Approach to hemoptysis
Reading File
Finding Sources
Searching PubMed
hemoptysis management diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-organized response. Here is a comprehensive approach to hemoptysis based on multiple authoritative textbooks:
Approach to Hemoptysis
Definition and Classification
Hemoptysis is the expectoration of blood or blood-stained sputum from the lower respiratory tract (below the glottis). The volume and acuity guide the urgency of evaluation.
| Category | Definition |
|---|---|
| Non-massive | Blood-streaked sputum to moderate volumes without physiologic compromise |
| Submassive | Significant volumes causing concern but not yet life-threatening |
| Massive / Life-threatening | >600 mL/24 h; OR >100 mL/24 h with abnormal gas exchange, airway obstruction, or hemodynamic instability |
Any volume that threatens the airway is effectively "massive." - Washington Manual of Medical Therapeutics
Step 1 - Confirm True Hemoptysis
Before proceeding, distinguish hemoptysis from:
- Pseudohemoptysis: blood from the upper airway (nose, pharynx, larynx) - inhaled and expectorated
- Hematemesis: vomited blood
| Feature | Hemoptysis | Hematemesis |
|---|---|---|
| Color | Bright red, frothy | Dark, "coffee-ground" |
| pH | Alkaline | Acid |
| Mixed with | Frothy sputum, hemosiderin-laden macrophages | Food particles |
| Prodrome | Cough, chest sensation | Nausea |
| History | Lung/airway disease | GI disease |
- Fishman's Pulmonary Diseases and Disorders, p. 444
Step 2 - Identify the Bleeding Source (Pathophysiology)
The vascular anatomy determines bleeding severity:
Bronchial circulation (high pressure, from aorta/intercostals):
- Only 1% of pulmonary blood flow, but accounts for up to 88% of massive hemoptysis
- Disrupted by: tumor invasion, fungal invasion, foreign body, denuded mucosa (bronchiectasis)
Pulmonary circulation (low pressure, 99% of flow):
-
Sources: vasculitis, DAH, PE/infarction, severe mitral stenosis, AVM rupture, Rasmussen aneurysm (TB cavity eroding a pulmonary artery), pulmonary artery catheter trauma
-
Washington Manual of Medical Therapeutics, p. 380
Step 3 - Differential Diagnosis
Causes are best organized anatomically:
Airway
- Acute/chronic bronchitis (most common cause in developed countries; 2-37% of cases)
- Bronchiectasis (1-37%; especially CF, post-TB)
- Bronchogenic carcinoma (2-24%; must rule out in smokers >40 years)
- Carcinoid tumor, endobronchial metastases (breast, colon, kidney, melanoma)
- Foreign body, broncholithiasis, bronchovascular fistula, pulmonary endometriosis (catamenial hemoptysis)
Parenchymal
- Tuberculosis (2-69%; leading cause globally; cavities → Rasmussen aneurysm)
- Pneumonia, lung abscess
- Fungal infections - aspergilloma (colonization of old TB cavity; massive hemoptysis as cavities erode bronchial/pulmonary vessels)
- Vasculitides - GPA (Wegener's), Goodpasture syndrome (anti-GBM), ANCA-positive vasculitis, SLE → diffuse alveolar hemorrhage
Vascular
- Pulmonary embolism with infarction (classically pleuritic pain + hemoptysis + small pleural effusion)
- Mitral stenosis (submucosal bronchial venous congestion; historically a classic cause of brisk bright-red hemoptysis)
- LV failure (pink, frothy sputum; heart failure cells/hemosiderin-laden macrophages)
- AVM, Dieulafoy disease of the bronchus (rare submucosal broncho-pulmonary arterial fistula)
Coagulopathic / Systemic
- Thrombocytopenia, DIC, anticoagulant therapy, hemophilia
- Cocaine and other inhaled agents
Idiopathic
- Up to 50% of cases remain unexplained; up to 4% of these are eventually diagnosed with malignancy
Age clue: Hemoptysis in patients <40 years → think infection. In patients >40-45 years or with smoking history → bronchogenic carcinoma heads the list.
