Stroke classification diagnosis management
"ischemic stroke" AND "management"
Stroke: Classification, Diagnosis, and Management
Overview
Classification

1. Ischemic Stroke (~80%)
| Subtype | Proportion | Mechanism |
|---|---|---|
| Thrombotic (large-vessel) | ~1/3 | Atherosclerotic plaque ulceration + clot at vessel bifurcations (ICA most common) |
| Lacunar (small-vessel) | ~1/4 | Lipohyalinosis of penetrating arteries; basal ganglia, thalamus, pons, internal capsule; 80-90% have HTN |
| Cardioembolic | ~1/4 | Atrial fibrillation is most common (5x risk); also mural thrombus, valvular disease |
| Cryptogenic | >1/3 | No clear cause identified |
- Carotid/vertebral dissection (leading determined cause in the young - may follow minor trauma, sneezing, yoga, spinal manipulation)
- Antiphospholipid syndrome, protein C/S deficiency
- Oral contraceptives, pregnancy
- Sickle cell anemia, polycythemia
- Fibromuscular dysplasia
- Cocaine/amphetamine vasospasm
- Varicella or fungal vasculopathy
Transient Ischemic Attack (TIA)
2. Hemorrhagic Stroke (~20%)
- Risk factors: hypertension (most common), older age, Black/Asian race, high alcohol use, low LDL/triglycerides
- Causes: hypertension, cerebral amyloid angiopathy (CAA in elderly), AVM, coagulopathy, anticoagulant use, tumor, cocaine
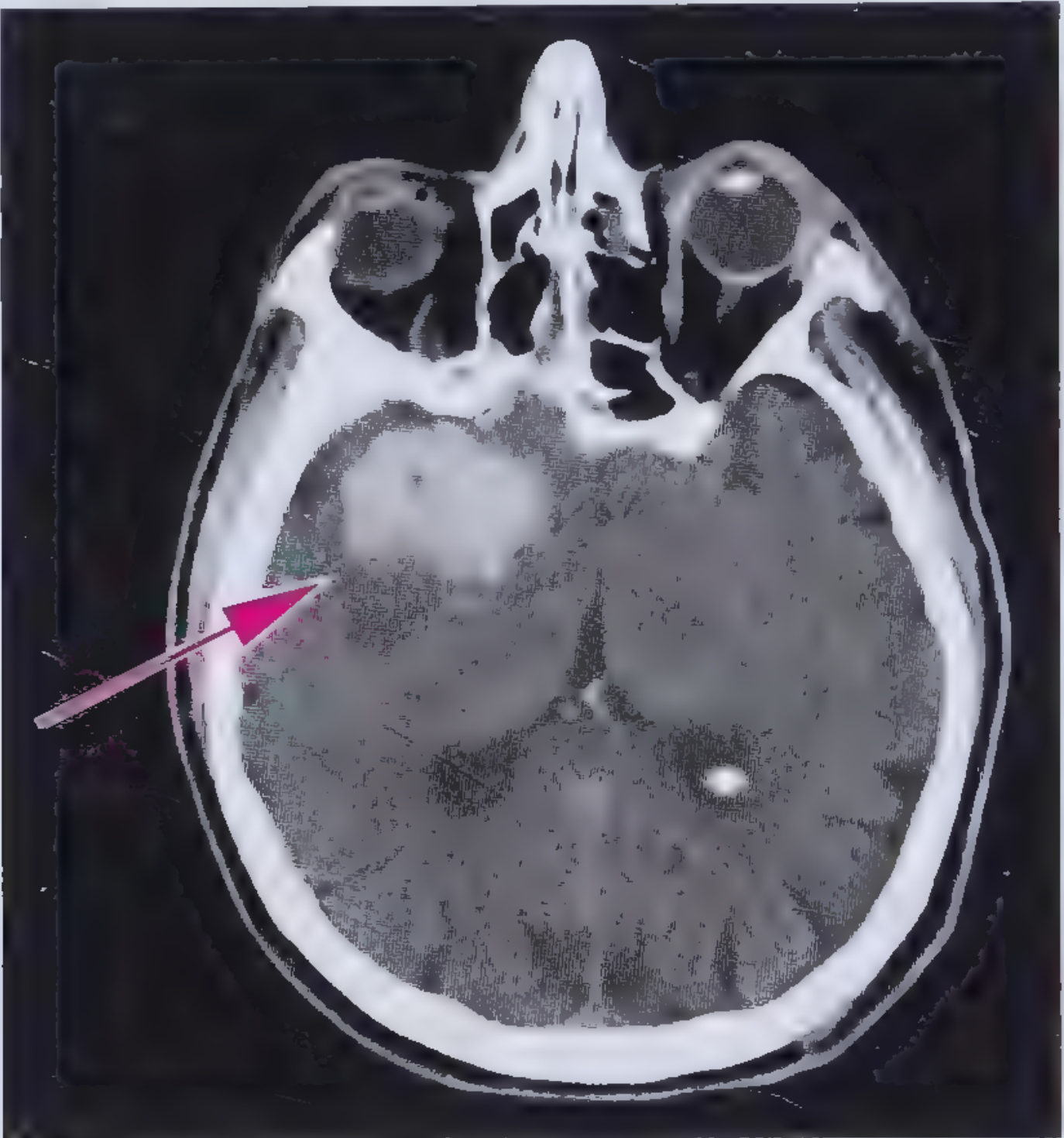
- CT appearance: round/oval hyperdense lesion (40-60 HU early, 80-100 HU over days)
- Bleeding between arachnoid and pia mater
- Classic: thunderclap headache ("worst headache of my life"), ruptured aneurysm
- CT may miss; LP shows xanthochromia if CT negative
Stroke Mimics (Differential Diagnosis)
- Hypoglycemia (most important - can mimic stroke for days)
- Todd's paralysis (postictal focal weakness)
- Subdural/epidural hematoma
- Brain tumor or abscess
- Complex migraine with aura
- Wernicke encephalopathy (ophthalmoplegia + ataxia + confusion mimics cerebellar stroke)
- Bell's palsy, vestibular neuronitis, Ménière disease
- Giant cell arteritis
Diagnosis
Immediate Evaluation (NINDS Target Times)
| Step | Target Time |
|---|---|
| Door to physician | 10 min |
| Door to CT completion | 25 min |
| Door to CT interpretation | 45 min |
| Door to treatment | 60 min |
| Neurology access | 15 min |
| Neurosurgery access | 2 hours |
Neuroimaging
- Immediately distinguishes ischemic from hemorrhagic stroke
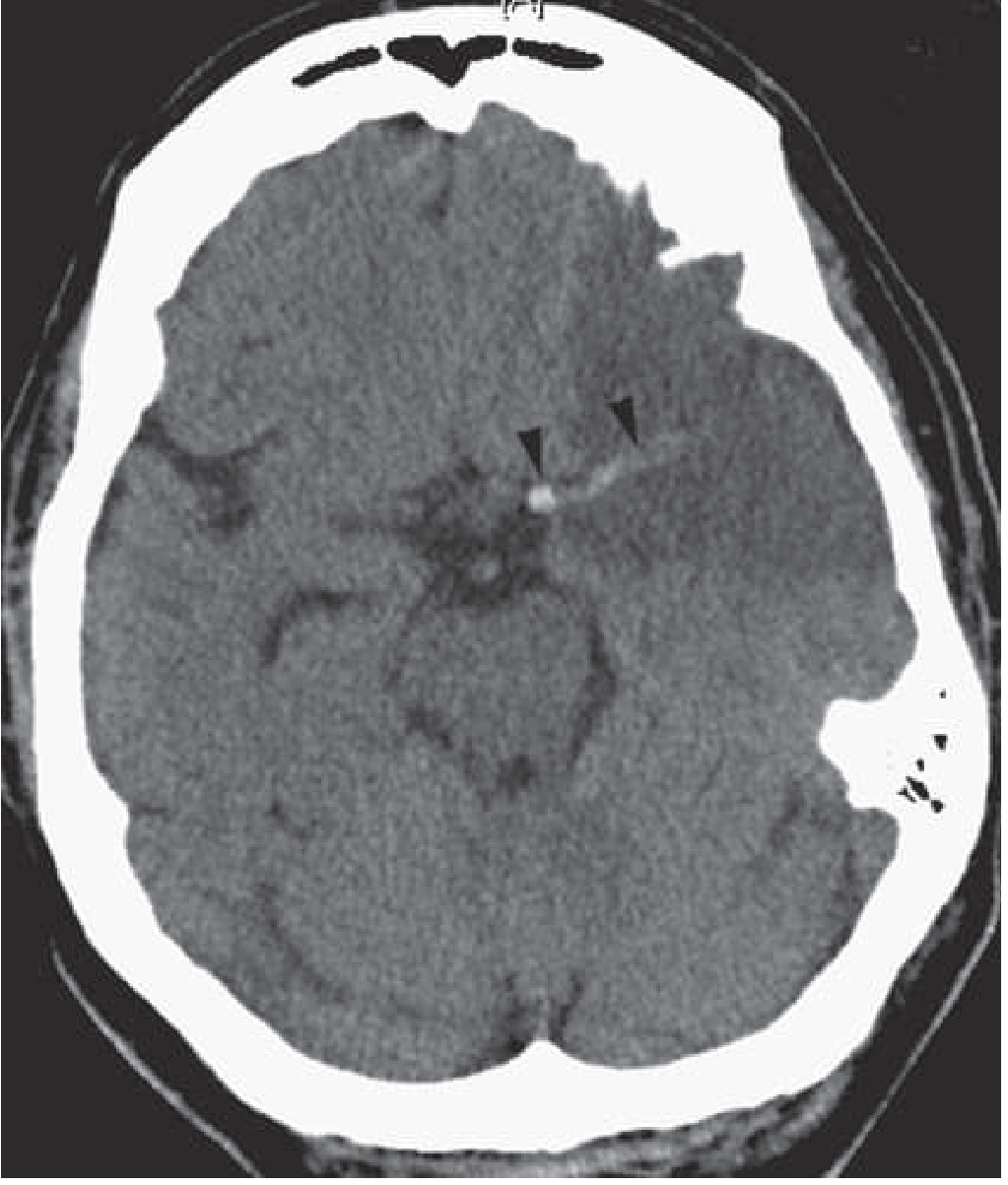
- Highly sensitive for parenchymal hemorrhage >1 cm and SAH
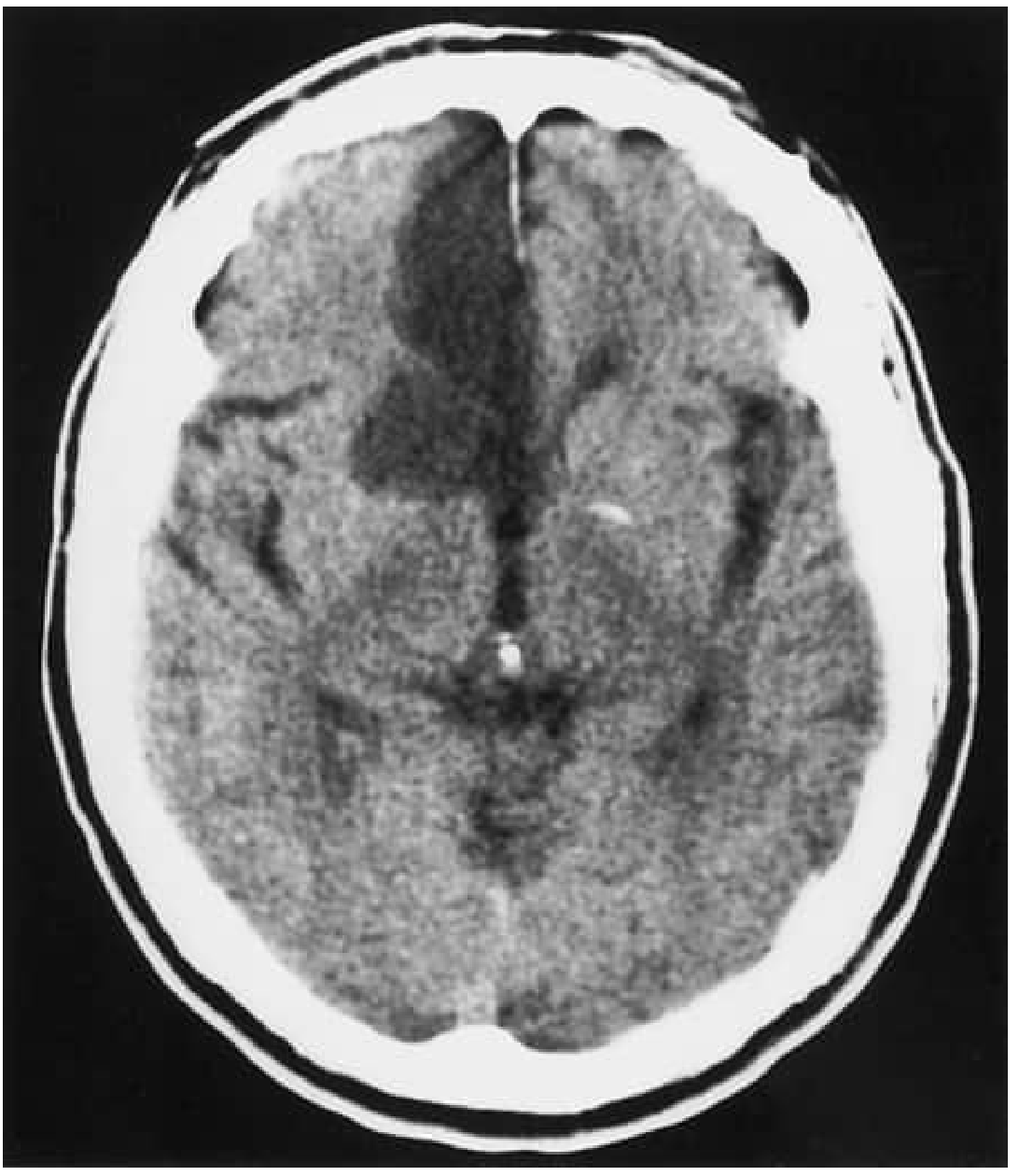
- Early ischemic changes (within 3 hours): hyperdense artery sign, sulcal effacement, loss of insular ribbon, gray-white interface loss, acute hypodensity (seen in up to 67% within 3 hours)
- Gross infarct signs typically not visible for 6-12 hours
- Run concurrently with CT head
- Identifies large vessel occlusion (LVO) for thrombectomy triage
- Also detects dissection, stenosis
- Identifies salvageable penumbra in extended time windows (6-24 hours)
- Generally not needed in first 6 hours
- Much higher sensitivity for ischemic stroke than CT, especially posterior fossa and within first hours
- DWI-FLAIR mismatch: DWI-positive + FLAIR-negative = stroke likely within ~4.5 hours (useful for "wake-up" strokes)
- Standard imaging for thrombectomy in 6-24 hour window (DAWN/DEFUSE-3 protocols)
Other Workup
- ECG - identify AF and acute MI
- Blood glucose - immediately (hypo/hyperglycemia mimics stroke)
- CBC, coagulation studies, BMP, troponin
- Echocardiography - cardioembolic source
- Carotid duplex / CTA neck - stenosis, dissection
- Cardiac monitoring (48-72h or longer) - paroxysmal AF detection
Management
A. General Supportive Care (All Stroke Types)
- Airway/Breathing/Circulation - supplemental O2 only if SpO2 <94%
- IV access - avoid overhydration (cerebral edema risk); use isotonic saline; avoid dextrose solutions in normoglycemic patients
- Temperature - treat fever (>38°C) aggressively; even mild hyperthermia worsens neurologic injury
- Blood glucose - target 140-180 mg/dL; treat hypoglycemia (<60 mg/dL) with IV dextrose
- Swallowing assessment - NPO until evaluated (aspiration risk)
- Document exact time of last known well - determines eligibility for reperfusion
B. Ischemic Stroke Management
Blood Pressure
