but volume depletion can also increase lithium toxicity)
Summary
Torasemide is a potent loop diuretic with a more predictable pharmacokinetic profile than furosemide, a longer duration of action (4-6 hours vs. 2-3 hours), and a lower risk of hypokalemia owing to its anti-aldosterone property. These advantages have positioned it as the preferred loop diuretic in chronic heart failure, though the mortality advantage over furosemide remains unproven. Its hepatic metabolism makes it particularly suitable when renal function is compromised.
Will there be increased urination
.
Yes, absolutely - increased urination (diuresis) is the primary intended effect of torasemide, not just a side effect.
Here is what happens:
Why urination increases:
Torasemide blocks the NKCC2 transporter in the thick ascending limb of Henle's loop, preventing reabsorption of Na+, K+, and Cl-. This means:
- More sodium stays in the tubule
- Water follows the sodium osmotically
- More urine is produced and excreted
What to expect practically:
- Diuresis typically begins within 1 hour of an oral dose (faster than furosemide)
- Peak effect is at around 1-2 hours
- The diuretic effect lasts 4-6 hours per dose
- This is sometimes called the "Niagara effect" - a torrential, short-burst diuresis
Timing matters:
- Most patients take it in the morning to avoid waking up at night to urinate (nocturia)
- Patients with prostate enlargement or stress incontinence can find the sudden, heavy diuresis particularly uncomfortable
The urine output is the goal:
In conditions like heart failure, liver cirrhosis, or edema, this increased urination is how the drug removes excess fluid from the body - reducing swelling, lowering blood pressure, and relieving congestion.
So yes - if someone starts torasemide, they should expect noticeably more frequent and higher-volume urination, especially in the first few hours after each dose.
This is a shared conversation. Sign in to Orris to start your own chat.