- Fishman's Pulmonary Diseases and Disorders, p. 443
Step 4 - Initial Evaluation
History
Key elements:
- Volume (estimated), onset, duration, recurrence
- Age, smoking history (>40 pack-year smoking, age >40: risk factors for malignancy)
- Prior lung disease (TB, bronchiectasis, COPD, malignancy)
- Associated symptoms: fever/productive cough (infection), weight loss/hemoptysis >1 week (malignancy), pleuritic chest pain (PE), dyspnea, leg swelling
- Coagulopathy risk, anticoagulant/antiplatelet use
- Geographic exposure (TB, histoplasmosis, paragonimiasis)
- Menstrual timing (catamenial hemoptysis)
Physical Examination
- Vital signs + SpO2 first
- Lung: focal crackles, bronchial breath sounds, wheeze/stridor
- Heart: murmurs (mitral stenosis = opening snap + mid-diastolic rumble)
- Skin/mucous membranes: telangiectasias (HHT), purpura (vasculitis), clubbing (malignancy, bronchiectasis)
- Lymphadenopathy, cachexia (malignancy)
Step 5 - Investigations
Bedside / Emergency (all patients)
| Test | Purpose |
|---|---|
| CBC | Anemia severity, thrombocytopenia |
| CMP | Renal function (pulmonary-renal syndrome) |
| PT/PTT | Coagulopathy |
| Type & crossmatch | Massive hemoptysis preparation |
| ABG | Gas exchange assessment |
| CXR (PA + lateral) | First-line; may be normal in up to 50% of cases; normal in up to 10% of lung cancers |
Targeted Labs (based on clinical suspicion)
- Sputum: Gram stain/culture, AFB smear/culture, cytology
- Urinalysis + microscopy: pulmonary-renal syndromes
- Serology: ANCA (MPO, PR3), anti-GBM (Goodpasture), ANA, dsDNA, complement, cryoglobulins
- BNP/NT-proBNP: LV failure
- ECG/echo: structural heart disease
Imaging
- Chest CT (with/without contrast): Indicated if diagnosis uncertain after initial evaluation
- CT angiography: best for vascular causes (AVM, aneurysm) and pre-embolization planning; identifies source with high sensitivity; may be better than bronchoscopy for etiology/source in stable patients
- Detects up to 96% of CXR-occult malignancies
- Limited for subtle mucosal lesions
- CT is not appropriate in hemodynamically unstable patients - proceed directly to bronchoscopy
Bronchoscopy
-
Localizes/lateralizes bleeding source in >66% of cases
-
Yield is highest when performed during or within 48 hours of active bleeding
-
Indications:
- Source unclear after imaging
- Persistent or recurrent hemoptysis
- Suspected airway abnormality
- Risk factors for bronchogenic carcinoma (male sex, age >40, >40 pack-year, hemoptysis >1 week, volume >30 mL)
- Obtaining biopsy if malignancy suspected
- Pre-embolization localization
- Evaluation for alveolar hemorrhage
-
Washington Manual of Medical Therapeutics, p. 382
Step 6 - Management
Algorithm
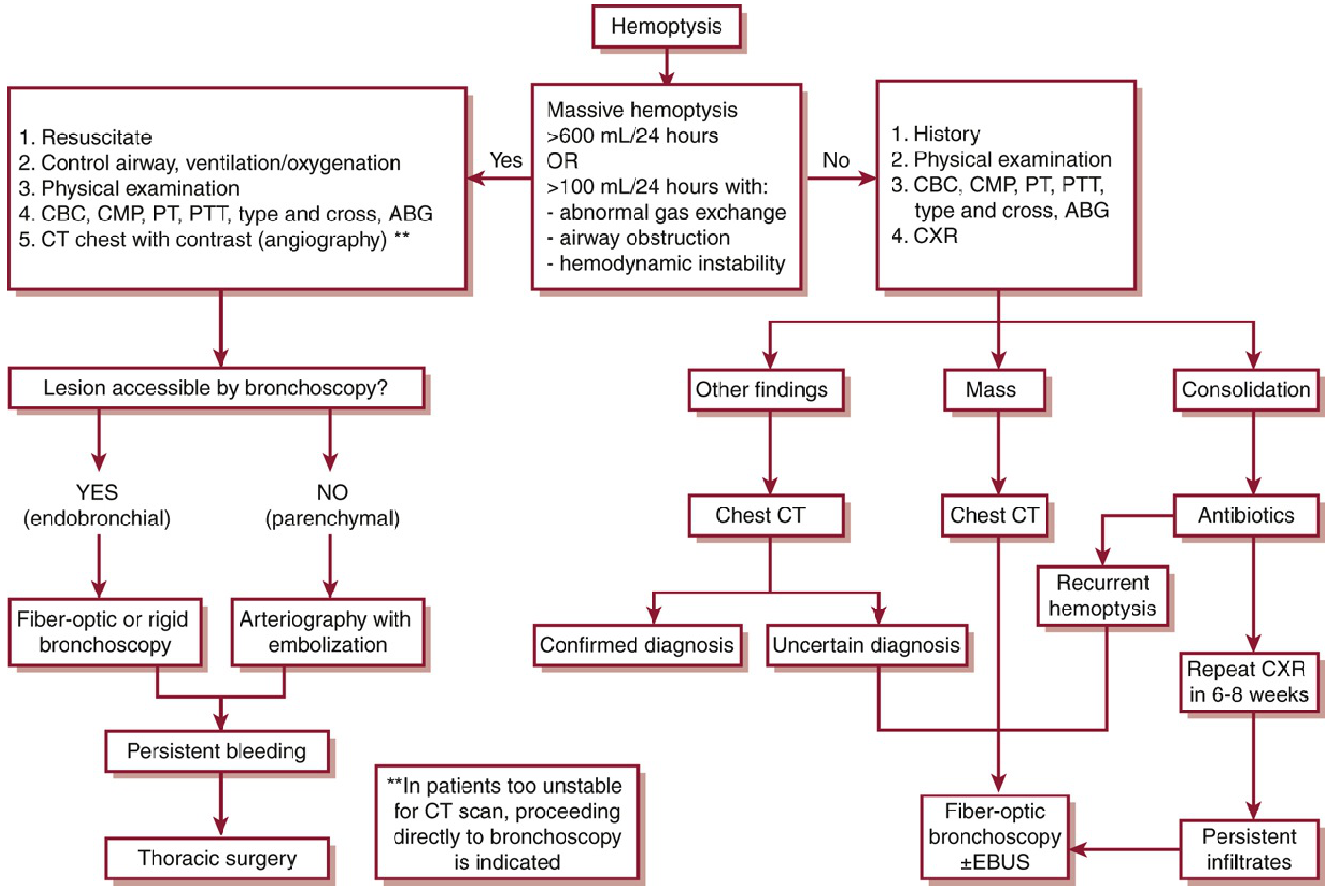
Algorithm for evaluation of hemoptysis (Washington Manual of Medical Therapeutics, adapted from Earwood & Thompson, Am Fam Physician 2015)
Non-Massive Hemoptysis (conservative approach)
- Identify and treat the underlying cause
- Reversal of coagulopathy (correct platelets, INR)
- Antitussives (reduce irritation and minor mucosal trauma)
- Antibiotics (for infection, including TB, fungal disease, NTM)
- Steroids/immunosuppression (vasculitis, DAH, Goodpasture)
- Diuretics/inotropes (LV failure, mitral stenosis)
- Bronchoscopy if recurrent or cause unclear
- Follow-up CXR at 6-8 weeks for persistent infiltrate
Massive Hemoptysis (emergency - multidisciplinary approach)
Team: interventional pulmonologist + thoracic surgeon + interventional radiologist
1. Immediate Stabilization
- Position: lateral decubitus with bleeding lung DOWN - prevents aspiration into the unaffected lung
- Airway protection: early intubation with a large-bore (>8 mm) endotracheal tube
- Single-lumen mainstem intubation into the unaffected bronchus (selective ventilation)
- Double-lumen tube under skilled supervision
- Supplemental oxygen, hemodynamic resuscitation
