Cough varient asthama 5 years old child iska full treatment btao with medicine name duration and doses according to mbbs medicine harrison or kd tripathi pharmacology book ke samjhao
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
cough variant asthma 5 year old child treatment salbutamol budesonide montelukast dose GINA guidelines pediatric
Loading Image
Reading File
Excellent! Now I have comprehensive data from Harrison's, Harriet Lane (pediatric doses), and GINA 2026. Let me compile the complete answer.
Cough Variant Asthma (CVA) - 5 Year Old Child: Complete Treatment Guide
(Harrison's 22E + KD Tripathi Pharmacology + GINA 2026 + Harriet Lane Pediatric Handbook)
CVA Kya Hai? (Definition)
Cough Variant Asthma wo asthma hai jisme sirf cough hoti hai - koi wheeze, dyspnea ya chest tightness nahi hoti. Yeh children mein adults se zyada common hai. Airway hyperresponsiveness hoti hai, cough often nocturnal hoti hai. (Harrison's 22E, p.317)
Harrison's: "Cough due to asthma in the absence of wheezing, shortness of breath, and chest tightness is referred to as 'cough-variant asthma.' It is common among children."
Diagnosis Confirm Karo Pehle
| Test | Finding |
|---|---|
| Spirometry (FEV1) | Reversible airflow obstruction (>12% improvement post-bronchodilator) |
| Methacholine challenge | Positive (confirms airway hyperresponsiveness) |
| Peak Flow monitoring | Variability >20% |
| Trial of treatment | Cough resolves with ICS + SABA - yeh bhi diagnostic hai |
| Trigger history | Allergen, exercise, cold air, URTIs se cough barhti hai |
STEPWISE TREATMENT APPROACH (NAEPP/GINA 2026 - Age 5 Years)
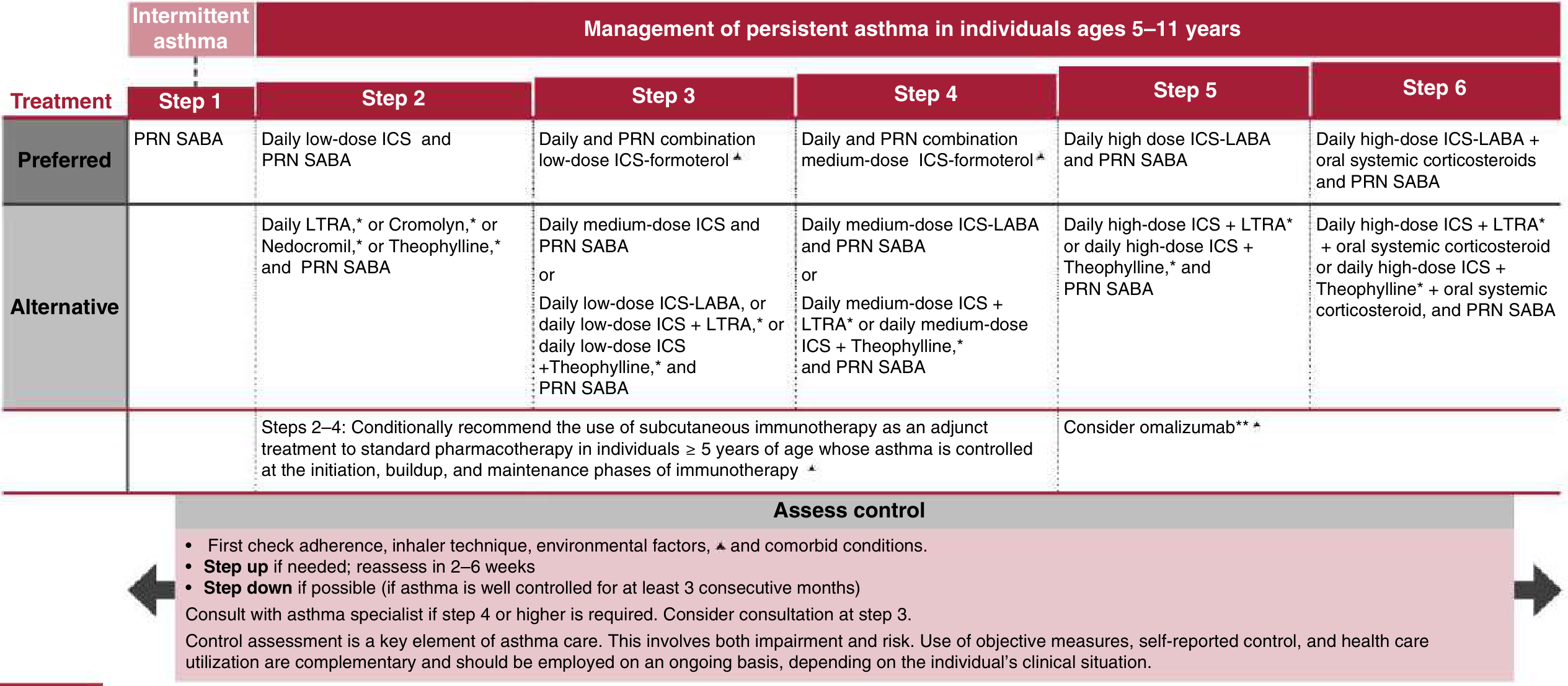
Harriet Lane Handbook 23e / NAEPP 2020 Updated Guidelines
CVA 5-Year-Old Ka Typical Classification
5 year ke child mein jo sirf cough hai = usually Mild Persistent Asthma → Step 2 se start karo.
