Vitamin a ,d,c and b12
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have rich data from the textbooks to compile a thorough answer. Let me put it all together.
Vitamins A, D, C, and B12 - A Comprehensive Overview
Vitamin A (Retinol)
Solubility: Fat-soluble
Forms: Retinol (animal sources), beta-carotene (plant precursor), retinal, retinoic acid
Functions
- Vision: Retinal is the functional form in photoreceptors. It combines with opsin to form rhodopsin in rod cells, which is essential for dim-light vision.
- Immunity: Maintains epithelial integrity; critical for mucosal immune defenses.
- Gene regulation: Retinoic acid acts as a ligand for nuclear receptors (RAR/RXR), regulating cell growth, differentiation, and embryogenesis.
- Skin and epithelium: Maintains the turnover of keratinized and mucus-secreting epithelial cells.
Dietary Sources
Liver, fish liver oils, dairy products, eggs (preformed vitamin A); carrots, sweet potatoes, leafy greens (beta-carotene).
Deficiency
- Night blindness (nyctalopia) - earliest sign; impaired rhodopsin regeneration reduces vision in dim light.
- Xerophthalmia - progressive corneal dryness and softening (keratomalacia) leading to blindness.
- Bitot's spots - white keratinized lesions on the conjunctiva.
- Increased susceptibility to infections; impaired bone growth in children.
- Leading cause of preventable blindness in the developing world.
- Ganong's Review of Medical Physiology; Wills Eye Manual
Toxicity (Hypervitaminosis A)
Vitamin A is the most important fat-soluble hepatotoxin when taken in excess. The average hepatotoxic dose in reported liver disease cases was nearly 100,000 IU/day over ~7 years. Even 25,000 IU/day for 6+ years can cause cirrhosis. Mechanisms include:
- Activation and hyperplasia of hepatic stellate cells (primary storage site), causing sinusoidal obstruction.
- Perisinusoidal fibrosis -> portal hypertension.
- Liver biopsy: characteristic greenish autofluorescence under UV light; "Swiss cheese" appearance from hypertrophied stellate cells compressing sinusoids.
- Water-soluble/emulsified preparations are up to 10x more toxic than oil-based forms.
- Because the liver half-life is 50 days to 1 year, fibrosis may progress even after stopping supplementation.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Vitamin D (Calciferol)
Solubility: Fat-soluble
Forms: D2 (ergocalciferol, plant/yeast) and D3 (cholecalciferol, animal/skin synthesis)
Synthesis and Metabolism
The diagram below shows the full pathway:
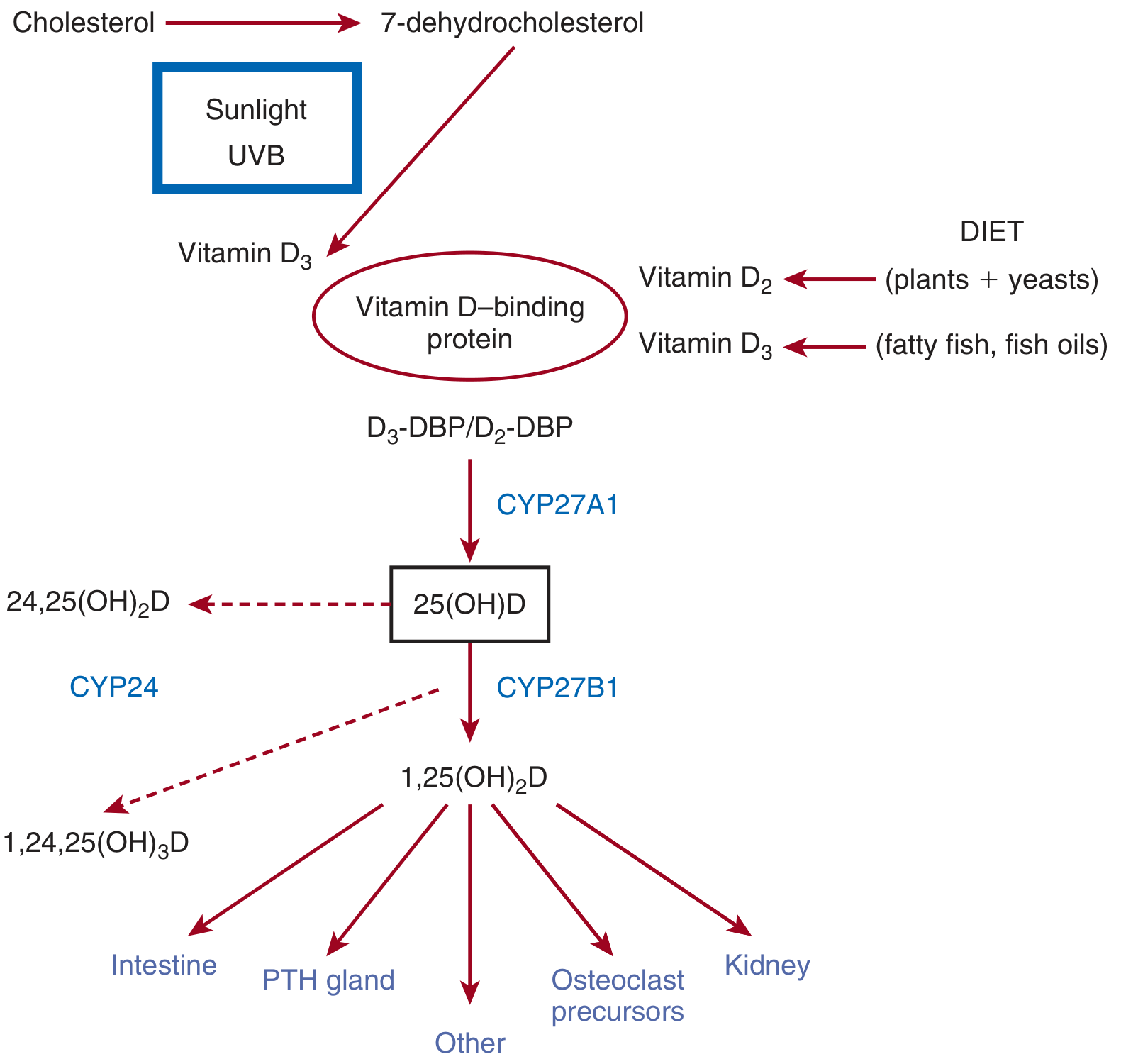
- Skin: Cholesterol -> 7-dehydrocholesterol -> Vitamin D3 (requires UVB sunlight). Melanin, sunscreen (SPF ≥8), and high latitude reduce this conversion.