- Inhaled tranexamic acid (nebulized): emerging evidence supports reduction in expectorated volume, hospital stay, and recurrence rates (PMID 39841268)
2. Bronchoscopy
- Rigid bronchoscopy preferred in massive hemoptysis: better airway control, suctioning, and instrument access
- Flexible bronchoscopy also used, especially for localization
- Endobronchial interventions:
- Direct tamponade with bronchoscope tip
- Balloon tamponade (Fogarty/bronchial blocker balloon, left 1-2 days; monitor for mucosal ischemia)
- Topical hemostatics: cold saline, topical epinephrine, vasopressin, thrombin, oxidized regenerated cellulose
- Electrocautery / argon plasma coagulation (APC): for endobronchial lesions
- Nd:YAG laser, endobronchial stent
3. Bronchial Artery Embolization (BAE)
- First-line definitive procedure for massive hemoptysis
- Success rate >75-90% acutely (up to >85% with careful localization)
- Most effective when CT angiography is used for pre-procedural planning
- Rebleeding rate: 20-50% at 1 year; usually responds to repeat embolization
- Rebleeding more common in: sarcoidosis, malignancy, aspergilloma
- Complications: post-embolization syndrome (pleuritic pain, fever, dysphagia, leukocytosis, 5-7 days, self-limited), bronchial/partial pulmonary infarction, and rarely ischemic myelopathy (spinal artery inadvertent embolization)
- Failure usually due to incomplete source vessel identification; post-embolization arteriography may reveal additional culprit vessels from intercostal/phrenic arteries
4. Surgery
-
Indicated when bronchoscopic and embolization strategies fail
-
Better outcomes when done electively (non-urgently) after embolization allows stabilization
-
Emergency surgery carries high mortality
-
Also indicated for: Aspergillus-related cavitary lesions (after granulocytopenia resolves), post-lobectomy hemothorax emptying into airways
-
Fishman's Pulmonary Diseases and Disorders, p. 445-446; Harrison's Internal Medicine 22e, p. 635; Washington Manual, p. 383-384
Special Situations
| Scenario | Key Points |
|---|---|
| Aspergilloma | Risk of massive hemoptysis as cavity erodes bronchial/pulmonary vessels; surgical evaluation recommended when granulocytopenia resolves; embolization useful |
| Tuberculosis | Rasmussen aneurysm (pulmonary artery pseudo-aneurysm eroding into TB cavity) - potentially fatal; selective embolization or emergency surgical resection |
| Anti-VEGF therapy (bevacizumab, ramucirumab) | Life-threatening hemoptysis in NSCLC, especially squamous cell histology with cavitary lesions; contraindicated with recent hemoptysis |
| Catamenial hemoptysis | Endometrial tissue in lower airways; hormonal suppression or surgery |
| Goodpasture / DAH | Life-threatening; requires steroids + cyclophosphamide ± plasmapheresis |
| CF | Embolization particularly useful; high rebleeding risk |
| PE with infarction | Hemoptysis is not an indication to withhold anticoagulation; however, co-existing lung cancer or bronchiectasis may necessitate IVC filter |
Summary: The 3 Goals of Management
- Stabilize airway and hemodynamics (position, intubate, oxygenate)
- Diagnose cause and localize bleeding source (history, CXR, CT, bronchoscopy, arteriography)
- Target therapy (treat underlying cause; BAE first-line for massive; surgery as salvage)
Key sources: Fishman's Pulmonary Diseases, p. 443-446; Harrison's Internal Medicine 22e, p. 635; Washington Manual of Medical Therapeutics, p. 378-384; Frameworks for Internal Medicine, p. 625-626
Approach to dyspnea
Finding Sources
Searching PubMed
dyspnea evaluation management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have very rich content from Murray & Nadel's full dyspnea chapter. I also got the Table 36.1 (quality-physiology-disease), Table 36.2 (physical exam findings), and the 4 physiologic mechanisms. I have enough for a comprehensive response. Let me now compile everything.