- Without thrombolysis: withhold antihypertensives unless SBP >220 mmHg, DBP >120 mmHg, or MAP >130 mmHg (permissive hypertension preserves penumbral perfusion)
- Before thrombolysis: lower to <185/110 mmHg before starting tPA
- After thrombolysis: maintain <180/105 mmHg for 24 hours; monitor BP every 15 min during infusion, then every 30 min for 6h, then hourly for 16h
- Labetalol 10-20 mg IV over 1-2 min (may repeat once)
- Nicardipine infusion 5 mg/h, titrate by 2.5 mg/h every 5-15 min (max 15 mg/h)
- Clevidipine 1-2 mg/h IV, double dose every 2-5 min (max 21 mg/h)
Reperfusion Therapy
- Dose: 0.9 mg/kg IV (max 90 mg); 10% as bolus over 1 min, remainder over 60 min
- Time window: within 3 hours (FDA-approved); up to 4.5 hours for eligible patients
- Contraindications include: recent surgery, active bleeding, prior ICH, BP consistently >185/110 mmHg (untreated), INR >1.7, heparin use within 48h with elevated aPTT, glucose <50 or >400 mg/dL
- Single IV bolus, simpler administration; approved as alternative
- Dose: 0.25 mg/kg IV (max 25 mg)
- For large vessel occlusion (LVO) confirmed on CTA (ICA, M1/M2 MCA, basilar artery)
- Time window: 0-6 hours (standard); 6-24 hours in selected patients with favorable penumbra imaging (DAWN/DEFUSE-3 criteria: target mismatch on CTP or DWI/PWI-MRI)
- Maintain BP ≤185/110 mmHg pre-procedure (if no prior IV tPA)
- Give IV tPA first if eligible; do NOT delay tPA to wait for thrombectomy
Antiplatelet Therapy
- Aspirin 325 mg within 24-48 hours of ischemic stroke (not within 24h of tPA)
- For minor stroke / high-risk TIA: dual antiplatelet (aspirin + clopidogrel) for 21 days (POINT/CHANCE trial evidence)
- Anticoagulation for cardioembolic stroke (AF): start after 4-14 days depending on stroke size; DOAC preferred over warfarin
C. Hemorrhagic Stroke Management
Intracerebral Hemorrhage (ICH)
- Reverse coagulopathy immediately: elevated INR - give vitamin K + 4-factor PCC (or FFP); dabigatran - idarucizumab; Xa inhibitors - andexanet alfa
- Blood pressure: if SBP 150-220 mmHg, acute lowering to target SBP 140 mmHg is safe and reasonable; reduces hematoma expansion
- Seizure prophylaxis: treat clinical seizures with antiepileptics; prophylactic treatment controversial
- Intracranial pressure management if elevated: HOB elevation 30°, hypertonic saline, osmotic therapy (mannitol), intubation/sedation, hemicraniectomy in refractory cases
- Glucose management: avoid hyper- and hypoglycemia
- Surgical evacuation: consider for cerebellar hemorrhage >3 cm, or accessible lobar clot with deterioration; deep basal ganglia hemorrhage generally not operated (no mortality benefit)
| Feature | Points |
|---|---|
| GCS 3-4 | 2 |
| GCS 5-12 | 1 |
| GCS 13-15 | 0 |
| ICH volume >30 mL | 1 |
| Intraventricular hemorrhage | 1 |
| Infratentorial origin | 1 |
| Age >80 | 1 |
Subarachnoid Hemorrhage (SAH)
- Neurosurgical/neurovascular emergency
- Secure aneurysm (coiling or clipping) early
- Nimodipine 60 mg q4h for 21 days (reduces vasospasm-related deficit)
- Monitor for hydrocephalus (external ventricular drain)
- Triple-H therapy (hypertension, hypervolemia, hemodilution) for delayed cerebral ischemia (vasospasm)
Stroke Risk Factors and Secondary Prevention
- Hypertension (strongest risk factor - present in most stroke patients; SBP ≥140 or DBP ≥90 mmHg)
- Atrial fibrillation (~5x risk)
- Diabetes mellitus
- Dyslipidemia
- Smoking
- Physical inactivity
- Antiplatelet therapy (aspirin, clopidogrel, or aspirin + dipyridamole)
- Anticoagulation for AF (DOAC preferred)
- Statin therapy (high-intensity)
- Carotid endarterectomy or stenting if symptomatic stenosis >50% (CEA preferred for >70%)
- BP control (target <130/80 mmHg)
- Lifestyle modification
Prognosis
| Timeframe | Mortality |
|---|---|
| 30-day (overall) | ~10% |
| 30-day (ICH) | ~50% |
| 1-year | ~20% |
| 5-year | ~40% |
Clinical features
Clinical Features of Stroke
General Presenting Features
- Unilateral face/arm/leg weakness or numbness
- Speech difficulty (aphasia or dysarthria)
- Visual disturbance (monocular loss, hemianopia, diplopia)
- Severe headache (especially hemorrhagic stroke - "worst ever")
- Vertigo, ataxia, imbalance
- Altered consciousness or confusion
Anterior Circulation Syndromes
Internal Carotid Artery (ICA)
- Ipsilateral amaurosis fugax - transient monocular blindness from emboli to the ophthalmic artery (this distinguishes ICA from pure MCA syndrome)
