Neglected elbow disslocation external fixators used
Reading File
Finding Sources
Finding Sources
Searching PubMed
"neglected elbow dislocation" AND "external fixator"
Reading File
Finding Sources
Searching PubMed
"neglected elbow dislocation" AND "open reduction"
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive textbook content and images. Let me compile the complete answer.
Neglected Elbow Dislocation - External Fixators
Definition of "Neglected" / Chronic Dislocation
A neglected (old, chronic, or late-presenting) elbow dislocation is one that has gone unreduced for more than 3 weeks. By that point, soft-tissue contracture, localized osteopenia, fibrosis filling the olecranon and coronoid fossae, and possible heterotopic ossification (the "radial humeral horn") make closed reduction virtually impossible and hazardous - the bone may fracture or articular surfaces be damaged.
- Closed reduction: almost impossible after 3 weeks
- Open reduction: results are acceptable if done within 3 months, but a normal elbow should not be expected
- In children, open reduction is worth attempting regardless of duration, as they regain useful ROM
Why External Fixators Are Used
After open reduction of a chronic elbow dislocation, the elbow is frequently unstable because:
- The collateral ligaments have shortened and require release/reconstruction
- Wide soft-tissue resection is needed to achieve reduction
- Ligamentous repair alone carries a ~30% recurrent dislocation rate
The external fixator addresses this by:
- Protecting the repair and maintaining joint reduction
- Permitting early motion - avoiding the stiffness that results from postoperative immobilization
- Enhancing muscle-tendon stretching during the healing phase
Types of External Stabilization Devices
1. Hinged Elbow External Fixator (Historical Standard)
The classic device used for neglected elbow dislocation. Examples include the Compass Elbow Hinge (Smith & Nephew).
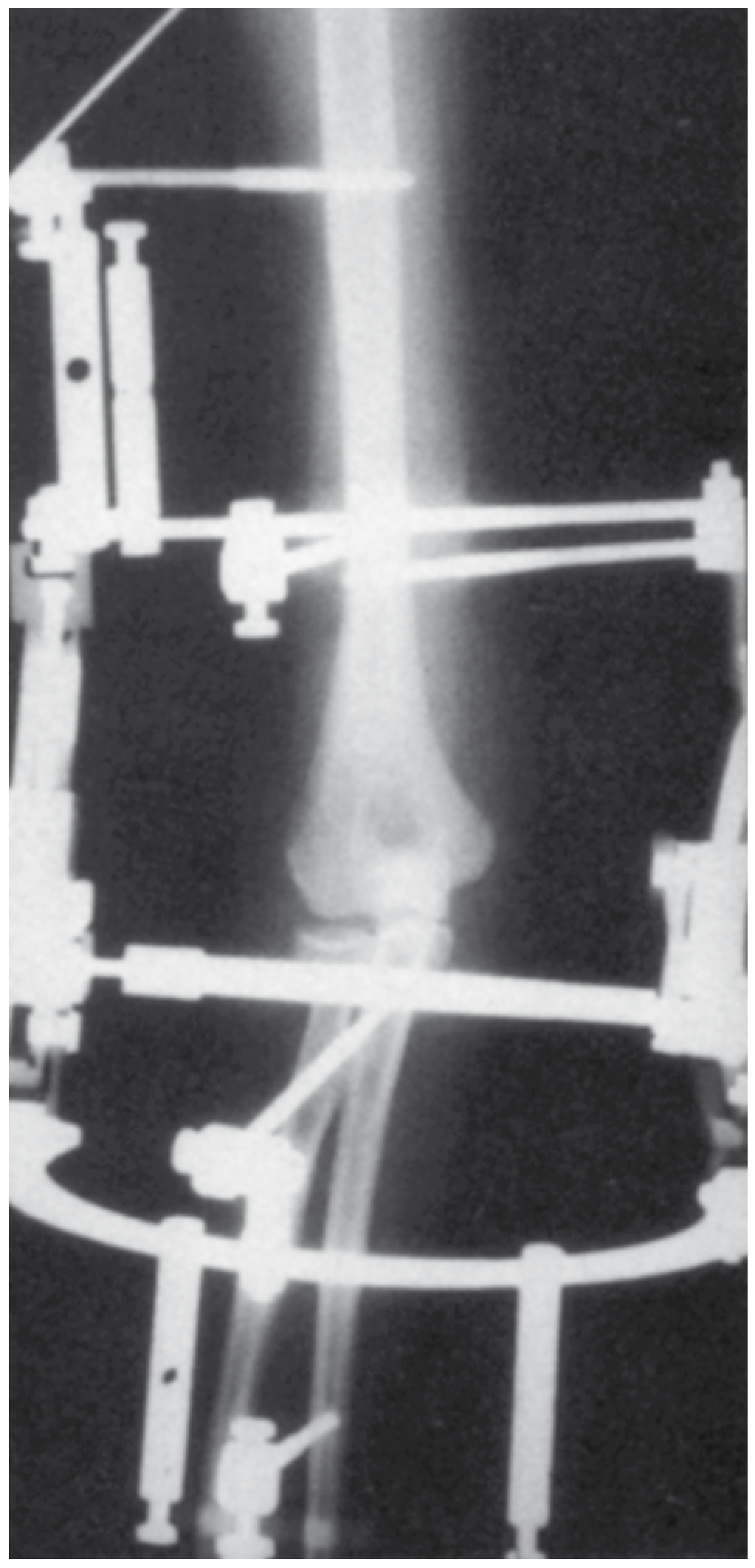
Radiograph showing hinged external fixation following open reduction of a late-discovered (6 weeks) medial elbow dislocation without ligament repair/reconstruction.