Approach to Dyspnea
Definition
Dyspnea is a subjective experience of breathing discomfort comprised of qualitatively distinct sensations that vary in intensity. The experience derives from interactions among multiple physiological, psychological, social, and environmental factors (American Thoracic Society consensus definition).
It is distinct from objective signs of respiratory distress (tachypnea, accessory muscle use) which can be observed by others. The patient's report is what defines dyspnea.
"Air hunger," "unable to get enough air," "can't take a deep breath," "chest tightness," "heavy breathing," "smothering" - all are valid descriptions. The specific quality matters clinically.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 854
Epidemiology and Importance
- Up to 25% of middle-aged and older adults suffer from dyspnea
- Present in 16% of non-critically ill hospitalized patients in the first 24 hours; 23% of ED admissions; 49% of critically ill patients
- Dyspnea is an independent predictor of mortality in cardiorespiratory disease
- Patients often gradually limit activity to avoid dyspnea, leading to deconditioning - which in turn worsens dyspnea: a vicious cycle
Pathophysiology: 4 Mechanisms of Dyspnea
Understanding mechanism helps predict the quality of the symptom and identify the cause:
1. Abnormal Blood Gases (Chemoreceptor Stimulation)
- Hypercapnia is a more potent driver of dyspnea than hypoxemia
- Hypoxemia alone causes relatively low-intensity dyspnea
- A-(A-a)PO₂ gradient: if elevated (>0.3 × age), gas exchanger abnormality is contributing
- Sensation: "air hunger," urge to breathe, "I cannot get enough air"
2. Receptor Stimulation (Afferent Signals)
- Pulmonary C-fibers (juxtacapillary receptors): triggered by inflammation, inhaled chemicals/toxins, increased pulmonary capillary pressure (LV failure)
- Rapidly adapting stretch receptors (irritant receptors): triggered by lung deflation/atelectasis → intense need to take a deep breath; also respond to bronchospasm → "chest tightness"
- Slowly adapting stretch receptors: activated by large tidal volumes → may reduce air hunger (basis for pursed-lip breathing benefit)
- Pulmonary vascular pressure receptors: contribute to dyspnea in PE, pulmonary HTN, LV failure
- Metaboreceptors in skeletal muscle: stimulated by low oxygen delivery in exercise limitation and heart failure → "breathing more" quality
3. Increased Mechanical Load on the Respiratory System
- Increased airway resistance: COPD, asthma
- Decreased respiratory system compliance: ILD, pulmonary edema, obesity, kyphoscoliosis
- Sensation: "increased work or effort to breathe"
4. Neuromuscular Weakness
-
System cannot handle even normal mechanical loads
-
Guillain-Barré, myasthenia gravis, diaphragm paralysis, spinal cord injury
-
Sensation: "increased effort" with rapid shallow breathing
-
Murray & Nadel's Textbook of Respiratory Medicine, p. 855-859
The Language of Dyspnea (Diagnostic Clues)
The quality of dyspnea is a key clinical tool:
| Quality of Dyspnea | Physiology | Typical Disease States |
|---|---|---|
| Air hunger / urge to breathe / "need more air" | Chemoreceptor stimulation (hypercapnia, hypoxia) | Pneumonia, pulmonary edema, PE, COPD exacerbation, asthma, pleural effusion |
| Chest tightness | Pulmonary receptor (irritant receptor) stimulation | Asthma, pulmonary edema with bronchospasm |
| Cannot get a deep breath | Respiratory controller stimulation; dynamic hyperinflation | COPD, asthma |
| Increased work / effort to breathe | Mechanical load; neuromuscular weakness | COPD, asthma, obesity, kyphoscoliosis, Guillain-Barré, myasthenia gravis |
| Breathing more / heavy breathing | Increased ventilation; metaboreceptor stimulation | Exercise, cardiovascular deconditioning |
- Murray & Nadel's Textbook of Respiratory Medicine, Table 36.1
Special Forms of Dyspnea
| Term | Description | Key Associations |
|---|---|---|
| Orthopnea | Dyspnea worsening on lying supine | LV failure (increased venous return), COPD, bilateral diaphragm paralysis (instant orthopnea), AVM, bronchiectasis |
| Paroxysmal nocturnal dyspnea (PND) | Episodes waking patient from sleep | LV failure (classic); also COPD (secretion pooling, increased airway resistance), nocturnal aspiration |