- Contralateral hemiplegia, hemisensory loss
- Homonymous hemianopia
- Aphasia if dominant hemisphere
Middle Cerebral Artery (MCA) - Most Common Stroke Territory
| MCA Division | Clinical Features |
|---|---|
| Stem (complete MCA) | Contralateral hemiplegia, hemianesthesia, homonymous hemianopia; conjugate ipsilateral eye deviation; global aphasia (dominant) or hemineglect (non-dominant) |
| Upper division | Face and arm > leg weakness; Broca's aphasia (dominant) - non-fluent speech, poor repetition, intact comprehension; impaired prosody (non-dominant) |
| Lower division | Wernicke's aphasia (dominant) - fluent but meaningless speech, poor comprehension; behavioral disturbances (non-dominant); homonymous hemianopia |
| Lenticulostriate branches | Pure motor hemiparesis from internal capsule lacune (subcortical - no aphasia, no sensory loss) |
- Alexia with agraphia (angular gyrus)
- Gerstmann syndrome (left angular/parietal gyrus): finger agnosia + acalculia + right-left disorientation + agraphia
- Conduction aphasia, transcortical aphasia (depending on extent)
- Anosognosia (denial of hemiparesis, more common with right hemisphere lesions)
- Hemi-inattention, tactile and visual extinction
- Anosognosia, anosodiaphoria
- Apraxia, impaired prosody
- Acute agitated delirium (rarely)
Anterior Cerebral Artery (ACA) - <3% of infarcts
- Contralateral leg > arm weakness (the leg is represented medially, which is ACA territory)
- Discriminative and proprioceptive sensory loss (lower extremity)
- Abulia (reduced motivation, flat affect)
- Akinetic mutism with bilateral mesiofrontal damage
- Transcortical motor aphasia (dominant hemisphere)
- Left arm apraxia (anterior corpus callosum disconnection)
- Sphincter incontinence
- Paratonia (gegenhalten)
Anterior Choroidal Artery
- Hemiparesis (posterior limb of internal capsule)
- Hemisensory loss (posterolateral thalamus or thalamocortical fibers)
- Hemianopia (lateral geniculate body or geniculo-calcarine tract) - with characteristic sparing of the horizontal meridian
Lacunar Syndromes (Small-Vessel / Deep Perforator Occlusion)
| Syndrome | Key Features | Common Location |
|---|---|---|
| Pure Motor Hemiparesis | Contralateral face, arm, and leg weakness + dysarthria; NO sensory/visual/cortical signs | Posterior limb internal capsule, basis pontis, corona radiata |
| Pure Sensory Stroke | Paresthesia, numbness, unilateral hemisensory loss (all modalities) | VPL/VPM thalamus |
| Sensorimotor Stroke | Motor + sensory deficit combined | Posterior internal capsule + thalamus |
| Ataxic Hemiparesis | Hemiparesis + ipsilateral limb ataxia (cerebellar signs on same side as weakness) | Posterior internal capsule or basis pontis |
| Dysarthria - Clumsy Hand Syndrome | Supranuclear facial weakness + dysarthria + dysphagia + loss of fine hand motor control + Babinski sign | Deep basis pontis |
Posterior Circulation Syndromes
Posterior Cerebral Artery (PCA)
| Feature | Mechanism |
|---|---|
| Contralateral homonymous hemianopia (often with macular sparing) | Striate cortex / optic radiations infarction |
| Superior quadrantanopia | Striate cortex inferior to calcarine / inferior optic radiations |
| Inferior quadrantanopia | Superior to calcarine / superior optic radiations |
| Alexia without agraphia | Left occipital lobe + splenium of corpus callosum (can write, cannot read) |
| Visual hallucinations (formed or unformed) | Occipital cortex |
| Prosopagnosia, color agnosia | Occipital/temporal |
| Dejerine-Roussy syndrome | Contralateral sensory loss + thalamic pain (severe dysesthesias) + choreoathetosis + transient hemiparesis |
| Anton syndrome | Bilateral occipital - cortical blindness with denial/unawareness of blindness |
| Balint syndrome | Bilateral parieto-occipital - optic ataxia + optic apraxia + simultanagnosia |
| Global amnesia | Left medial temporal or bilateral mesiotemporal involvement |
Thalamic Infarction
| Region | Features |
|---|---|
| Posterolateral (thalamogeniculate a.) | Pure sensory stroke, sensorimotor stroke, Dejerine-Roussy syndrome |
| Anterior (polar/tuberothalamic a.) | Memory impairment, emotional disturbances, dysphasia (left) or neglect (right) |
| Paramedian | Classic triad: decreased consciousness + memory loss + vertical gaze palsy |