Pin Placement (Hotchkiss Technique - Compass Elbow Hinge):
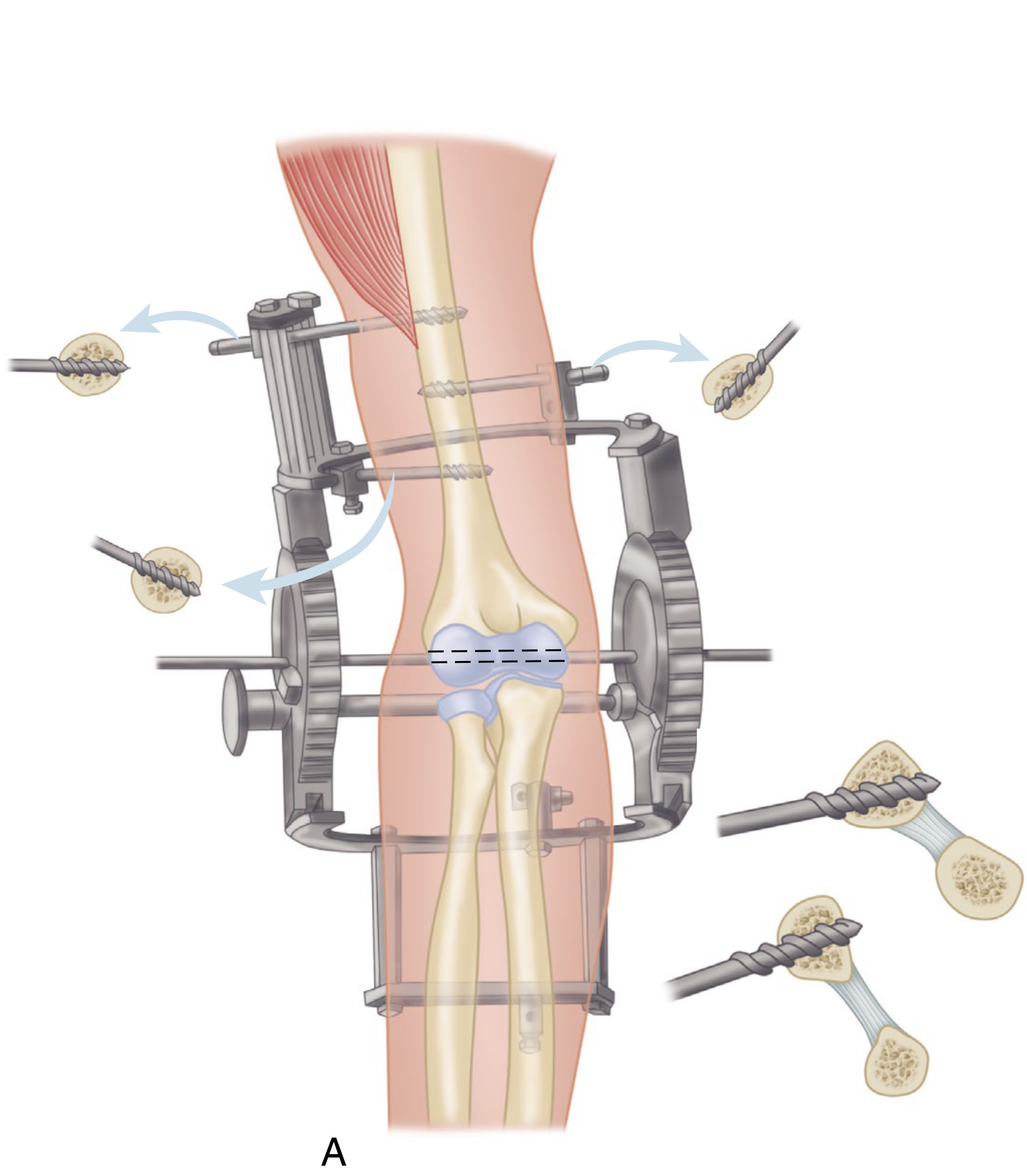
Representative pin placements for hinged external fixator in old elbow dislocation. Placements may be modified based on patient needs.