| Platypnea | Dyspnea in the upright position (improved supine) | Pulmonary vascular shunting, hepatopulmonary syndrome, intracardiac shunt |
| Trepopnea | Dyspnea in one lateral decubitus position | Unilateral lung or pleural disease, heart failure |
| Orthodeoxia | Desaturation on standing (accompanies platypnea) | Hepatopulmonary syndrome, intracardiac shunt |
| Kussmaul breathing | Deep, labored hyperventilation (increased rate and depth) | Metabolic acidosis (DKA, lactic acidosis, salicylates, renal failure) |
- Murray & Nadel's, p. 3487; Goldman-Cecil, p. 2519
Differential Diagnosis
By Onset and Time Course
Acute (minutes to hours) - EMERGENCY causes first:
- Pulmonary embolism
- Acute myocardial infarction / ACS
- Acute pulmonary edema (LV failure, flash pulmonary edema)
- Tension pneumothorax
- Pericardial tamponade
- Acute severe asthma / status asthmaticus
- Anaphylaxis
- Upper airway obstruction (foreign body, angioedema, epiglottitis)
- Acute respiratory distress syndrome (ARDS)
- Severe hypertensive emergency
- Drug overdose (salicylates, opioids → respiratory failure)
Subacute (days to weeks):
- Pneumonia, pleural effusion
- Worsening heart failure or COPD exacerbation
- Pericardial effusion
- Anemia
Chronic (weeks to months):
- COPD, asthma, ILD
- Heart failure (LV or RV dysfunction)
- Pulmonary arterial hypertension
- Valvular heart disease (especially mitral or aortic)
- Obesity-hypoventilation syndrome
- Deconditioning
- Severe anemia
- Neuromuscular disease (ALS, myasthenia gravis, Guillain-Barré)
- Malignancy (endobronchial, pleural, mediastinal)
- Thyroid disease (hypothyroidism → pleural/pericardial effusion, hyperthyroidism → high-output state)
- Psychogenic / hyperventilation syndrome
By Organ System
| System | Causes |
|---|---|
| Airway | Asthma, COPD, bronchiectasis, upper airway obstruction, foreign body, vocal cord dysfunction |
| Pulmonary parenchyma | Pneumonia, ILD, ARDS, pulmonary edema (cardiogenic/non-cardiogenic), lung cancer |
| Pleural | Effusion, pneumothorax, empyema, mesothelioma |
| Pulmonary vascular | PE, pulmonary arterial hypertension, AVM, pulmonary veno-occlusive disease |
| Cardiac | LV failure, RV failure, ACS, valvular disease, tamponade, pericarditis, arrhythmia |
| Chest wall / neuromuscular | Kyphoscoliosis, obesity, Guillain-Barré, myasthenia gravis, ALS, diaphragm paralysis, cervical cord injury |
| Hematologic/metabolic | Anemia, metabolic acidosis (DKA, uremia), thyrotoxicosis, sepsis |
| Psychogenic | Anxiety, panic disorder, hyperventilation syndrome, sighing dyspnea |
Diagnostic Approach
Step 1: Is This an Emergency? (Rule Out Life-Threatening Causes)
Immediately assess: airway, breathing, circulation, SpO₂
Red flags requiring immediate action:
- SpO₂ <90%, stridor, accessory muscle use, cyanosis, altered mental status
- Hemodynamic instability, diaphoresis, unilateral absent breath sounds
- Signs of obstructive shock (elevated JVP + hypotension + clear lungs → tamponade/tension PTX)
Step 2: History
Key questions:
- Onset: sudden (PTX, PE, acute MI, foreign body) vs. gradual (CHF, COPD, ILD)
- Time course: acute, subacute, chronic, episodic (asthma), progressive
- Severity: exertional only? At rest? Functional impairment (MRC scale: how many stairs, flat ground distance, dressing, eating)
- Quality: "air hunger" vs. "tight chest" vs. "cannot breathe deeply" vs. "effort" - guides physiology
- Positional: orthopnea (CHF), platypnea (hepatopulmonary syndrome)
- Nocturnal: PND (CHF), nocturnal asthma
- Associated symptoms:
- Chest pain → ACS, PE, pneumothorax, pericarditis
- Cough/wheezing → asthma, COPD, heart failure
- Fever/productive cough → pneumonia, bronchitis
- Leg edema → heart failure, DVT/PE
- Palpitations → arrhythmia, thyrotoxicosis
- Weight loss → malignancy, COPD, cardiac cachexia
- Triggers: allergens/dust/exercise/cold air (asthma), occupational/environmental exposures (hypersensitivity pneumonitis, occupational asthma)
- Medical history: prior CHF, COPD, malignancy, PE/DVT, connective tissue disease, HIV