| Dorsal (posterior choroidal a.) | Homonymous quadrantanopia or horizontal sectoranopsia |
| Bilateral (artery of Percheron) | Bilateral thalamic infarction: coma, amnesia, vertical gaze palsy |
Cerebellar Syndromes
| Artery | Syndrome | Features |
|---|---|---|
| PICA (medial branch) | Vestibulocerebellar | Prominent vertigo, ataxia, nystagmus |
| PICA (lateral branch) | - | Vertigo, gait ataxia, limb dysmetria, nausea/vomiting, conjugate gaze palsies, dysarthria |
| PICA / Vertebral artery | Wallenberg (lateral medullary) syndrome | Ipsilateral: Horner syndrome, facial pain/temperature loss, palate/pharynx/cord weakness, cerebellar ataxia. Contralateral: hemibody pain/temperature loss |
| AICA | Lateral inferior pontine | Ipsilateral: facial palsy, facial sensory loss, corneal hyesthesia, deafness, Horner, ataxia. Contralateral: hemibody pain/temperature loss |
| SCA | Dorsal cerebellar | Ipsilateral: Horner, nystagmus, ataxia, intention tremor. Contralateral: hearing loss, hemibody hypalgesia. Vertigo less prominent than PICA |
Brainstem Syndromes
Midbrain
| Syndrome | Features |
|---|---|
| Weber | Ipsilateral CN III palsy (dilated pupil, ptosis, "down and out" eye) + contralateral hemiplegia |
| Benedikt | Ipsilateral CN III palsy + contralateral involuntary movements (tremor, hemiballismus, hemichorea) - red nucleus involvement |
| Claude | Ipsilateral CN III palsy + contralateral cerebellar signs (more dorsal than Benedikt) |
| Parinaud | Supranuclear upward gaze paralysis + convergence-retraction nystagmus + pupillary light-near dissociation + lid retraction |
| Top of basilar | Somnolence, peduncular hallucinosis, memory disturbances, ocular motor abnormalities, hemianopia or cortical blindness |
Pons
| Syndrome | Features |
|---|---|
| Locked-in syndrome (bilateral ventral pons) | Quadriplegia + aphonia + loss of horizontal gaze; preserved consciousness; vertical eye movement and blinking intact |
| Lateral inferior pontine (AICA) | Ipsilateral: facial palsy, facial sensory loss, conjugate gaze palsy, deafness, tinnitus, ataxia. Contralateral: hemibody pain/temperature loss |
| Medial inferior pontine (paramedian basilar branch) | Ipsilateral: conjugate gaze palsy, abducens palsy, nystagmus, ataxia. Contralateral: hemibody tactile/proprioceptive loss + hemiparesis |
Medulla
| Syndrome | Features |
|---|---|
| Lateral medullary (Wallenberg) | Vertebral artery >> PICA. Ipsilateral: Horner, facial pain/temp loss, palatal/pharyngeal/laryngeal weakness, ataxia. Contralateral: hemibody pain/temp loss |
| Medial medullary (Dejerine) | Ipsilateral: lower motor neuron tongue paralysis (tongue deviates to lesion side). Contralateral: hemiparesis (face spared) + loss of tactile/vibratory/position sense |
Watershed (Border Zone) Infarctions
| Territory | Clinical Picture |
|---|---|
| ACA/MCA bilateral | "Man in a barrel" - bilateral proximal arm weakness with preserved leg function; impaired saccadic eye movements |
| MCA/PCA bilateral | Bilateral parieto-occipital - cortical blindness, dyslexia, dyscalculia, memory deficits |
| ACA/MCA/PCA | Bilateral lower visual field defects, optic ataxia, cortical blindness |
Hemorrhagic Stroke: Clinical Clues
- Sudden, severe headache at onset ("thunderclap")
- Rapid progression to coma or obtundation
- Vomiting at onset
- Very high blood pressure at presentation
- Stiff neck (suggests SAH)
- Onset during exertion
NIHSS Assessment
- Mild: NIHSS 1-4
- Moderate: NIHSS 5-15
- Severe: NIHSS 16-20
- Very severe: NIHSS >20
Diagnosis n investigation
Stroke: Diagnosis and Investigations
Step 1 - Immediate Bedside Evaluation (Before Imaging)
| Intervention | Rationale |
|---|---|
| Airway, Breathing, Circulation | Immediately identify and manage life threats |
| IV access | Needed for thrombolytics - do not delay imaging for this |
| Pulse oximetry | Detect hypoxia; O2 only if SpO2 <94% (routine O2 not indicated) |
| Bedside blood glucose | First and most important test - hypoglycemia (<60 mg/dL) is the #1 stroke mimic and is immediately treatable with IV dextrose |
| Cardiac monitoring (ECG telemetry) | Atrial fibrillation is common; dysrhythmias including AF predict 3-month mortality |
| Record exact last-known-well time | Determines eligibility for reperfusion therapy |
| NIHSS score | Quantify deficit severity at baseline; document neurologic trajectory |