- The hinge pin must be placed along the central rotational axis of the elbow (through the center of the capitellum, coaxial with the trochlea)
- Humeral half-pins are placed anteriorly and posteriorly to the axis
- Ulnar half-pins or a ring/frame are fixed distally
- The hinge is left in place for ~8 weeks, during which active and passive ROM exercises are performed
Complications of hinged external fixator:
- Radial nerve injury (can be frequent)
- Pin-track infection
- Difficulty with accurate axis placement
- Bulky construct limiting patient compliance
2. Internal Joint Stabilizer (IJS) - Modern Preferred Device
The Internal Joint Stabilization (IJS) device (Skeletal Dynamics, Miami) has largely supplanted hinged external fixation in many centers.
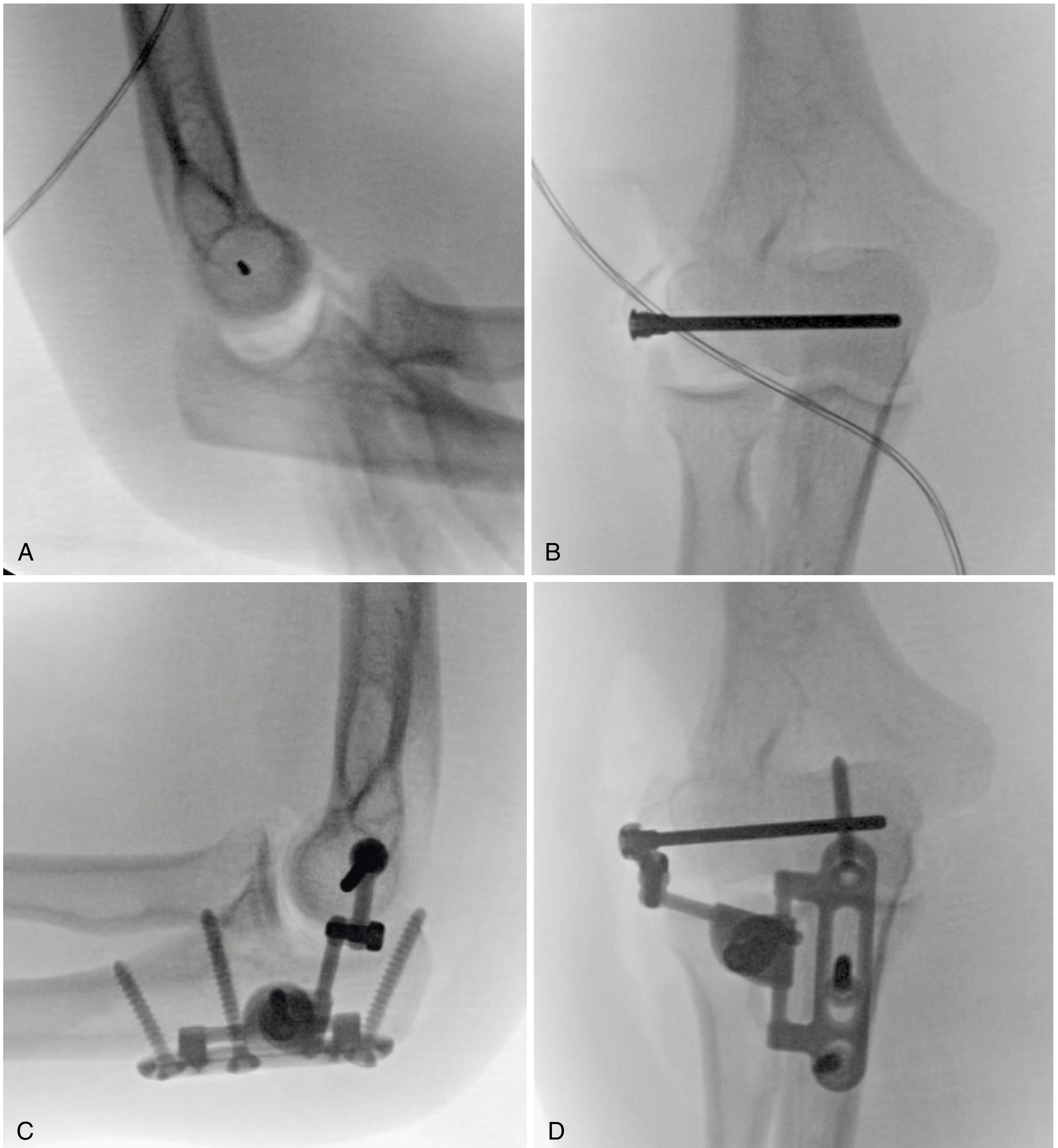
A: Lateral fluoroscopic image of guidepin placed along central rotational axis. B: AP view after placement of central axis pin. C & D: Final lateral and AP fluoroscopy demonstrating IJS device with concentric ulnohumeral and radiocapitellar joints.