MEDICINES - Names, Doses, Duration
STEP 1 - Intermittent CVA (symptoms <2 days/week)
Salbutamol (Albuterol) pMDI with Spacer - PRN (Reliever)
- Drug class: Short-acting Beta-2 agonist (SABA)
- Dose: 100 mcg/puff - 2 puffs (200 mcg) via pMDI + spacer
- Frequency: As needed, only when symptomatic
- Onset: 3-5 minutes, duration 4-6 hours
- Brand names (India): Asthalin, Ventolin, Salbutard
- KD Tripathi: Salbutamol stimulates β2 receptors → adenylyl cyclase → ↑cAMP → smooth muscle relaxation
Note: If child needs SABA more than 2 days/week, STEP UP to Step 2.
STEP 2 - Mild Persistent CVA (FIRST-LINE for most 5-year CVA children)
A) Inhaled Corticosteroid (ICS) - CONTROLLER (Preferred)
| Drug | Dose (Low Dose, Age ≤5 yrs) | Frequency | Duration |
|---|---|---|---|
| Budesonide (Pulmicort Respules) | 0.25-0.5 mg/day nebulized | Once daily or BD | Minimum 2-3 months to assess |
| Fluticasone propionate pMDI | 88 mcg/day (44 mcg x 2 puffs OD or 1 puff BD) | OD or BD | 2-3 months |
| Beclomethasone pMDI | 80-160 mcg/day | BD (2 puffs morning, 2 puffs evening of 40 mcg) | 2-3 months |
- Mechanism (KD Tripathi): ICS → binds glucocorticoid receptor → reduces inflammatory mediators (IL-4, IL-5, RANTES), reduces eosinophil recruitment, decreases mucosal edema and mucus hypersecretion
- Harrison's: "Cough-variant asthma typically responds well to inhaled glucocorticoids and intermittent use of inhaled beta-agonist bronchodilators"
- Side effects: Growth suppression (small), oral thrush (gargle after use, use spacer), hoarseness
- Duration of ICS treatment: At least 3 months trial; if well controlled for 3 consecutive months, consider step-down
B) PLUS Salbutamol PRN (same as Step 1)
STEP 2 ALTERNATIVE - Montelukast (LTRA) (If ICS concerns)
Montelukast (Singulair/Montair)
- Dose (Age 2-5 years): 4 mg chewable tablet once daily at bedtime
- Duration: 1-3 months; reassess
- Why use in 5-year-old: Harrison's clearly states - "Montelukast is frequently used in children with mild asthma due to concerns of ICS-related growth suppression"
- Mechanism: CysLT1 receptor antagonist → blocks leukotriene D4/C4/E4 → reduces bronchoconstriction, mucus, and eosinophilic inflammation
- FDA Warning (2020): Boxed warning for neuropsychiatric events (suicidal ideation) - counsel parents. Use when ICS not tolerated/accepted
- Not as effective as low-dose ICS - second choice (Katzung Pharmacology, per library)
STEP 3 - Moderate Persistent CVA (Symptoms daily, nighttime >1x/week)
Preferred: Daily Low-dose ICS + Formoterol (LABA) pMDI as maintenance AND reliever
| Drug | Dose |
|---|---|
| Budesonide/Formoterol (Symbicort) | 80/4.5 mcg - 1-2 puffs BD |
| Fluticasone/Salmeterol (Seretide) | 50/25 mcg - 1 puff BD |
Alternative Step 3:
- Medium-dose ICS alone: Budesonide 400 mcg/day + PRN SABA
- OR Low-dose ICS + Montelukast 4 mg OD + PRN SABA
ACUTE EXACERBATION (Cough suddenly worsening/attack)
Salbutamol (pMDI + spacer) - GINA 2026:
- Mild attack: 4 puffs (400 mcg) via pMDI+spacer, repeat once after 30-60 min if needed
- Moderate attack: 4 puffs every 20 minutes x 3 doses
- Nebulization: Salbutamol 2.5 mg in 3 mL normal saline via nebulizer
