respiratory alkalosis management
Reading File
Finding Sources
Searching PubMed
"respiratory alkalosis" management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of respiratory alkalosis management drawn from multiple authoritative textbooks.
Respiratory Alkalosis: Management
Pathophysiology Recap
Respiratory alkalosis results from alveolar hyperventilation → ↓PaCO₂ → ↑pH. Two phases of compensation occur:
- Acute (minutes–hours): Non-bicarbonate cellular buffers reduce HCO₃⁻ by ~2 mEq/L per 10 mmHg ↓PaCO₂
- Chronic (2–5 days): Renal compensation ↓ HCO₃⁻ by 4–5 mEq/L per 10 mmHg ↓PaCO₂ (can be fully compensated, unlike other disorders)
Common Causes (to guide therapy)
| Category | Examples |
|---|---|
| Respiratory | Hypoxemia (PE, pneumonia, asthma), mechanical hyperventilation |
| CNS | Anxiety/panic, brain lesions, pain |
| Drugs/Toxic | Salicylates (direct medullary stimulation), theophylline, progesterone, catecholamines |
| Systemic illness | Sepsis, hepatic failure, circulatory failure |
| Metabolic | Fever, hyperthyroidism |
| Physiologic | Pregnancy, high altitude |
Core Management Principle
Treatment is directed at the underlying cause. Respiratory alkalosis itself is rarely life-threatening, and direct measures to correct the alkalosis will fail if the underlying stimulus is not addressed. — Brenner & Rector's The Kidney
Management by Scenario
1. Hypoxemia-Driven Hyperventilation
- Correct hypoxemia with supplemental oxygen
- Treat the underlying cause (PE, pneumonia, etc.)
2. Anxiety / Hyperventilation Syndrome
- Diagnosis of exclusion — rule out PE, coronary artery disease, pneumothorax, hyperthyroidism
- Reassurance and removal of stressors
- Breathing retraining — diaphragmatic (abdominal) breathing
- ❌ Rebreathing into a paper bag is no longer recommended — can cause significant hypoxemia, especially with underlying cardiorespiratory disease (Comprehensive Clinical Nephrology)
- Short-acting benzodiazepines (small doses) if conservative treatment fails
- Long-term: cognitive behavioral therapy (CBT), identify and treat underlying panic disorder
- β-blockers may help with peripheral hyperadrenergic symptoms in select patients; antidepressants and sedatives are generally not recommended
3. Mechanically Ventilated Patients