Step 2 - Emergency Brain Imaging
A. Non-Contrast CT Head (NCCT) - FIRST-LINE
| Finding | Significance |
|---|---|
| Hyperdense artery sign | Acute intraluminal thrombus (e.g., "hyperdense MCA sign," "hyperdense dot sign") |
| Loss of gray-white interface | Early ischemic swelling - present in up to 67% within 3 hours |
| Sulcal effacement | Cytotoxic edema |
| Loss of insular ribbon | MCA territory ischemia |
| Acute hypodensity | Established infarct - if >1/3 MCA territory, increased ICH risk with tPA |
| No early changes | Common in first 6-12 hours (sensitivity ~50%); does NOT exclude ischemia |
| Finding | Significance |
|---|---|
| Hyperdense parenchymal lesion | ICH - round/oval, 40-60 HU early, 80-100 HU within days; identifies virtually all hemorrhages >1 cm |
| Blood in subarachnoid cisterns | SAH - check basal cisterns, sylvian fissures |
| Intraventricular blood | Ventricular extension - worsens prognosis |
| Midline shift, mass effect | Indicates degree of herniation risk |
- Low sensitivity for posterior fossa ischemia (skull base streak artifacts)
- Cannot detect ischemia in first few hours
- Cannot identify penumbra or tissue viability
B. CT Angiography (CTA) - Run Concurrently with CT Head
- Identifies large vessel occlusion (LVO) - M1/M2 MCA, ICA, basilar artery - triage for thrombectomy
- Detects vessel dissection (carotid or vertebral)
- Identifies stenosis, aneurysm (cause of SAH)
- Hyperdense dot sign on CTA correlates with proximal occlusion
C. CT Perfusion (CTP)
- Extended time window (6-24 hours) - DAWN and DEFUSE-3 trial criteria
- Unknown onset "wake-up strokes"
- Not routinely needed in the first 6 hours
- CBF (cerebral blood flow) - reduced in ischemia
- CBV (cerebral blood volume) - core infarct has reduced CBV; penumbra may maintain CBV
- MTT/Tmax - prolonged in ischemic tissue
- Core vs. penumbra mismatch - core = irreversible damage; penumbra = salvageable tissue
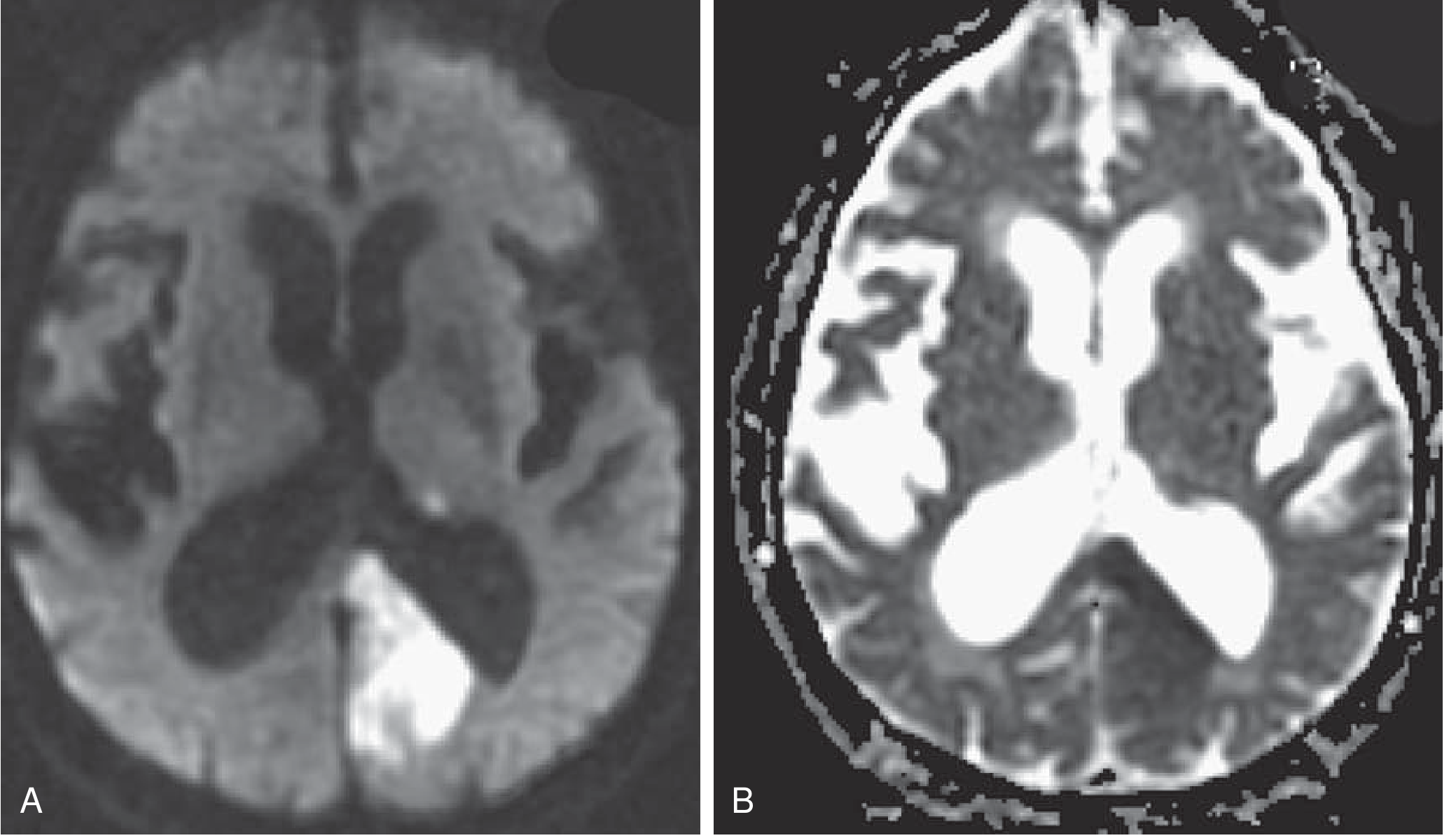
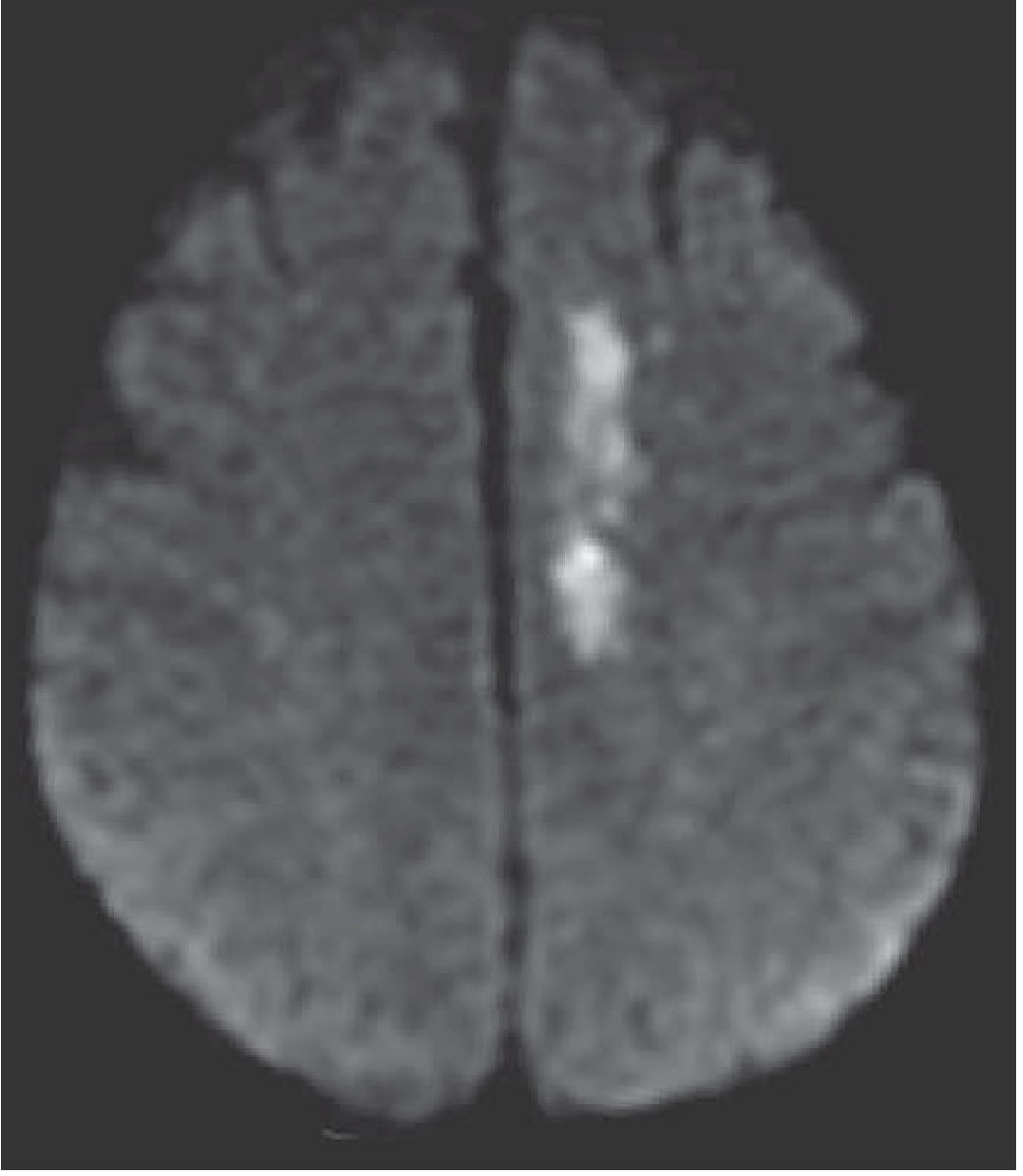
D. MRI Brain - Superior Sensitivity for Ischemia
- Posterior fossa / brainstem lesions
- Small lacunar infarcts
- Within the first few hours
| Sequence | What it Shows | Timing |
|---|---|---|
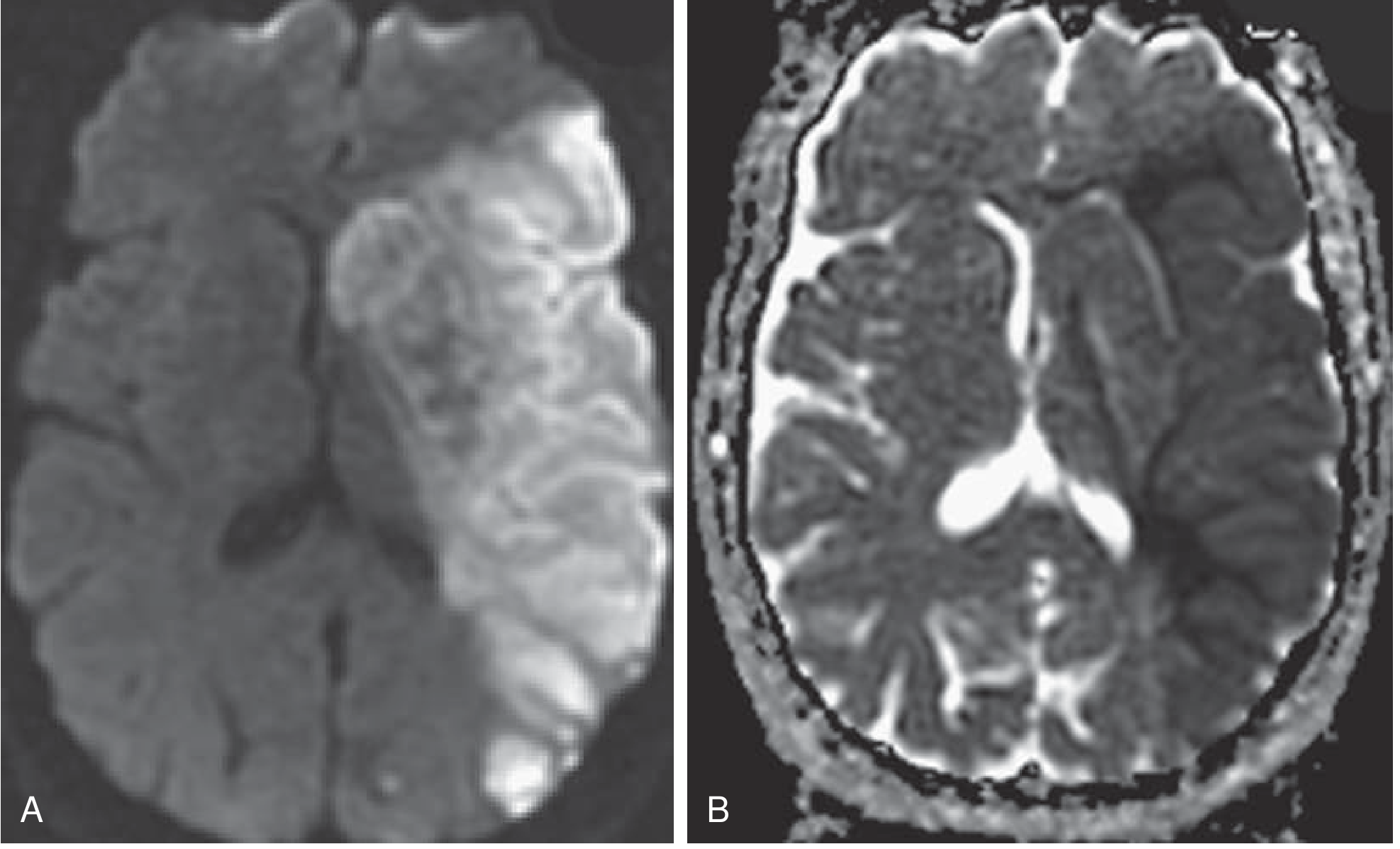
| DWI (Diffusion-Weighted Imaging) | Hyperintense in acute ischemia within minutes of onset - most sensitive | Detects ischemia immediately |
| ADC map (Apparent Diffusion Coefficient) | Hypointense in acute infarct (confirms restricted diffusion); becomes hyperintense after 7-10 days | Age estimation of lesion |
| FLAIR | Normal in hyperacute (<4.5 h); hyperintense after ~6 h; DWI+/FLAIR- = stroke within ~4.5 h | Wake-up stroke eligibility |
| T2 | Normal initially; markedly hyperintense by 4-24 h; stable thereafter | Subacute/chronic changes |
| T1 | Subtle T1 changes; used with Gd for BBB disruption | Less used acutely |
| GRE/SWI (Gradient Echo / Susceptibility) | Detects microbleeds, old hemorrhage, hemorrhagic transformation | Safety check before tPA |
| MRA (MR Angiography) | Non-invasive vessel imaging; identifies occlusion, stenosis | LVO detection without contrast |
| PWI (Perfusion-Weighted Imaging) | Delineates penumbra | DWI-PWI mismatch = viable tissue |
DWI-ADC Correlation: Key to Lesion Age
| ADC Signal | DWI Signal | Age of Lesion |
|---|---|---|
| Hypointense | Hyperintense | Acute (<7-10 days) |
| Isointense | Hyperintense (T2 shine-through) | ~7-10 days |
| Hyperintense | Variable | >10 days (chronic/old) |
DWI-FLAIR Mismatch (Wake-Up Stroke Rule)
- DWI positive + FLAIR negative = stroke onset likely within 4.5 hours - may be eligible for tPA even with unknown onset time
- DWI positive + FLAIR positive = stroke onset likely >4.5-6 hours ago - proceed to perfusion imaging
CT vs MRI - Practical Choice
| Feature | NCCT | MRI-DWI |
|---|---|---|
| Speed | Faster (minutes) | Slower (20-30 min) |
| Hemorrhage detection | High sensitivity | GRE/SWI also reliable |
| Acute ischemia (<6h) | Low (~50%) | Very high (~95%) |
| Posterior fossa | Poor (artifact) | Excellent |
| Availability | Universal | Not always immediately available |
| Penumbra assessment | CTP needed | DWI-PWI mismatch |
| Standard practice | First-line for all | When CT inconclusive, posterior fossa, unknown onset |