- Medications: beta-blockers (mask tachycardia; can trigger bronchospasm), ACE inhibitors (cough), amiodarone (pulmonary toxicity), methotrexate (pneumonitis), bleomycin (ILD)
- Social history: smoking (COPD, lung cancer), occupation, travel (PE risk), IV drug use (septic emboli, endocarditis)
Step 3: Physical Examination
Findings and their physiologic significance:
| Finding | Physiology | Likely Diagnoses |
|---|---|---|
| Tachypnea + accessory muscle use | Increased respiratory drive | Pneumonia, pulmonary edema, PE, COPD exacerbation, asthma |
| Wheezes | Airway narrowing | Asthma, COPD, cardiac asthma (heart failure) |
| Stridor | Upper airway obstruction | Foreign body, angioedema, epiglottitis, laryngeal mass |
| Crackles/rales | Reduced lung compliance | ILD, pneumonia, pulmonary edema |
| Rhonchi | Airway inflammation/secretions | Pneumonia, bronchitis |
| Dullness to percussion | Absent air | Pleural effusion, dense consolidation |
| Hyperresonance | Absent lung tissue | Pneumothorax, bullous emphysema |
| Pulsus paradoxus | Severe airway obstruction or tamponade | Asthma, COPD, cardiac tamponade |
| JVD + peripheral edema + S3 | Elevated venous pressure | Right or biventricular heart failure |
| Mitral regurgitation / AS murmur | Valvular disease | Valvular heart disease causing pulmonary HTN |
| Kussmaul breathing | Metabolic acidosis compensatory hyperventilation | DKA, lactic acidosis, renal failure, salicylate toxicity |
| Paradoxical abdominal motion | Diaphragm paralysis | Phrenic nerve injury, ALS |
| Cyanosis | Severe hypoxemia or methemoglobinemia | Multiple severe causes |
| Clubbing | Chronic hypoxia | COPD, ILD, malignancy, bronchiectasis, cyanotic heart disease |
- Murray & Nadel's Textbook of Respiratory Medicine, Table 36.2
Step 4: Initial Investigations (All Patients)
| Investigation | Key Findings |
|---|---|
| SpO₂ / Pulse oximetry | First-line; note: normal SpO₂ does NOT exclude PE or early ILD |
| CXR (PA + lateral) | Cardiomegaly, effusions, infiltrates, pneumothorax, hyperinflation, masses |
| ECG | Sinus tachycardia, RV strain (S1Q3T3, new RBBB) → PE; ischemic changes → ACS; LVH → HTN heart disease; arrhythmias |
| CBC | Anemia (Hb <7 g/dL typically causes exertional dyspnea); leukocytosis → infection |
| BMP / CMP | Renal failure (metabolic acidosis), glucose (DKA), electrolytes |
| ABG | PaO₂, PaCO₂, pH; A-a gradient (>0.3 × age = gas exchanger problem); respiratory vs. metabolic acidosis; CO poisoning (carboxyhemoglobin) |
| BNP / NT-proBNP | BNP <100 pg/mL effectively excludes heart failure as cause; BNP >400 strongly suggests HF |
| D-dimer | If PE pre-test probability is low-intermediate; negative rules out PE with high sensitivity |
| Troponin | ACS, myocarditis, RV strain from PE |
Step 5: Targeted Investigations (Based on Working Diagnosis)
| Suspected Cause | Additional Tests |
|---|---|
| Heart failure / cardiac | Echocardiography (EF, valves, wall motion, RVSP), cardiac MRI |
| COPD / asthma | Spirometry (FEV₁/FVC <0.70 post-BD = obstructive), bronchodilator reversibility, DLCO, peak flow |
| PE | CT pulmonary angiography (gold standard), V/Q scan, lower limb Doppler USS, echocardiography (RV strain) |
| ILD / parenchymal | HRCT chest, DLCO (reduced out of proportion to FVC), bronchoscopy with BAL, lung biopsy |
| Pulmonary HTN | Echo (estimate RVSP), right heart catheterization, V/Q scan (to exclude CTEPH) |
| Neuromuscular | Sniff nasal inspiratory pressure (SNIP), maximal inspiratory/expiratory pressures (MIP/MEP), NCS/EMG, diaphragm fluoroscopy ("sniff test") |
| Anemia | Reticulocyte count, iron studies, B12/folate, hemolysis workup |
| Metabolic | Thyroid function tests, lactate, arterial blood gas |
| Malignancy | CT chest/abdomen/pelvis, bronchoscopy, biopsy |
| Unexplained exertional | Cardiopulmonary exercise testing (CPET) - identifies whether limitation is cardiac, pulmonary, deconditioning, or effort-related |
CPET is particularly valuable when both cardiac and respiratory problems are present, or when no cause is found after standard evaluation.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 860
Management
Management is directed at the underlying cause. Symptomatic treatment is also important, especially in chronic or end-stage disease.