- Liver: D2/D3 + Vitamin D-binding protein (DBP) -> 25(OH)D (calcidiol) via CYP27A1. This step is largely unregulated.
- Kidney: Calcidiol -> 1,25(OH)₂D (calcitriol) via CYP27B1. This is the active form and is tightly regulated by PTH, calcium, and phosphate.
Functions
- Promotes intestinal calcium and phosphate absorption.
- Regulates osteoclast activity (bone resorption/remodeling).
- Suppresses PTH secretion from the parathyroid glands.
- Acts on the kidney to enhance calcium reabsorption.
- Immune modulation, muscle function, cell differentiation (extrarenal synthesis).
Deficiency
- Children: Rickets (bowed legs, craniotabes, rachitic rosary).
- Adults: Osteomalacia (bone pain, proximal muscle weakness, fractures), hypocalcemia, tetany, seizures, low bone mineral density, osteoporosis.
At-risk populations: Elderly, exclusively breastfed infants, dark-skinned individuals, people with malabsorption (Crohn's, celiac), hepatic disease, chronic kidney disease, post-gastric surgery, high-altitude dwellers.
Toxicity
Upper tolerable intake limit: 4,000 IU/day (>9 years old). Toxicity typically from supplement over-ingestion. Causes hypercalcemia (nausea, vomiting, polyuria, nephrolithiasis, soft tissue calcification). Toxic levels are associated with serum 25(OH)D of 710-1587 nmol/L.
- Brenner and Rector's The Kidney; Yamada's Textbook of Gastroenterology
Vitamin C (Ascorbic Acid)
Solubility: Water-soluble
Functions
- Antioxidant - scavenges reactive oxygen species; regenerates vitamin E.
- Collagen synthesis - hydroxylates proline and lysine residues (essential for cross-linking); without it, collagen is unstable.
- Promotes non-heme iron absorption in the gut.
- Required for carnitine biosynthesis, dopamine -> norepinephrine conversion (dopamine-beta-hydroxylase), tyrosine catabolism, and peptide hormone synthesis.
- Histone and DNA demethylation (epigenetic role).
- Component of mixed-function oxidase drug-metabolizing systems.
Dietary Sources
Citrus fruits, broccoli, bell peppers, tomatoes, potatoes. Five servings of fruits/vegetables daily exceeds the RDA.
RDA: 90 mg/day (men), 75 mg/day (women). Requirements are increased by smoking, hemodialysis, pregnancy, lactation, and infection/trauma.
Absorption: Nearly 100% absorbed at doses <100 mg; drops to <50% at doses >1 g (excess is excreted in urine/feces).
Deficiency - Scurvy
Vitamin C deficiency (<10 mg/day) causes scurvy. Seen in poor/elderly populations, alcoholics, and those with severely restricted diets.
Clinical features:
- Perifollicular hemorrhages, petechiae, ecchymoses
- Inflamed and bleeding gums (gingivitis)
- Hemorrhage into joints, peritoneal cavity, pericardium, adrenal glands
- Impaired bone growth in children
- Generalized fatigue
Treatment: 200 mg/day of vitamin C resolves symptoms within days.
