different essential cariac markers
Reading File
Finding Sources
Finding Sources
Searching the Web
essential cardiac biomarkers myocardial infarction troponin CK-MB BNP 2024
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have enough information from the textbooks and web sources to give a thorough answer. Here it is:
Essential Cardiac Markers
Cardiac markers (biomarkers) are substances released into the bloodstream when the heart muscle is damaged or stressed. They are used primarily for diagnosing acute coronary syndrome (ACS), risk stratification, and monitoring heart failure.
1. Cardiac Troponins (cTnI and cTnT) - Gold Standard
Troponins I and T are structural proteins of the cardiac sarcomere responsible for regulating the actin-myosin interaction. They are found both within the sarcomere and in small concentrations in the cytosol of cardiomyocytes.
| Feature | Detail |
|---|---|
| Rises | 3-6 hours after injury |
| Peaks | 12-24 hours |
| Duration | Remains elevated 7-14 days (cTnI) / 10-14 days (cTnT) |
| Specificity | Nearly entirely cardiac in origin - very high cardiac specificity |
| Sensitivity | High; high-sensitivity troponin (hs-cTn) detectable even at very low levels |
Clinical notes:
- Current ESC/ACC guidelines recommend troponin as the only biomarker for diagnosing acute MI. CK-MB is used only when troponin is unavailable.
- hs-cTn assays can reclassify roughly 30% of UA patients to NSTEMI due to higher sensitivity.
- Accelerated diagnostic pathways using hs-cTn can rule out NSTEMI in as little as 1 hour.
- A rise-and-fall pattern (delta troponin) is needed to distinguish acute MI from chronic/non-ischemic elevation.
- Troponin is not specific for the cause of injury - it can be elevated in pulmonary embolism, myocarditis, sepsis, stroke, renal failure, and many other conditions (see causes table below).
Causes of troponin elevation other than ACS:
- Cardiac: heart failure, myocarditis, pericarditis, aortic dissection, Takotsubo (apical ballooning syndrome)
- Neurological: stroke, subarachnoid hemorrhage
- Pulmonary: PE, ARDS
- Systemic: sepsis, rhabdomyolysis, CKD/ESRD, hypothyroidism
- Drugs: chemotherapy, colchicine, carbon monoxide
(Fuster and Hurst's The Heart, 15th Edition, Table 19-3)
2. Creatine Kinase-MB (CK-MB)
CK is an enzyme present in skeletal muscle, brain, and cardiac muscle. The MB isoform is predominant in cardiac tissue.
| Feature | Detail |
|---|---|
| Rises | 4-8 hours after MI |
| Peaks | 18-24 hours |
| Duration | Returns to normal in 48-72 hours |
| Advantage | Useful for detecting reinfarction (returns to baseline faster than troponin) |
| Limitation | Less specific than troponin; elevated in skeletal muscle injury |
CK-MB is now a second-line marker, reserved when troponin testing is not available. Its faster return to baseline makes it useful for diagnosing a second infarct on top of a recent one.
3. B-type Natriuretic Peptide (BNP) and NT-proBNP
BNP is a 32-amino acid peptide secreted primarily by cardiac ventricles in response to wall-stretch (volume/pressure overload). NT-proBNP is an inactive N-terminal cleavage fragment.
| Feature | Detail |
|---|---|
| Primary use | Diagnosis and monitoring of heart failure |
| BNP cutoff | >100 pg/mL suggests HF |
| NT-proBNP cutoff | >125 pg/mL (age-adjusted) suggests HF |
| Prognosis | Elevated BNP/NT-proBNP correlates with HF severity and mortality |
| Limitation | Elevated in ESRD, PE, AF, and other conditions |
(Henry's Clinical Diagnosis and Management by Laboratory Methods)
4. Myoglobin
Myoglobin is an oxygen-binding protein found in both cardiac and skeletal muscle.
| Feature | Detail |
|---|---|
| Rises | Within 1-3 hours (earliest marker) |
| Peaks | 6-9 hours |
| Normalizes | Within 24 hours |
| Advantage | Fastest rising marker - useful for very early rule-out |
| Limitation | Not cardiac-specific (also elevated with skeletal muscle injury) |
Myoglobin is now largely replaced in practice by hs-cTn assays, which can also detect early injury.