How it works:
- A post is established along the elbow's central rotational axis using a guidepin under fluoroscopy
- The hinge is locked into the device, which is fixed to the ulna
- The joint is reduced concentrically, and the IJS is locked in position
- Allows concentric flexion-extension along the defined axis of rotation while maintaining a stable platform
Advantages over hinged external fixator:
- Functions as an internal fixator - better tolerated, less bulky
- Maintains stable concentric reduction through the full arc of motion
- Allows immediate range of motion post-operatively despite the instability from wide soft-tissue resection
- Dual function: maintains congruent elbow ROM and protects from early ligament reconstruction failure
- Elective implant removal between 4 and 6 months
Campbell's Expert Opinion (2026): "The IJS has largely supplanted the need to perform hinged elbow external fixation. Early range of motion after elbow capsular release is paramount. A correctly applied IJS provides sufficient stability to initiate immediate range of motion."
Surgical Steps for Open Reduction (Speed Technique) - Neglected Posterior Dislocation
- Posterolateral approach - incision from 10 cm proximal to olecranon, continuing distally and laterally
- Identify and protect/transpose the ulnar nerve
- Reflect triceps aponeurosis as a distally attached flap
- Subperiosteally free all muscle attachments from distal humerus (anteriorly and posteriorly)
- Release joint capsule and collateral ligament attachments around condyles
- Remove all callus and scar tissue from posterior humerus and olecranon fossa
- Clear radial head and trochlear notch of ulna
- Gently press the capitellum anteriorly - bring radial head into normal position
- After reduction - apply hinged fixator or IJS to protect the reconstruction
- Active and passive ROM begun immediately or within the first week
Summary Table
| Feature | Hinged External Fixator | Internal Joint Stabilizer (IJS) |
|---|---|---|
| Type | External frame | Internal implant on ulna |
| Axis establishment | Fluoroscopic / clinical | Fluoroscopic guidepin |
| Duration in situ | ~8 weeks | 4-6 months then elective removal |
| Early ROM | Yes (goal) | Yes (immediate) |
| Complications | Radial nerve injury, pin-track infection | Lower profile, better tolerated |
| Current status | Historical standard | Now preferred |
Key References
- Campbell's Operative Orthopaedics 15th Ed 2026, Chapter 66 (Chronic/Neglected Elbow Dislocations)
- Rockwood and Green's Fractures in Adults 10th Ed 2025, Chapter 15-16
- Hotchkiss RN: Compass Elbow Hinge Surgical Technique. Smith & Nephew, 2004
- Orbay JL et al. - Internal Joint Stabilizer (Skeletal Dynamics)
Recent literature (PubMed): Case series on neglected elbow dislocations confirm open reduction remains viable even in late presentations. A 2023 case report (PMID 37752900) using a double-approach technique and a 2025 case report (PMID 41281861) using the "box-loop technique" for ligamentous reconstruction both demonstrate acceptable functional outcomes. High-level evidence (RCTs) specifically comparing fixator types for neglected elbow dislocation is lacking - most evidence comes from case series and expert opinion.
Complete details about neglected elbow joint dislocation as i am doing poster on it in my case open reduction with bell tawse and tommy John procedure was done what are the possible questions that they can ask
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Here is the complete, structured guide for your poster presentation on neglected elbow dislocation treated with open reduction + Bell-Tawse + Tommy John procedures.
NEGLECTED ELBOW DISLOCATION - Complete Poster Guide
SECTION 1: DEFINITION & EPIDEMIOLOGY
Neglected (chronic/old) elbow dislocation = a dislocation that remains unreduced for >3 weeks (some authors use >2 weeks; the consensus cutoff is 3 weeks for closed reduction being hazardous).
- More common in developing countries due to delayed presentation, traditional bone-setting practices, lack of access to orthopaedic care
- Posterolateral dislocations are the most common type overall
- Adult elbows unreduced for >3-6 months may require arthroplasty rather than open reduction
- In children, open reduction is worth attempting regardless of duration - they regain useful flexion-extension more reliably than adults
SECTION 2: ANATOMY OF ELBOW STABILITY
Understanding this is mandatory for your poster - examiners will ask about it.
Bony Stability (Primary)
- Ulnohumeral articulation - trochlea in trochlear notch = primary bony constraint
- Coronoid process - resists posterior translation
- Radial head - resists axial and valgus loads (proximal radioulnar + radiocapitellar)
Ligamentous Stability (Secondary)
Medial (UCL) Complex:
- Anterior bundle of MCL = primary medial stabilizer; runs from medial epicondyle to sublime tubercle of ulna; resists valgus stress
- Posterior bundle - tightens in flexion
- Transverse bundle - minimal contribution
Lateral (LCL) Complex:
- Lateral ulnar collateral ligament (LUCL) = most important; runs from lateral epicondyle to crista supinatoris of ulna; resists posterolateral rotatory instability (PLRI)
- Radial collateral ligament
- Annular ligament - stabilizes radial head in proximal radioulnar joint
Muscular/Dynamic Stability
- Brachialis, biceps (anterior)
- Common flexor and extensor mass (medial and lateral compressive forces)
- Anconeus
SECTION 3: MECHANISM OF DISLOCATION
Most common mechanism: Fall on outstretched hand (FOOSH) with the elbow slightly flexed
- Axial load + valgus + forearm supination
- Force transmitted: wrist → radius → capitellum → lateral compartment fails first
"Horii Circle" / O'Driscoll's Sequential Disruption Pattern:
- Stage 1: LUCL tears (posterolateral instability)
- Stage 2: Anterior and posterior capsule tears
- Stage 3a: Partial MCL tear (posterior bundle)
- Stage 3b: Complete MCL tear → full dislocation
This means the lateral side always fails first, the medial side last.