Step 3 - Vascular Imaging
| Modality | Purpose |
|---|---|
| CTA head + neck | LVO detection, dissection, tandem lesions - first-line, run with CT |
| MRA head + neck | Alternative to CTA (no contrast); slightly less sensitive for small vessels |
| Carotid duplex ultrasound | Assess extracranial carotid stenosis, plaque morphology; used after acute phase for secondary prevention planning; sensitivity ~92% for dissection |
| Transcranial Doppler (TCD) | Detects MCA stenosis, emboli monitoring; can confirm LVO; also used to detect PFO (bubble study) |
| Conventional DSA (digital subtraction angiography) | Gold standard for vessel anatomy; reserved for pre-thrombectomy/stenting or when non-invasive imaging is inconclusive |
Step 4 - Cardiac Investigations
| Investigation | Purpose |
|---|---|
| 12-lead ECG | Detect atrial fibrillation, acute MI, long QT, ST changes (common in stroke); ECG abnormalities predict 3-month mortality |
| Cardiac monitoring (continuous telemetry 24-48h) | Detect paroxysmal AF - present in up to 25% of cryptogenic strokes if monitored long enough |
| Prolonged cardiac monitoring (30-day event recorder / implantable loop recorder) | Detect intermittent AF in cryptogenic stroke - yields new AF in 12-30% if monitored >30 days |
| Transthoracic echocardiogram (TTE) | Assess wall motion, LV thrombus, valvular disease, cardiomyopathy, PFO |
| Transesophageal echocardiogram (TEE) | Superior sensitivity for: left atrial appendage thrombus, PFO + atrial septal aneurysm, aortic arch atheroma, valvular vegetations |
| Troponin | Elevated in ~20% of stroke; predicts short-term mortality; also rules out concomitant ACS |
Step 5 - Laboratory Investigations
Immediate (all patients - results required before tPA)
| Test | Purpose |
|---|---|
| Blood glucose (bedside) | Most urgent - hypo/hyperglycemia mimics stroke |
| CBC | Thrombocytopenia (tPA contraindication if <100,000), polycythemia, sickle cell |
| Prothrombin time / INR | tPA contraindication if INR >1.7 |
| aPTT | tPA contraindication if elevated (heparin use) |
| Serum electrolytes, renal function (BMP) | Metabolic stroke mimics; baseline for management |
| Blood type and screen | Pre-procedure preparation |
Urgent (within hours)
| Test | Purpose |
|---|---|
| Troponin I/T | Cardiac injury, ACS co-morbidity |
| Lipid panel (fasting) | Risk stratification, statin indication |
| HbA1c | Assess chronic glycemic control, diabetes diagnosis |
| Urine pregnancy test | In women of reproductive age (affects management) |
| Urine drug screen | Cocaine, amphetamines as stroke cause in young |
| Liver function tests | Coagulopathy, hepatic disease |
| Blood cultures | If infective endocarditis suspected (fever, murmur, IV drug use) |
Specialized / Etiologic (selected patients)
| Test | Indication |
|---|---|
| Hypercoagulable panel | Young stroke, cryptogenic, venous sinus thrombosis: protein C, protein S, antithrombin III, factor V Leiden, prothrombin gene mutation, homocysteine |
| Antiphospholipid antibodies | Lupus anticoagulant, anticardiolipin IgG/IgM, anti-β2 glycoprotein I |
| Hemoglobin electrophoresis | Sickle cell disease (especially young patients) |
| ESR, CRP, ANCA, ANA | Vasculitis (especially young; systemic features) |
| Blood smear | TTP (thrombocytopenia + neurologic symptoms) |
| HIV, VDRL/RPR | Infectious vasculopathy (young, HIV risk factors, syphilitic arteritis) |
| Genetic testing | CADASIL (NOTCH3 gene), MELAS (mitochondrial), Fabry disease (GLA gene) - young recurrent strokes |
| CSF analysis | If SAH suspected but CT negative (xanthochromia), CNS vasculitis, CNS infection |
Step 6 - Additional Investigations
| Investigation | Purpose |
|---|---|
| Chest X-ray | Baseline, aspiration pneumonia, cardiomegaly |
| EEG | If seizure activity or altered consciousness - exclude non-convulsive status epilepticus |
| Lumbar puncture | SAH when CT is negative but clinical suspicion is high (xanthochromia on spectrophotometry); CNS infection |
| Sleep study | OSA is a modifiable stroke risk factor - important for secondary prevention |
Summary: Diagnostic Algorithm
Acute neurological deficit
↓
Bedside glucose + NIHSS + ECG monitoring
↓
NCCT head (within 25 min of arrival)
/ \
Hemorrhage No hemorrhage
↓ ↓
ICH/SAH CTA head+neck (concurrent)
confirmed ↓
↓ LVO identified?