5. Lactate Dehydrogenase (LDH) and LDH Isoforms
LDH-1 predominates in cardiac muscle. It was historically used when patients presented late (>24-48h) after MI when CK-MB had already normalized.
| Feature | Detail |
|---|---|
| Rises | 24-48 hours post-MI |
| Duration | Remains elevated 7-14 days |
| LDH-1 > LDH-2 | "Flipped pattern" - historically diagnostic of MI |
| Current use | Largely replaced by troponin in modern practice |
6. Aspartate Aminotransferase (AST)
An older, non-specific marker previously used for MI. Not specific for cardiac tissue (also elevated in liver, skeletal muscle disease). No longer used as a primary cardiac marker.
Comparative Summary Table
| Marker | Rises | Peaks | Normalizes | Cardiac Specificity | Primary Use |
|---|---|---|---|---|---|
| Troponin I/T | 3-6 h | 12-24 h | 7-14 days | Very high | MI diagnosis (gold standard) |
| hs-Troponin | 1-3 h | 12-24 h | 7-14 days | Very high | Rapid MI rule-in/out |
| CK-MB | 4-8 h | 18-24 h | 48-72 h | Moderate | Reinfarction detection |
| Myoglobin | 1-3 h | 6-9 h | ~24 h | Low | Early screening (obsolete) |
| BNP/NT-proBNP | Hours-days | Variable | Varies | Moderate | Heart failure |
| LDH | 24-48 h | 3-6 days | 7-14 days | Low | Late presentation (historical) |
| AST | 8-12 h | 18-36 h | 3-4 days | Very low | Historical only |
Key Clinical Principles
- Serial sampling is required for troponin - a rise-and-fall pattern distinguishes acute MI from chronic elevation. Serial measurement at 0h, 1h, or 3h depending on protocol.
- Troponin is preferred for all ACS - CK-MB is only a backup when troponin assays are unavailable.
- BNP/NT-proBNP are used for heart failure, not ischemia.
- Context matters - an isolated elevated troponin without symptoms or ECG changes requires careful interpretation before labeling it an MI.
- In ESRD patients, baseline troponin is often elevated due to LV hypertrophy and microvascular disease; a dynamic rise of ≥20% from baseline is required to diagnose MI.
Sources: Fuster and Hurst's The Heart, 15th Ed. | Tintinalli's Emergency Medicine | Henry's Clinical Diagnosis and Management by Laboratory Methods | Medscape (2024)
all
Asking for Preferences
Finding Sources
Finding Sources
Searching the Web
complete list all cardiac biomarkers including emerging novel markers 2024 2025
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC11989402
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
I now have comprehensive data from multiple authoritative textbooks. Here is the full expanded list of all cardiac markers:
Complete List of All Cardiac Markers
Cardiac biomarkers can be classified into six major categories based on their mechanism, what they detect, and their primary clinical application.
CATEGORY 1 - Markers of Myocardial Necrosis (Cell Death)
These are released when cardiomyocytes die, indicating actual tissue infarction.
1. Cardiac Troponins I and T (cTnI / cTnT) - GOLD STANDARD
- Source: Sarcomeric proteins of the cardiac contractile apparatus (myofilaments); small amounts also in cytosol
- Function: Regulate actin-myosin interaction in muscle contraction
- Rises: 3-6 hours post-MI
- Peaks: 12-24 hours
- Duration: 7-14 days
- Specificity: Very high - nearly entirely cardiac in origin
- Use: Primary marker for diagnosing MI; risk stratification in ACS/NSTE-ACS
- Key point: Even minor elevations are independently associated with adverse outcomes; does not identify the cause of myocardial injury