SECTION 4: CLASSIFICATION
By Direction
| Type | Frequency | Notes |
|---|---|---|
| Posterior / posterolateral | ~80-90% | Most common; arm in extension/slight flexion |
| Posteromedial | Less common | |
| Lateral | Rare | |
| Medial | Rare | |
| Anterior | Very rare | Associated with direct posterior blow |
| Divergent | Very rare | Radioulnar dissociation |
By Associated Injuries (Simple vs Complex)
- Simple = no associated fractures
- Complex = with fractures (radial head, coronoid, olecranon)
- "Terrible Triad" = elbow dislocation + radial head fracture + coronoid fracture
By Duration (Acute vs Neglected)
- Acute: <3 weeks
- Chronic/Neglected: >3 weeks (some: >2 weeks)
SECTION 5: PATHOLOGICAL FINDINGS IN NEGLECTED DISLOCATION
This is distinctive and examiners love asking about it:
- Heterotopic ossification around the joint (extensive)
- Marked shortening of triceps muscle
- Shortening and contracture of collateral ligaments (medial and lateral)
- Ulnar nerve tightening with attempts at flexion
- Fibrous/ossified joint capsule, may cause ankylosis
- Dense fibrous tissue filling olecranon and coronoid fossae
- "Radial-humeral horn" - pathognomonic of neglected dislocation:
- Ossification of a hematoma near the periosteum adjacent to the radial head/capsule
- Creates a bony block to reduction
Clinical appearance: Arm fixed in extension or very slight flexion, minimal ROM. Pronation more limited than supination (biceps under tension from angulation around condyles, pulling forearm into supination).
SECTION 6: INVESTIGATIONS
Plain X-rays (AP + Lateral):
- Confirm direction and type of dislocation
- Identify any associated fractures
- Identify heterotopic ossification / radial humeral horn
- Assess joint surface congruity
CT scan:
- Best for coronoid fractures, radial head fractures
- Map heterotopic ossification and bony blocks
- 3D reconstruction helps pre-operative planning
MRI:
- Ligamentous injuries
- Articular cartilage assessment (needed if arthroplasty being considered)
SECTION 7: TREATMENT OPTIONS
Conservative (usually fails in neglected cases)
- Closed reduction under GA: virtually impossible after 3 weeks; risk of fracture or articular damage
Surgical Options (in order of increasing severity)
| Option | Indication |
|---|---|
| Open reduction | < 3 months, good joint surfaces |
| Open reduction + ligament reconstruction | Post-reduction instability (your case) |
| Distraction interposition arthroplasty | Chronic, joint degeneration, young patient |
| Total elbow arthroplasty | Elderly, > 3-6 months, significant degeneration |
| Arthrodesis | Salvage, failed arthroplasty |
SECTION 8: OPEN REDUCTION - SURGICAL PRINCIPLES (Speed Technique)
- Posterolateral approach - incision from 10 cm proximal to olecranon, laterally to radial head, 5 cm distally
- Ulnar nerve identification and protection (low threshold for transposition due to tension with flexion)
- Reflect triceps aponeurosis distally as an attached flap
- Subperiosteal release of all muscle attachments from distal humerus (anterior + posterior)
- Release joint capsule and collateral ligaments from condyles to mobilize distal humerus
- Remove all callus, scar tissue from posterior humerus and olecranon fossa
- Remove radial-humeral horn if present (essential - it blocks reduction)
- Clear trochlear notch of ulna
- Rotate forearm, press capitellum anteriorly to bring radial head into position
- Achieve concentric reduction and assess stability
- Ligament reconstruction if instability persists (your case)
- Ulnar nerve decompression/transposition as indicated
- Apply hinged fixator / IJS as needed
Important: "Triceps must be lengthened if shortened."
SECTION 9: BELL-TAWSE PROCEDURE
What It Is
The Bell-Tawse procedure is a lateral/annular ligament reconstruction using a strip of triceps tendon fashioned as a loop around the radial neck, reconstructing the annular ligament.