Disease-Specific Treatment
- Asthma/COPD: bronchodilators (SABA, LAMA, ICS), pulmonary rehabilitation
- Heart failure: diuretics (furosemide), ACE inhibitors/ARBs, beta-blockers, SGLT2 inhibitors
- PE: anticoagulation, thrombolysis (massive PE), embolectomy
- Pneumonia: antibiotics, oxygen supplementation
- Pleural effusion/PTX: thoracentesis, chest drain
- Anemia: treat cause; transfusion for severe/symptomatic
- ILD: corticosteroids (some subtypes), antifibrotics (pirfenidone, nintedanib for IPF)
- Pulmonary HTN: PDE5 inhibitors, endothelin antagonists, prostacyclins
Symptomatic (Non-Disease-Specific) Treatment
| Intervention | Mechanism | Notes |
|---|---|---|
| Oxygen | Reduces hypoxic drive and receptor stimulation | Most effective when SpO₂ <88%; limited benefit when normoxic |
| Opioids (low-dose morphine) | Decrease respiratory drive; reduce perception | Effective for end-stage lung disease; does not significantly worsen ventilation at dyspnea doses; useful in acute severe asthma/COPD to break hyperinflation-dyspnea-anxiety cycle |
| Benzodiazepines | Reduce anxiety component | Limited evidence; may help hyperventilation syndrome and anxiety-related dyspnea |
| Fan directed at face | Stimulates facial cold receptors → reduces dyspnea perception | Low-cost, non-pharmacologic; evidence-based in COPD and cancer |
| Pulmonary rehabilitation | Desensitizes dyspnea, improves muscle efficiency, reduces deconditioning cycle | First-line in COPD, beneficial in ILD and CHF |
| Cognitive behavioral therapy | Addresses psychological component | Hyperventilation syndrome, anxiety, dyspnea catastrophizing |
| Pursed-lip breathing / breathing retraining | Activates slowly adapting stretch receptors → reduces air hunger; reduces dynamic hyperinflation | COPD, emphysema |
Dyspnea in End-Stage / Palliative Setting
-
Goals of care shift from prolonging life to maximizing comfort
-
Low-dose oral/parenteral opioids are the most evidence-based pharmacologic intervention
-
Coordination of pulmonary and palliative care improves breathlessness mastery and prolongs survival
-
Fear of opioid-induced respiratory depression should not prevent their use at appropriate dyspnea-relief doses
-
Murray & Nadel's Textbook of Respiratory Medicine, p. 862-863
Quantifying Dyspnea: Validated Scales
| Scale | Use |
|---|---|
| MRC Dyspnea Scale (1-5) | Chronic functional impairment; used in COPD |
| Borg Scale (0-10) | Acute/exercise dyspnea intensity |
| mMRC (modified MRC) | COPD staging (part of GOLD criteria, CAT score) |
| Pulmonary Functional Status and Dyspnea Questionnaire | Research and chronic disease monitoring |
| Visual Analogue Scale (VAS) | Simple 0-100 mm subjective rating |
Summary Framework
DYSPNEA
|
├─ EMERGENCY? (SpO₂, HR, BP, RR, appearance)
| YES → immediate stabilization (O₂, IV access, monitor)
| → CXR, ECG, ABG, troponin, BNP, D-dimer