2. High-Sensitivity Troponin (hs-cTnI / hs-cTnT)
- Same molecule as above but detected by more analytically precise assays
- Rises: Detectable as early as 1-2 hours
- Advantage: Superior sensitivity at low concentrations; can rule in/out MI in 1 hour (ESC 0h/1h algorithm)
- Impact: Reclassifies ~30% of UA patients to NSTEMI; detectable in virtually 100% of healthy individuals at some concentration
- Limitation: More false positives; requires delta (serial change) interpretation
3. Creatine Kinase-MB (CK-MB)
- Source: Cardiac muscle (predominant source of MB isoform); also small amounts in skeletal muscle (especially pelvic musculature)
- Rises: 3-4 hours post-MI
- Peaks: 18-24 hours
- Normalizes: 48-72 hours
- Advantage: Faster return to baseline makes it useful for detecting reinfarction after an initial MI
- Limitation: Lower cardiac specificity than troponin; elevated in rhabdomyolysis, myositis, muscular dystrophy, vigorous exercise
- Current status: Second-line only - used when troponin is unavailable
(Rosen's Emergency Medicine)
4. Creatine Kinase Total (CK / CPK)
- Source: Skeletal muscle, cardiac muscle, brain, kidney, GI tract
- Rises: 4-8 hours
- Peaks: 24 hours
- Normalizes: 3-4 days
- Specificity: Very low - non-specific for cardiac tissue
- Use: Rarely used alone for cardiac diagnosis; measured alongside CK-MB
5. Myoglobin
- Source: Both cardiac and skeletal muscle (identical immunologically - cannot be distinguished)
- Molecular weight: 17 kDa (small, rapidly diffuses into bloodstream)
- Rises: 1-2 hours (earliest rising marker)
- Peaks: 5-7 hours
- Normalizes: Within 24 hours
- Advantage: Earliest marker; was used for very early rule-out
- Limitation: Not cardiac-specific; elevated in any skeletal muscle injury, trauma, vigorous exercise, renal failure (reduced clearance)
- Current status: Largely obsolete; replaced by hs-cTn
(Rosen's Emergency Medicine)
6. Lactate Dehydrogenase (LDH) / LDH Isoenzymes
- Source: Multiple tissues; LDH-1 predominates in cardiac muscle
- Rises: 24-48 hours post-MI
- Peaks: 3-6 days
- Duration: Elevated up to 7-14 days
- Diagnostic pattern: LDH-1 > LDH-2 ("flipped" ratio) = historically diagnostic of MI
- Historical use: Used when patients presented >24-48h after onset when CK-MB had already normalized
- Current status: Replaced by troponin in modern practice
7. Aspartate Aminotransferase (AST / SGOT)
- Source: Liver, heart, skeletal muscle, brain, kidney
- Rises: 8-12 hours
- Peaks: 18-36 hours
- Normalizes: 3-4 days
- Limitation: Very low cardiac specificity; the AST-to-ALT ratio helps differentiate cardiac vs. hepatic pathology
- Current status: Historical only; no longer used as a cardiac marker
8. Carbonic Anhydrase III (CA-III)
- Source: Skeletal muscle-specific; absent in cardiac tissue
- Use: Used as a corrective marker - if CA-III is elevated alongside CK-MB or myoglobin, the elevation is more likely skeletal in origin, improving cardiac specificity
- Status: Research/adjunctive marker
CATEGORY 2 - Markers of Myocardial Ischemia (Without Necrosis)
These detect ischemia before cell death has occurred.
9. Ischemia-Modified Albumin (IMA)
- Mechanism: During myocardial ischemia, free radicals and metal ions modify the N-terminus of serum albumin, reducing its ability to bind cobalt (detected by the albumin cobalt binding test - FDA approved)