Historical Context
- Originally described by Bell Tawse AJ (1965) for treatment of malunited anterior Monteggia fractures in children (J Bone Joint Surg Br. 1965;47:718)
- Adopted subsequently for radial head dislocations and chronic Monteggia variants
Indication in Your Case
- After open reduction, radial head instability persists (radiocapitellar joint unstable)
- Annular ligament is absent/incompetent/destroyed
- The native annular ligament cannot be repaired
Technique (Bell-Tawse)
- Expose the radial head via lateral approach (Kocher or Kaplan)
- Harvest a strip of triceps tendon (approximately 1 cm wide, 8-10 cm long), keeping it attached distally or as a free graft
- Pass the strip around the radial neck in a loop
- Secure the loop to itself (or to bone) to reconstruct the annular ligament
- Confirm radial head reduction and stability through full ROM
- Pinning of radiocapitellar joint: avoid if possible (risk of pin breakage intra-articularly) - if unstable enough to need pinning, check for adequate ulnar reduction or entrapped soft tissue
Key Point
Radial head resection should be avoided in younger patients - risk of late deformity (proximal migration of radius, cubitus valgus, ulnar neuropathy)
SECTION 10: TOMMY JOHN PROCEDURE (UCL Reconstruction)
What It Is
Reconstruction of the medial/ulnar collateral ligament (UCL) - specifically the anterior bundle - using a tendon graft. Named after baseball pitcher Tommy John, who had the first procedure performed by Dr. Frank Jobe in 1974.
Why It Is Needed in Your Case
- After open reduction of neglected elbow, the MCL/UCL is contracted and released during the approach - it cannot simply be reattached as viable tissue
- Without medial stability, elbow will re-dislocate in valgus
- ~30% recurrent dislocation rate after ligamentous repair alone justifies formal reconstruction
Anatomy Targeted
- Anterior bundle of MCL: Origin = medial epicondyle (anterior-inferior aspect) → Insertion = sublime tubercle on anteromedial coronoid/ulna
- This is the primary restraint to valgus stress between 20-120° flexion
Graft Choices
| Graft | Notes |
|---|---|
| Palmaris longus (most common) | Absent in 15% of population; check preop |
| Gracilis | Higher rate of heterotopic ossification (10%) at harvest site |
| Plantaris | Thin; less favored |
| Hamstrings | Used in revision cases |
Techniques
Jobe Original Technique (1986):
- Flexor mass detached from epicondyle
- Open-ended tunnels in ulna (sublime tubercle) and medial epicondyle
- Palmaris longus graft in figure-of-8
- Ulnar nerve anteriorly transposed
Modified Jobe (most common now):
- Flexor-pronator mass split (not detached) through FCU interval
- Closed-ended tunnel in medial epicondyle ("docking" variant)
- Ulnar nerve transferred only if there is heavy scar around it or chronic nerve changes
Docking Technique (Altchek):
- Single tunnel in ulna
- Two small cortical exits on medial epicondyle
- Graft docked in humeral tunnel and tied over bony bridge
- Less hardware, good biomechanics
Key Surgical Steps (Modified Jobe)
- Medial incision over medial epicondyle
- Identify and protect medial antebrachial cutaneous nerve
- Identify and protect/transpose ulnar nerve
- Split flexor carpi ulnaris to expose UCL
- Drill tunnel in sublime tubercle of ulna (3.5-4 mm)
- Drill closed-ended tunnel in medial epicondyle
- Pass graft, tension, secure in figure-of-8 or docking configuration
- Test stability with valgus stress
Outcomes
- 83% of athletes with primary reconstruction return to same level of play
- Revision reconstruction: 42-63% return to play
- Mean return to sport: ~13 months after primary reconstruction
- Ulnar nerve neuropraxia if transposed: ~12%
SECTION 11: POST-OPERATIVE MANAGEMENT
- Splint at 90° for first 2 weeks (wound healing)
- Active and passive ROM exercises started early (within days if fixator used)
- If hinged fixator/IJS applied: ROM exercises while fixator in place
- Extension blocking: block extension at 45° for week 1, 30° for week 2
- Full motion thereafter
- Splint at night for 2-3 months
- Expect prolonged recovery - "if dislocation has been present for a long time, best results require continuing exercises for a long time"
- Children regain motion more easily than adults
SECTION 12: COMPLICATIONS
| Complication | Notes |
|---|---|
| Re-dislocation | ~30% after ligament repair alone; reduced with fixator/reconstruction |
| Stiffness/loss of extension | Most common functional deficit |
| Ulnar nerve palsy | From pre-existing traction or iatrogenic during surgery; decompress/transpose |
| Posterior interosseous nerve (PIN) injury | During lateral dissection for Bell-Tawse |
| Radial nerve injury | During external fixator pin placement |
| Heterotopic ossification | Especially with delayed surgery; consider NSAIDs prophylaxis |
| Avascular necrosis | Disruption of blood supply to condyles |
| Infection | Pin-track infection with external fixators |
| Residual instability | May need further reconstruction |
| Arthrosis | Especially after prolonged neglect |
SECTION 13: LIKELY EXAMINER QUESTIONS AND MODEL ANSWERS
Basic Science / Anatomy
Q1. What is the primary stabilizer of the elbow against valgus stress?
A: The anterior bundle of the medial collateral ligament (UCL) - it runs from the medial epicondyle to the sublime tubercle of the ulna and is the primary restraint from 20° to 120° of flexion.