- If not improving → add Ipratropium 4 puffs (0.5 mg nebule) with each salbutamol dose x 3
Oral Prednisolone (for exacerbations):
- Dose: 1-2 mg/kg/day (max 30 mg for child 2-5 years)
- Duration: 3-5 days
- Form: Syrup or dispersible tablet
- Brand (India): Wysolone, Omnacortil
COMPLETE DRUG SUMMARY TABLE
| Drug | Class | Route | Dose (5 yr child) | Frequency | Duration |
|---|---|---|---|---|---|
| Salbutamol (Asthalin) | SABA | pMDI+spacer | 200 mcg (2 puffs) | PRN | As needed |
| Salbutamol | SABA | Nebulization | 2.5 mg | PRN q20 min (acute) | Acute use |
| Budesonide (Pulmicort) | ICS | Nebulization | 0.25-0.5 mg/day | OD or BD | Min. 3 months |
| Fluticasone (Flohale) | ICS | pMDI+spacer | 88 mcg/day | BD | Min. 3 months |
| Beclomethasone | ICS | pMDI | 80-160 mcg/day | BD | Min. 3 months |
| Montelukast (Montair) | LTRA | Oral | 4 mg | OD at bedtime | 1-3 months, reassess |
| Prednisolone (Wysolone) | OCS | Oral | 1-2 mg/kg/day | OD (max 30 mg) | 3-5 days (exacerbation) |
| Ipratropium (Ipravent) | SAMA | Nebulization | 0.25 mg | With salbutamol in moderate-severe attack | Acute use |
TREATMENT DURATION SUMMARY
| Severity | Treatment | Duration |
|---|---|---|
| Intermittent | PRN SABA only | As needed; no daily medication |
| Mild persistent | ICS (low dose) daily + PRN SABA | Minimum 3 months, then reassess |
| If well-controlled for 3 months | Step down (reduce ICS dose) | Every 3 months review |
| Exacerbation | Prednisolone burst | 3-5 days only |
INHALER TECHNIQUE - 5 Year Old Ke Liye
At 5 years, pMDI + Spacer with mask or mouthpiece preferred:
- Metered-dose inhaler (pMDI) alone is NOT effective in young children without spacer
- Nebulization is acceptable alternative for controller therapy (Budesonide respules)
- Child should rinse mouth/gargle after ICS use to prevent oral candidiasis
MONITORING & FOLLOW-UP
- 2-4 weeks - Initial response check
- Every 2-3 months - Assess control, step up or step down
- Peak flow monitoring at home (if feasible)
- Watch for ICS growth suppression - measure height every 6 months
- Identify and avoid triggers: dust mites, pet dander, cold air, URTIs, smoke
IMPORTANT POINTS (Harrison's + KD Tripathi)
- CVA is the most common cause of chronic cough in children
- Objective testing (spirometry, methacholine challenge) confirms diagnosis; if child is <5 years and spirometry not feasible, therapeutic trial of ICS is diagnostic
- ICS is the cornerstone - reduces airway inflammation, not just bronchospasm
- Never prescribe LABA alone without ICS in children (risk of asthma death)
- Theophylline can be used as alternative but narrow therapeutic window and monitoring needed (blood levels 10-15 mcg/mL) - rarely preferred in children today
- Montelukast FDA 2020 boxed warning: inform parents about behavioral side effects
Sources: Harrison's Principles of Internal Medicine 22E (2025) p.317, 2267-2268 | Harriet Lane Handbook 23e (NAEPP 2020 Stepwise Chart) | Goodman & Gilman / Katzung Pharmacology | GINA 2026 Strategy Report | KD Tripathi Pharmacology (Beta-2 agonists, ICS mechanisms)
This is a shared conversation. Sign in to Orris to start your own chat.