- Rises: Within minutes of ischemia onset; even before myocyte necrosis
- Normalizes: 6-12 hours
- Advantage: Can detect ischemia before troponin rises - the "pre-necrosis" window
- Limitation: Non-specific; elevated in liver disease, infections, cancer
- Use: Adjunctive, not primary; not recommended for routine ED use
10. Heart-Type Fatty Acid-Binding Protein (H-FABP)
- Source: Small cytoplasmic protein abundant in cardiomyocytes
- Rises: Very early (1-2 hours), similar to myoglobin but more cardiac-specific
- Advantage: More cardiac-specific than myoglobin; rises earlier than CK-MB
- Use: Investigated as an early ACS marker and for reinfarction detection
- Status: Research/emerging; not in routine clinical use
11. Unbound Free Fatty Acids / Whole Blood Choline
- Source: Membrane phospholipid breakdown products released during ischemia
- Status: Investigational markers of ischemia; not clinically deployed
CATEGORY 3 - Markers of Hemodynamic Stress / Heart Failure
12. B-type Natriuretic Peptide (BNP)
- Source: Predominantly cardiac ventricles (not the brain, despite the name); also atria to a lesser extent
- Trigger: Released in response to ventricular wall stretch (volume/pressure overload)
- BNP >100 pg/mL: Supports diagnosis of heart failure
- BNP <100 pg/mL: Largely rules out HF
- Primary uses:
- Diagnosis and severity assessment of heart failure
- Prognostic marker in ACS (elevated BNP = higher short-term mortality)
- Monitoring HF therapy response
- Limitation: Elevated in PE, AF, ESRD, RV strain, aging
13. NT-proBNP (N-terminal Pro-BNP)
- Mechanism: Inactive cleavage fragment from the same BNP precursor (pro-BNP)
- Half-life: Longer than BNP (~2 hours vs. ~20 minutes for BNP) - remains elevated longer
- Cutoffs: Age-adjusted:
- <50 years: >450 pg/mL suggests HF
- 50-75 years: >900 pg/mL suggests HF
-
75 years: >1800 pg/mL suggests HF
- Preferred in: Renal patients, serial monitoring
- Note: In ESRD patients on hemodialysis, natriuretic peptides are chronically elevated due to LV hypertrophy; serial changes are more meaningful than absolute values
14. Atrial Natriuretic Peptide (ANP) / MR-proANP
- Source: Cardiac atria in response to atrial stretch
- Use: Less widely used than BNP; MR-proANP (mid-regional fragment) is more stable and used in some European HF protocols
- Status: Adjunctive; not widely available in routine clinical practice
CATEGORY 4 - Inflammatory / Plaque Instability Markers
15. High-Sensitivity C-Reactive Protein (hs-CRP)
- Source: Liver (acute-phase reactant); released in response to systemic inflammation
- Use:
- Long-term cardiovascular risk prediction in healthy individuals (primary prevention)
- hs-CRP >2-3 mg/L = elevated cardiovascular risk
- Used in conjunction with cholesterol scores (e.g., Reynolds Risk Score)
- Limitation: Non-specific; elevated in any infection, autoimmune disease, trauma
- NOT recommended for acute ED evaluation of ACS
16. Myeloperoxidase (MPO)
- Source: Abundant leukocyte enzyme found in vulnerable/ruptured coronary plaques
- Mechanism: Reflects oxidative stress and active plaque inflammation
- Key finding: Elevated MPO predicts short-term adverse cardiac events even when troponin is negative and there is no evidence of necrosis
- Use: Identifies plaque vulnerability/instability before rupture
- Status: Not yet in routine ED use; primarily investigational/research
17. Interleukin-6 (IL-6)