Q2. Which structure fails first in a posterolateral elbow dislocation?
A: The lateral ulnar collateral ligament (LUCL) fails first, followed sequentially by the anterior and posterior capsule, then the MCL (O'Driscoll's circle of instability).
Q3. What is posterolateral rotatory instability (PLRI)?
A: Instability pattern where the forearm supinates and rotates posterolaterally relative to the humerus due to LUCL insufficiency. Tested by the lateral pivot-shift test (O'Driscoll).
Q4. What is the "radial humeral horn" and why is it important?
A: It is ossification of the hematoma near the periosteum adhering to the capsule at the radial head, seen in neglected dislocations. It creates a bony block to reduction and must be excised to achieve concentric reduction.
Diagnosis
Q5. What are the clinical features of neglected elbow dislocation?
A: Arm fixed in extension or slight flexion; elbow appears widened; prominent olecranon posteriorly; limited ROM (flexion more limited than extension); pronation more limited than supination (biceps under tension pulling into supination); ulnar nerve symptoms possible; shortened triceps.
Q6. Why is CT preferred over MRI in pre-operative planning for neglected elbow dislocation?
A: CT (especially 3D reconstruction) better defines heterotopic ossification, bony blocks, radial-humeral horn, and articular congruity. MRI is better for soft tissue, but surgical planning in neglected cases is primarily about bony pathology.
Surgical Decision Making
Q7. Why can't you just close-reduce a neglected elbow dislocation?
A: After 3 weeks, soft-tissue contracture and localized osteopenia make closed reduction hazardous - the bone may fracture and articular surfaces may be damaged. Extensive fibrosis, shortened ligaments, and the radial humeral horn physically obstruct reduction.
Q8. What are your treatment options for neglected posterior elbow dislocation?
A: (1) Closed reduction (only if <3 weeks), (2) Open reduction ± ligament reconstruction, (3) Distraction interposition arthroplasty (chronic + joint degeneration + young), (4) Total elbow arthroplasty (elderly, >3-6 months), (5) Arthrodesis (salvage).
Q9. Why did you choose open reduction over arthroplasty in this case?
A: Duration was within 3 months / patient is young / joint surfaces were preserved. Open reduction is preferred when joint surface is viable, as it preserves bone stock, maintains normal biomechanics, and avoids implant-related complications.
Q10. What is the 30% recurrent dislocation rate you mentioned - what does this mean?
A: After ligamentous repair alone in neglected elbow dislocation, approximately 30% of patients develop recurrent dislocation. This is why formal ligament reconstruction (rather than repair) and/or use of a hinged external fixator/IJS is recommended.
Bell-Tawse Specific
Q11. Why did you perform the Bell-Tawse procedure?
A: After open reduction, the radial head was unstable at the radiocapitellar joint due to annular ligament destruction/absence. The Bell-Tawse procedure reconstructs the annular ligament using a triceps tendon strip to maintain radial head reduction.
Q12. Why not just excise the radial head instead of reconstructing it?
A: Radial head excision should be avoided in young/active patients because of risk of: proximal radial migration, cubitus valgus, late ulnar nerve palsy (tardy ulnar nerve palsy), and decreased grip strength. Excision is only a salvage procedure.
Q13. What nerve are you protecting during the lateral approach for Bell-Tawse?
A: The posterior interosseous nerve (PIN) - it passes through the radial tunnel and can be injured during dissection around the radial neck. The nerve is identified between brachialis and brachioradialis proximally.
Q14. Why should you avoid radiocapitellar joint pinning if possible?
A: Risk of intra-articular pin breakage. If the joint is unstable enough to require pinning, the surgeon should re-evaluate for inadequate ulnar reduction or entrapped soft tissue (not just pin it and leave).
Tommy John / UCL Reconstruction Specific
Q15. Why did you do UCL reconstruction (Tommy John) in a neglected dislocation case?
A: In chronic dislocation, the UCL is contracted, attenuated, and of poor quality - it cannot provide meaningful stability after repair alone. Formal reconstruction with a healthy tendon graft provides reliable medial stability and protects the reduction.
Q16. Where exactly do you drill the tunnels in Tommy John surgery?
A: Humeral tunnel: in the anterior-inferior medial epicondyle (isometric point of UCL origin). Ulnar tunnel: at the sublime tubercle on the anteromedial aspect of the coronoid process/proximal ulna, approximately 2 cm from the tip of the olecranon.
Q17. What graft do you use and why?
A: Palmaris longus is most common - low donor-site morbidity, appropriate size, no functional deficit. Must check that it is present (absent in ~15%). If absent, gracilis is the alternative but has higher rate of heterotopic ossification (10%) at harvest site.
Q18. What do you do about the ulnar nerve?
A: The ulnar nerve runs immediately posterior to the medial epicondyle and is at risk. In the modified Jobe technique, the nerve is identified and protected. It is formally transposed anteriorly only if: heavy scar tissue around it, or chronic nerve changes (cubital tunnel syndrome). Routine anterior transposition carries 12% neuropraxia risk.