- Reduce tidal volume and/or respiratory rate
- Add dead space to the circuit
- Change ventilation mode (e.g., assist-control → mandatory ventilation)
- Ensure adequate sedation and analgesia (pain/agitation drives tachypnea)
- If persistent: sedation ± skeletal muscle paralysis
4. Salicylate Toxicity
- Induced emesis / gastric lavage
- Activated charcoal with sorbitol
- Forced diuresis with urinary alkalinization
- Hemodialysis for severe poisoning
5. Sepsis / Hepatic / Circulatory Failure
- Specific measures tailored to the underlying cause (source control, antibiotics, liver support)
6. High-Altitude / Mountain Sickness
- Acetazolamide prophylactically — induces a metabolic acidosis that prevents extreme pH elevation; monitor K⁺ to avoid hypokalemia
7. Advanced Renal Failure / Fluid Overload / CHF
- Dialysis or ultrafiltration with alkali supplementation
8. Severe Alkalemia (pH > 7.60)
- Rare scenario; consider IV hydrochloric acid, arginine chloride, or ammonium chloride (Morgan & Mikhail's Clinical Anesthesiology)
Management Flowchart
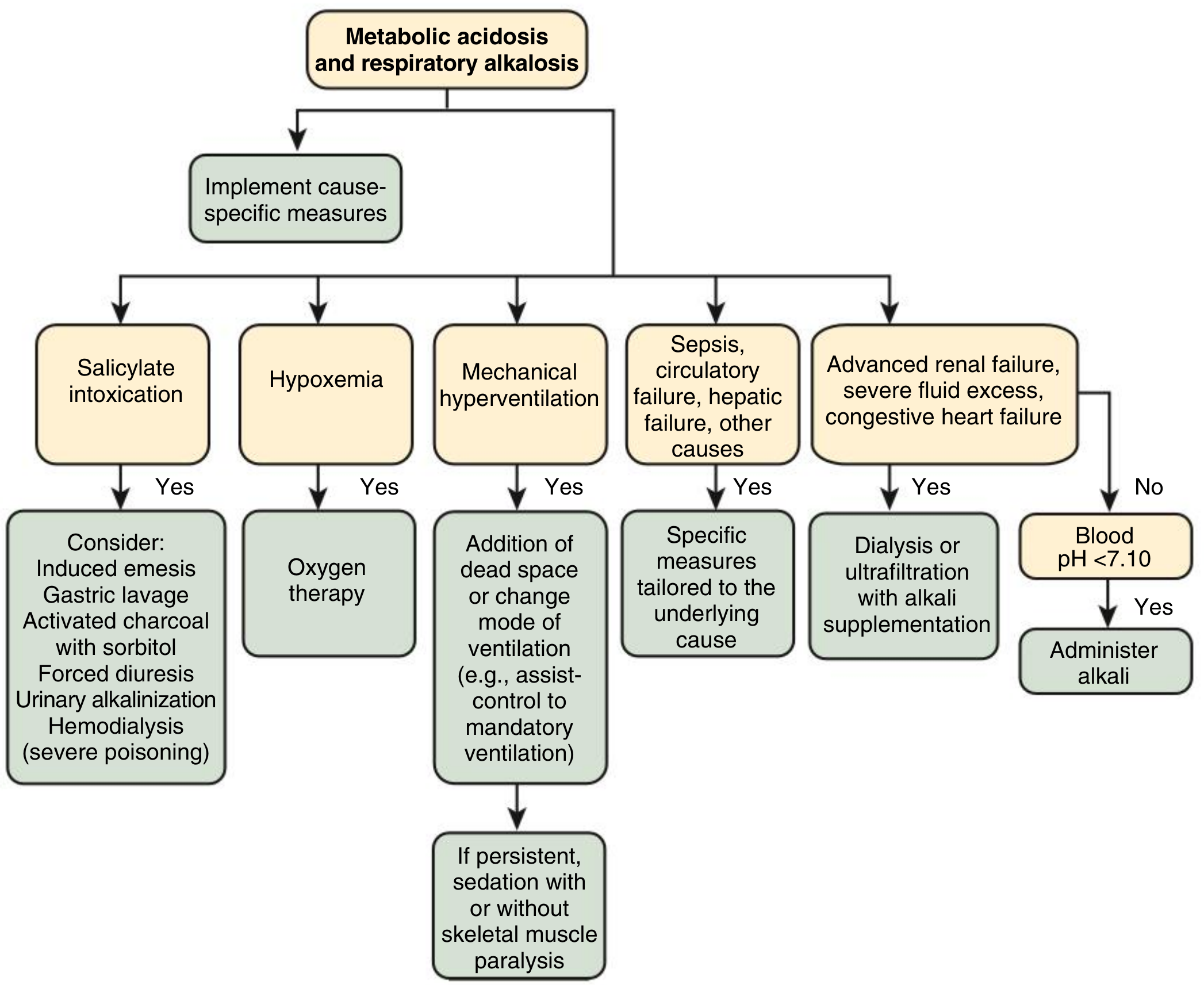
Fig. 15.9 — Treatment pathways for respiratory alkalosis by underlying cause. Comprehensive Clinical Nephrology, 7th Ed.
Electrolyte Monitoring
- K⁺: Usually mildly ↓ (intracellular shift); generally does not need specific treatment
- Cl⁻: ↑ (hyperchloremia accompanies chronic compensation)
- Ionized Ca²⁺: ↓ in acute phase (increased albumin binding) → causes perioral paresthesias, carpopedal spasm, tetany; resolves as pH normalizes
- Phosphate: Can fall (hypophosphatemia); improves with treatment of the alkalosis
Key Compensatory Formulas
| Disorder | Expected compensation |
|---|---|
| Acute respiratory alkalosis | HCO₃⁻ ↓ 2 mEq/L per 10 mmHg ↓PaCO₂ |
| Chronic respiratory alkalosis | HCO₃⁻ ↓ 4–5 mEq/L per 10 mmHg ↓PaCO₂ |
| Minimum HCO₃⁻ in pure resp. alkalosis | ~12 mEq/L (acute); ~16 mEq/L (chronic) |
If HCO₃⁻ falls below these thresholds, suspect a concurrent metabolic acidosis.
Sources: Brenner & Rector's The Kidney; Murray & Nadel's Respiratory Medicine; Comprehensive Clinical Nephrology, 7th Ed.; Goldman-Cecil Medicine; Rosen's Emergency Medicine; Morgan & Mikhail's Clinical Anesthesiology, 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.