Other Uses
- High-dose supplementation may modestly reduce duration of upper respiratory infections.
- Useful in Chediak-Higashi syndrome and osteogenesis imperfecta.
- IV pharmacologic doses (up to 1 g/kg body weight) are under investigation for cancer treatment (metastatic pancreatic, ovarian, glioblastoma, NSCLC) - the mechanism is pro-oxidative, synergistic with gemcitabine and PD-1 inhibitors.
Toxicity
-
2 g in single dose: abdominal pain, diarrhea, nausea.
- Theoretical risk of oxalate kidney stones with chronic high-dose use; avoid in patients with history of oxalate stones or renal insufficiency.
- Possible risk of promoting iron overload in predisposed patients.
- Harrison's Principles of Internal Medicine 22E (2025)
Vitamin B12 (Cobalamin)
Solubility: Water-soluble
Forms: Cyanocobalamin (supplement), hydroxocobalamin, methylcobalamin, adenosylcobalamin (active forms)
Functions
- DNA synthesis - cofactor for thymidylate synthesis; deficiency causes megaloblastic anemia.
- Methylation reactions - methylcobalamin is a cofactor for methionine synthase (homocysteine -> methionine). Deficiency raises homocysteine.
- Fatty acid/odd-chain amino acid metabolism - adenosylcobalamin is a cofactor for methylmalonyl-CoA mutase; deficiency raises methylmalonic acid (MMA).
- Nerve myelination - B12 deficiency causes subacute combined degeneration of the spinal cord (posterior and lateral columns).
Absorption
B12 requires intrinsic factor (IF), secreted by gastric parietal cells, for absorption in the distal ileum. After absorption, it binds to transcobalamin II for blood transport to tissues. Intrinsic factor is degraded in ileal enterocytes but cobalamin itself is retained.
Causes of Deficiency
| Category | Examples |
|---|---|
| Lack of intrinsic factor | Pernicious anemia (autoimmune type A gastritis), gastrectomy, gastric bypass |
| Food cobalamin malabsorption | Atrophic gastritis, achlorhydria, exocrine pancreatic dysfunction |
| Ileal disorders | Crohn's disease, surgical resection, ileal conduit, Imerslund-Grasbeck syndrome |
| Usurpation (competition) | Bacterial overgrowth, blind loops, Diphyllobothrium latum, Giardia |
| Nutritional | Vegan/vegetarian diet, breastfed infant of deficient mother, poverty |
| Drug-induced | Metformin, PPIs, H2 blockers, nitrous oxide abuse |
| Inborn errors | Transcobalamin deficiency, CblC-J mutations (combined methylmalonic acidemia + homocystinuria) |
- Goldman-Cecil Medicine International Edition
Clinical Features of Deficiency
- Megaloblastic anemia (macrocytosis, hypersegmented neutrophils)
- Subacute combined degeneration (SCD) - demyelination of dorsal columns (loss of proprioception/vibration) and corticospinal tracts (spasticity, Babinski sign)
- Glossitis, angular stomatitis
- Elevated homocysteine AND methylmalonic acid (both elevated = B12 deficiency; only homocysteine elevated = folate deficiency)
- Neurological symptoms can occur without anemia in B12 deficiency - important clinical pearl.
Treatment
- IM hydroxocobalamin 1 mg/day for severe deficiency or pernicious anemia (since absorption requires IF which is absent).
- Oral high-dose cyanocobalamin (1000-2000 mcg/day) can be effective even without IF via passive diffusion, but IM is standard for pernicious anemia.
- Lifelong treatment required for pernicious anemia and post-total gastrectomy.
Quick Comparison Table
| Feature | Vitamin A | Vitamin D | Vitamin C | Vitamin B12 |
|---|---|---|---|---|
| Solubility | Fat | Fat | Water | Water |
| Key deficiency disease | Night blindness / Xerophthalmia | Rickets / Osteomalacia | Scurvy | Megaloblastic anemia / SCD |
| Key function | Vision, immunity | Calcium homeostasis, bone | Collagen synthesis, antioxidant | DNA synthesis, myelination |
| RDA (adult) | 700-900 mcg RAE | 600-800 IU | 75-90 mg | 2.4 mcg |
| Toxicity concern | Liver damage, teratogen | Hypercalcemia | Kidney stones (high dose) | Essentially non-toxic |
| Storage | Liver (large stores) | Adipose/liver | Minimal | Liver (2-5 year supply) |
Sources: Harrison's Principles of Internal Medicine 22E (2025); Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Brenner and Rector's The Kidney; Goldman-Cecil Medicine International Edition; Yamada's Textbook of Gastroenterology; Guyton and Hall Medical Physiology; Ganong's Review of Medical Physiology.
This is a shared conversation. Sign in to Orris to start your own chat.