Q19. What is the docking technique? How does it differ from Jobe?
A: Docking (Altchek): single tunnel in the ulna, two small exit tunnels on the medial epicondyle through which the graft ends are brought out and tied over a bony bridge. Advantages: preserves medial epicondyle bone, no suture anchor needed, secure fixation. Jobe: open-ended humeral tunnel with figure-of-8 graft. Results are comparable between the two.
Complications / Post-Op
Q20. What is your post-operative protocol?
A: Splint at 90° for 2 weeks; then progressive ROM - extension blocked at 45° for week 1, 30° for week 2, full motion after; active and passive exercises continued long-term; night splinting for 2-3 months. If unstable, external fixator/IJS applied intra-operatively with ROM exercises begun immediately.
Q21. What complications can occur after your procedure?
A: (1) Re-dislocation, (2) Stiffness/loss of terminal extension (most common functional deficit), (3) Ulnar nerve palsy (neuropraxia or permanent), (4) PIN injury, (5) Heterotopic ossification, (6) Infection, (7) Graft failure/re-rupture, (8) Avascular necrosis of condyle.
Q22. When would you consider the case a failure and what would you do?
A: If open reduction fails to maintain concentric reduction, or joint surfaces are destroyed: consider distraction interposition arthroplasty (fascia lata, young patient) or total elbow replacement (elderly). Arthrodesis as last resort.
"Tricky" / Viva-Type Questions
Q23. What is the elbow's "circle of instability"? Who described it?
A: Described by O'Driscoll. It refers to the sequential disruption of elbow stabilizers from lateral to medial with progressive force: LUCL → capsule → MCL, creating progressive instability (subluxation → dislocation).
Q24. What is the Terrible Triad? How would your management differ if this was your case?
A: Elbow dislocation + radial head fracture + coronoid fracture. Management: (1) Coronoid ORIF (if Type II/III), (2) Radial head ORIF or replacement (not excision alone), (3) Lateral ligament repair, (4) MCL repair if unstable after lateral repair, (5) Hinged fixator if still unstable. Much more complex than simple neglected dislocation.
Q25. What is the difference between Bell-Tawse and other annular ligament reconstructions?
A: Bell-Tawse uses a triceps tendon strip (local tissue - no separate donor site). Other options include: fascia of the forearm, free graft from palmaris longus, or native annular ligament if salvageable. The triceps strip is conveniently available in the same surgical field during elbow reconstruction.
Q26. Why is this case more common in developing countries?
A: Reasons include: delayed presentation due to lack of access to orthopaedic facilities, reliance on traditional/indigenous bone setters who may attempt manipulation without imaging, poverty, patient unawareness, and referral delays. The initial dislocation may be inadequately treated.
Q27. What would be your approach if the patient presented with ulnar nerve palsy preoperatively?
A: Document the deficit completely (motor + sensory, grade). At surgery, decompress the ulnar nerve first. If the nerve is under significant tension with the elbow reduced (as expected from shortening), perform anterior transposition. Post-op monitor recovery. EMG/NCS at 3 months if no recovery.
SECTION 14: KEY REFERENCES FOR YOUR POSTER
- Campbell's Operative Orthopaedics 15th Ed 2026, Chapter 66
- Rockwood and Green's Fractures in Adults 10th Ed 2025
- Bell Tawse AJ. Treatment of malunited anterior Monteggia fractures in children. J Bone Joint Surg Br. 1965;47:718
- Jobe FW et al. Reconstruction of the ulnar collateral ligament in athletes. J Bone Joint Surg Am. 1986
- Donohue KW, Mehlhoff TL. Chronic elbow dislocation: evaluation and management. J Am Acad Orthop Surg. 2016;24:413
- O'Driscoll SW. Elbow instability. Hand Clin. 1994;10:405
QUICK SUMMARY CHEAT-SHEET
| Point | Key Fact |
|---|---|
| Definition | Unreduced >3 weeks |
| Most common type | Posterolateral |
| Most common mechanism | FOOSH with valgus + supination |
| Pathognomonic feature | Radial humeral horn |
| Closed reduction limit | Virtually impossible after 3 weeks |
| Open reduction result | Acceptable if <3 months; no normal elbow expected |
| Recurrent dislocation risk without reconstruction | ~30% |
| Bell-Tawse | Triceps strip → annular ligament reconstruction |
| Tommy John graft (1st choice) | Palmaris longus |
| Absent in ~15% | Palmaris longus |
| UCL reconstruction first performed | Dr. Frank Jobe, 1974 |
| Return to sport (primary UCL recon) | 83% at ~13 months |
| Most feared nerve at lateral approach | PIN (posterior interosseous nerve) |
| Most feared nerve at medial approach | Ulnar nerve |
| Children vs Adults | Children always attempt OR; regain motion better |
Good luck with your poster presentation!
This is a shared conversation. Sign in to Orris to start your own chat.