Hemorrhagic / \
management Yes No
Thrombectomy tPA if eligible
workup (window + criteria)
↓
MRI if unknown onset,
posterior fossa, or
6-24h window candidate
(DWI-FLAIR / DWI-PWI mismatch)
↓
Etiologic workup:
Echo + cardiac monitoring
+ vascular imaging +
laboratory panel
Make a flowchart
A detailed clinical flowchart titled "Acute Stroke Management" on a clean white background. The flowchart uses color-coded boxes and arrows flowing top to bottom. Structure: 1. TOP BOX (red, wide): "ACUTE STROKE SUSPECTED" with subtitle "Sudden focal neurological deficit" 2. Arrow down to YELLOW BOX: "IMMEDIATE ACTIONS (All patients)" with bullet points: Airway/Breathing/Circulation | IV access | Bedside glucose | Pulse oximetry | ECG monitoring | NIHSS score | Record last-known-well time 3. Arrow down to BLUE BOX: "EMERGENCY BRAIN IMAGING" with text: "Non-Contrast CT Head within 25 min | CT Angiography (concurrent)" 4. From BLUE BOX, TWO BRANCHES with arrows: LEFT BRANCH → GREEN BOX "HEMORRHAGE ON CT" → sub-box "Intracerebral Hemorrhage (ICH)" with: Reverse anticoagulation | BP target SBP 140 mmHg | Treat ICP if elevated | Neurosurgery consult | AND sub-box "Subarachnoid Hemorrhage (SAH)": Neurosurgery emergent | Nimodipine 60mg q4h | Monitor for vasospasm/hydrocephalus RIGHT BRANCH → ORANGE BOX "NO HEMORRHAGE = ISCHEMIC STROKE" with two sub-paths: PATH A (purple box) "tPA ELIGIBLE?" criteria listed: Onset <3h (or <4.5h selected patients) | BP <185/110 | No contraindications | NIHSS disabling → YES → "IV ALTEPLASE 0.9 mg/kg (max 90mg) | 10% bolus then 60 min infusion | BP <180/105 for 24h" PATH B (dark blue box) "LARGE VESSEL OCCLUSION (LVO)?" → YES → "MECHANICAL THROMBECTOMY | 0-6h standard window | 6-24h with DWI/CTP mismatch (DAWN/DEFUSE-3)" 5. BOTTOM SHARED BOX (teal): "ALL ISCHEMIC STROKE - GENERAL CARE" with: Aspirin 325mg (after 24h if tPA given) | BP permissive unless >220/120 (no tPA) | Glucose 140-180 mg/dL | Temp <38°C | Swallow assessment before oral intake | Admit to stroke unit | Etiologic workup: Echo + Holter + lipids + coagulation Color scheme: professional medical blue, red, orange, green, teal. Clean sans-serif font. Arrows clearly labeled. Very readable, clinical style.
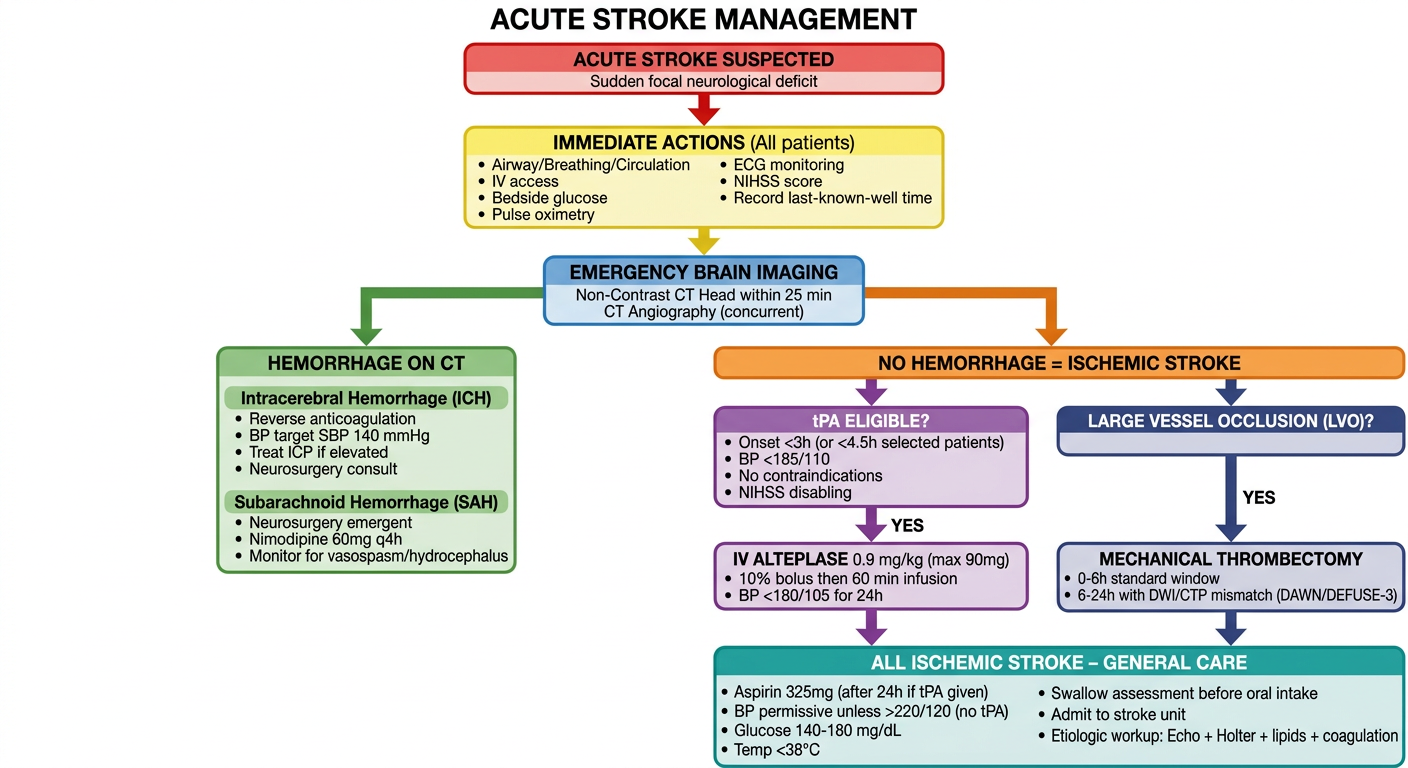
- Immediate actions on suspected stroke (all patients)
- Emergency CT to differentiate hemorrhagic from ischemic
- Hemorrhagic branch - ICH and SAH specific management
- Ischemic branch - tPA eligibility criteria and dosing, plus LVO/thrombectomy pathway
- General ischemic stroke care applicable to all patients at the bottom
Investigation flowchart
A detailed clinical flowchart titled "Stroke Investigation Algorithm" on a clean white background. Professional medical style, color-coded boxes, clear arrows flowing top to bottom with branching paths. Clean sans-serif font, very readable. STRUCTURE: TOP BOX (bold red, wide): "SUSPECTED STROKE / TIA" subtitle: "Sudden focal neurological deficit — Time is Brain" Arrow down to YELLOW BOX: "STEP 1: IMMEDIATE BEDSIDE (Before Imaging)" — two columns of bullet points: Left: Bedside blood glucose (rule out hypoglycemia) | IV access | Pulse oximetry | Continuous