| → Treat: PTX drain / pericardiocentesis / thrombolysis / diuretics / bronchodilators
|
├─ HISTORY → onset / quality / position / triggers / associated symptoms
|
├─ 4 MECHANISMS → blood gases / receptor stimulation / mechanical load / neuromuscular
|
├─ INITIAL TESTS → SpO₂, CXR, ECG, CBC, BMP, BNP, ABG
|
├─ TARGETED TESTS → echo / CT-PA / spirometry / HRCT / CPET
|
└─ TREATMENT → disease-specific + symptomatic (O₂, opioids, rehab, fan)
Key sources: Murray & Nadel's Textbook of Respiratory Medicine, p. 854-863 (Chapter 36); Goldman-Cecil Medicine, p. 2516-2520; Guyton & Hall Medical Physiology, p. 548-549; Fishman's Pulmonary Diseases and Disorders
Create a image with revision of pneumonia. Include everything required for theory exam
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Generating Image
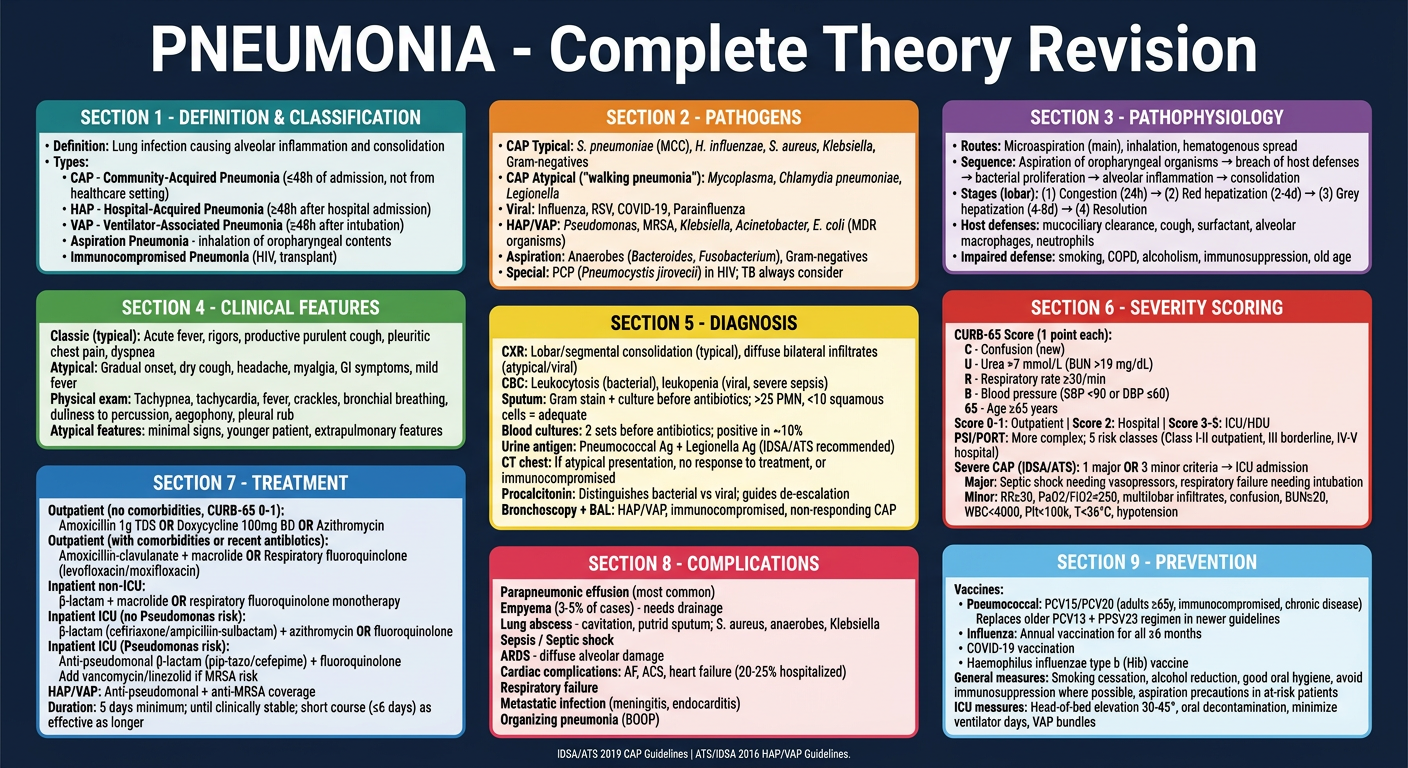
Here is your complete pneumonia revision poster. It covers all the key theory exam topics:
- Definition & Classification - CAP, HAP, VAP, aspiration, immunocompromised
- Pathogens - typical, atypical, viral, HAP/VAP MDR organisms, special populations
- Pathophysiology - routes of infection, 4 stages of lobar pneumonia (congestion → red hepatization → grey hepatization → resolution), host defense mechanisms
- Clinical Features - typical vs atypical presentation, physical examination signs
- Diagnosis - CXR patterns, sputum, blood cultures, urine antigens, procalcitonin, BAL
- Severity Scoring - full CURB-65 criteria with score-based management, PSI/PORT, IDSA/ATS severe CAP major and minor criteria
- Treatment - stratified outpatient/inpatient/ICU regimens, HAP/VAP, MRSA/Pseudomonas coverage, duration of therapy
- Complications - empyema, lung abscess, ARDS, cardiac complications (seen in 20-25%)
- Prevention - pneumococcal vaccine schedule, influenza, VAP bundle
Create similar revision poster for bronchial asthma and COPD separately
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Generating Image
Generating Image
How much time will it take
The two posters will take about 1-2 minutes to generate. I'll create them both at the same time (in parallel), so you won't be waiting twice.
Shall I go ahead now?
Generate both asthma and COPD revision posters now
Generating Image
Generating Image
Stop generating image
Stopped. The image generation has been cancelled.
Would you like me to do something different instead? For example, I can:
- Write out the revision notes as text for both Asthma and COPD (formatted, detailed, exam-ready)
- Create a downloadable PDF or Word document with the revision content
- Create a PowerPoint presentation with the revision slides
- Answer specific questions about Asthma or COPD
What would you prefer?
Create comprehensive text revision notes for Asthma and COPD
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Make a downloadable pdf
Reading File
Running Command
This is a shared conversation. Sign in to Orris to start your own chat.