- Source: Inflammatory cytokine from macrophages and vascular endothelial cells
- Role: Mediates systemic inflammation in atherosclerosis and post-MI
- Use: Research marker; elevated levels predict cardiovascular events
- Status: Not routinely used clinically
18. Pregnancy-Associated Plasma Protein A (PAPP-A)
- Source: Metalloproteinase produced in atherosclerotic plaques
- Role: Activates IGF-1; marker of plaque instability
- Use: Studied as an early ACS marker (rises before troponin in some studies); also a prenatal screening marker
- Status: Investigational for cardiac use
CATEGORY 5 - Adhesion Molecules / Endothelial Markers
These reflect vascular inflammation and endothelial dysfunction:
19. Vascular Cell Adhesion Molecule (VCAM-1)
20. Intercellular Adhesion Molecule (ICAM-1)
21. E-Selectin
22. P-Selectin
- Mechanism: Expressed on activated endothelial cells and platelets during atherosclerotic inflammation; facilitate leukocyte trafficking into plaques
- Use: Studied as markers of vascular inflammation and ACS risk
- Status: Research only; current evidence does not support ED use
(Tintinalli's Emergency Medicine)
CATEGORY 6 - Novel / Emerging Markers
23. Copeptin
- Source: C-terminal fragment of arginine vasopressin (AVP) precursor; released with AVP during physiological stress
- Use: Rises very rapidly with any acute stress including MI; used as an early rule-out marker in combination with troponin
- Key property: A normal copeptin + negative troponin at presentation has high negative predictive value for MI
- Status: Used in some European protocols; FDA approved in some formulations; not widely used in the US
24. ST2 (Soluble ST2)
- Source: Soluble decoy receptor for interleukin-33 (IL-33); reflects myocardial stress, fibrosis, and hypertrophy
- Use: Risk stratification and prognosis in heart failure; elevated ST2 = worse outcomes
- Advantage: Not significantly affected by age, BMI, or renal function (unlike BNP)
- Status: Approved for use in heart failure prognosis; used alongside BNP
25. Galectin-3
- Source: Beta-galactoside-binding lectin secreted by activated macrophages; marker of cardiac fibrosis and remodeling
- Use: Prognosis in heart failure; predicts fibrotic progression
- Status: FDA approved as a prognostic aid in HF; used alongside BNP/NT-proBNP
26. Growth Differentiation Factor-15 (GDF-15)
- Source: Member of TGF-beta family; released from cardiac tissue under oxidative stress, inflammation, and injury
- Use: Risk stratification in ACS and heart failure; elevated GDF-15 = increased mortality risk
- Status: Emerging marker; not yet in routine clinical use
27. MicroRNAs (miR-1, miR-133, miR-208, miR-499)
- Source: Small non-coding RNA molecules released from damaged cardiomyocytes
- Use: Highly cardiac-specific (miR-208 and miR-499 are almost exclusively cardiac); being studied for early MI detection and HF prognosis
- Advantage: Potentially more specific than troponin for cardiac origin
- Status: Research only; not clinically available yet
28. Trimethylamine N-oxide (TMAO)
- Source: Gut microbiome metabolite from dietary choline and carnitine
- Use: Elevated TMAO levels associated with increased risk of major adverse cardiovascular events (MACE)
- Status: Emerging research marker; not in routine clinical use
29. Lipoprotein-Associated Phospholipase A2 (Lp-PLA2)