ECG monitoring | Blood pressure measurement Right: NIHSS assessment | Record exact last-known-well time | 12-lead ECG | Airway assessment Arrow down to BLUE BOX (wide): "STEP 2: EMERGENCY BRAIN IMAGING" with subtext "Target: CT within 25 min | Read within 45 min of arrival" From BLUE BOX — TWO SIDE-BY-SIDE BOXES connected with "OR": LEFT GREEN BOX "NON-CONTRAST CT HEAD (First-line)" with bullet points: • Rules out hemorrhage (sensitivity >95% for ICH >1cm) • Early ischemic signs: hyperdense artery, sulcal effacement, gray-white loss, insular ribbon loss • Limitations: poor posterior fossa, misses early ischemia RIGHT PURPLE BOX "MRI BRAIN (Higher sensitivity)" with bullet points: • DWI: hyperintense in ischemia within MINUTES • ADC map: hypointense = acute (<7-10 days) • FLAIR: normal <4.5h (DWI+/FLAIR- = onset <4.5h) • GRE/SWI: detects microbleeds • Indications: posterior fossa, unknown onset, inconclusive CT Arrow down to ORANGE BOX "STEP 3: VASCULAR IMAGING" with four sub-boxes in a row: Box 1 (blue): "CTA Head + Neck" — Run concurrent with CT | LVO detection | Dissection | Stenosis Box 2 (blue): "MRA Head + Neck" — Alternative to CTA | No contrast needed Box 3 (blue): "Carotid Duplex US" — Extracranial stenosis | Plaque | Post-acute Box 4 (blue): "CT Perfusion (CTP)" — 6-24h window | Core vs penumbra mismatch | DAWN/DEFUSE-3 Arrow down to TEAL BOX "STEP 4: CARDIAC INVESTIGATIONS" — two columns: Left: 12-lead ECG (AF, acute MI, QT changes) | Continuous telemetry 24-48h | Prolonged monitoring 30 days (cryptogenic) Right: Transthoracic Echo (TTE) — LV thrombus, PFO, valvular disease | Transesophageal Echo (TEE) — LAA thrombus, aortic atheroma | Troponin Arrow down to DARK NAVY BOX "STEP 5: LABORATORY INVESTIGATIONS" — Three labeled columns: Column 1 header "IMMEDIATE (before tPA)": Blood glucose | CBC | PT/INR | aPTT | BMP (electrolytes, renal) | Blood type & screen Column 2 header "URGENT (hours)": Troponin | Lipid panel | HbA1c | LFTs | Urine pregnancy test | Urine drug screen Column 3 header "SPECIALIZED (selected patients)": Hypercoagulable panel (Protein C/S, Factor V Leiden, antithrombin III) | Antiphospholipid antibodies | Hemoglobin electrophoresis | ESR/CRP/ANCA/ANA (vasculitis) | HIV/VDRL | Genetic panel (CADASIL, MELAS, Fabry) BOTTOM BOX (light green border): "STEP 6: ADDITIONAL STUDIES (as indicated)" in one row: Lumbar puncture — CT-negative SAH, CNS vasculitis | EEG — seizure/altered consciousness | Chest X-ray — aspiration, cardiomegaly | Sleep study — OSA screening Color scheme: professional, medical. Red, yellow, blue, purple, orange, teal, navy. All boxes clearly labeled. Arrows between each step clearly shown.
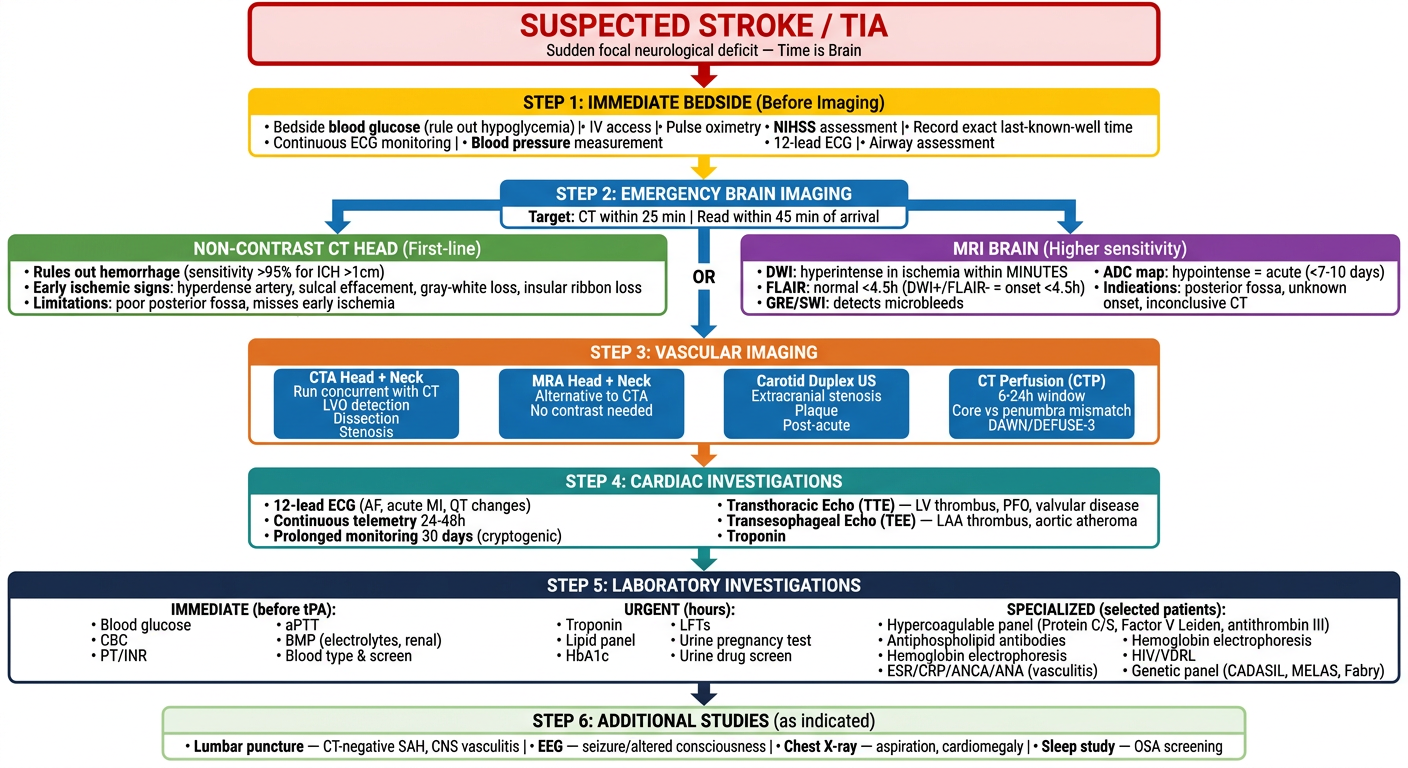
| Step | Focus |
|---|---|
| 1 | Immediate bedside assessment (glucose, NIHSS, ECG, last-known-well time) |
| 2 | Emergency brain imaging - NCCT vs MRI with key findings for each |
| 3 | Vascular imaging - CTA, MRA, carotid duplex, CT perfusion |
| 4 | Cardiac investigations - ECG, telemetry, echo, troponin |
| 5 | Labs in three tiers - immediate (pre-tPA), urgent, and specialized |
| 6 | Additional studies - LP, EEG, CXR, sleep study |