- Source: Enzyme produced by inflammatory cells within atherosclerotic plaques; cleaves oxidized phospholipids
- Use: Marker of plaque inflammation; predicts cardiovascular events independent of LDH and CRP
- Status: FDA approved for cardiovascular risk assessment; used in primary prevention risk stratification
30. Pentraxin-3 (PTX3)
- Source: Long-chain pentraxin produced locally in the vessel wall (unlike CRP which is hepatic)
- Use: More tissue-specific marker of vascular inflammation than CRP; studied in ACS and HF
- Status: Investigational
Summary Table - All Cardiac Markers
| # | Marker | Category | Rises | Peaks | Normalizes | Cardiac Specificity | Clinical Status |
|---|---|---|---|---|---|---|---|
| 1 | cTnI / cTnT | Necrosis | 3-6 h | 12-24 h | 7-14 days | Very High | Gold Standard |
| 2 | hs-cTnI / hs-cTnT | Necrosis | 1-2 h | 12-24 h | 7-14 days | Very High | Standard of care |
| 3 | CK-MB | Necrosis | 3-4 h | 18-24 h | 48-72 h | Moderate | Second-line |
| 4 | CK total | Necrosis | 4-8 h | 24 h | 3-4 days | Low | Rarely used |
| 5 | Myoglobin | Necrosis | 1-2 h | 5-7 h | 24 h | Low | Obsolete |
| 6 | LDH / LDH-1 | Necrosis | 24-48 h | 3-6 days | 7-14 days | Low | Historical |
| 7 | AST | Necrosis | 8-12 h | 18-36 h | 3-4 days | Very Low | Historical |
| 8 | CA-III | Necrosis | - | - | - | None (skeletal) | Corrective marker |
| 9 | IMA | Ischemia | Minutes | 2-4 h | 6-12 h | Moderate | Investigational |
| 10 | H-FABP | Ischemia/necrosis | 1-2 h | 4-6 h | 24 h | Moderate-High | Emerging |
| 11 | Free fatty acids / choline | Ischemia | Early | - | - | Low | Investigational |
| 12 | BNP | Hemodynamic stress | Hours-days | Variable | Days | Moderate | Standard for HF |
| 13 | NT-proBNP | Hemodynamic stress | Hours-days | Variable | Days | Moderate | Standard for HF |
| 14 | ANP / MR-proANP | Hemodynamic stress | - | - | - | Moderate | Limited use |
| 15 | hs-CRP | Inflammation | Hours | 48-72 h | Days-weeks | Low | Risk stratification |
| 16 | Myeloperoxidase | Plaque instability | - | - | - | Low | Emerging |
| 17 | IL-6 | Inflammation | - | - | - | Low | Research |
| 18 | PAPP-A | Plaque instability | - | - | - | Low | Research |
| 19-22 | VCAM, ICAM, E/P-Selectin | Endothelial | - | - | - | Very Low | Research |
| 23 | Copeptin | Stress response | Minutes | 1-2 h | Hours | Low | Emerging (EU) |
| 24 | ST2 | Fibrosis/remodeling | - | - | - | Moderate | Approved for HF |
| 25 | Galectin-3 | Fibrosis/remodeling | - | - | - | Moderate | Approved for HF |
| 26 | GDF-15 | Stress/injury | - | - | - | Moderate | Emerging |
| 27 | MicroRNAs | Necrosis | - | - | - | Very High | Research only |
| 28 | TMAO | Metabolic | - | - | - | Low | Research |
| 29 | Lp-PLA2 | Plaque inflammation | - | - | - | Low | FDA approved (risk) |
| 30 | Pentraxin-3 | Vascular inflammation | - | - | - | Low | Investigational |
Typical Troponin Rise-and-Fall Pattern After AMI
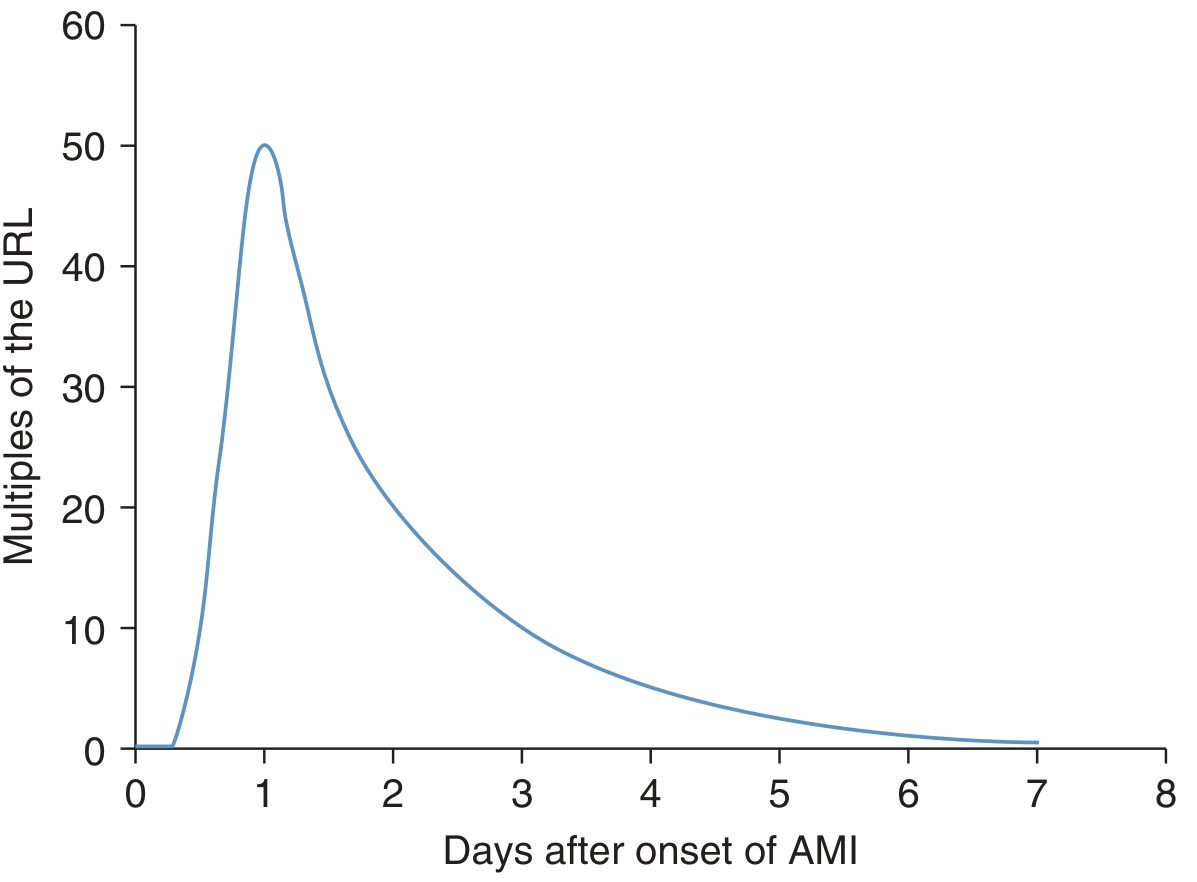
Tintinalli's Emergency Medicine, Figure 48-1 - Troponin elevation peaks around day 1 at ~50x the upper reference limit and slowly returns toward baseline over 7 days.
Current Hierarchy in Clinical Practice
For ACUTE MI DIAGNOSIS:
hs-Troponin (first choice)
→ CK-MB (if troponin unavailable)
→ [Myoglobin, LDH, AST: obsolete]
For HEART FAILURE:
BNP / NT-proBNP (first choice)
→ ST2 / Galectin-3 (prognostic adjuncts)
For CARDIOVASCULAR RISK (asymptomatic):
hs-CRP → Lp-PLA2 → Lipoprotein(a)
For PLAQUE INSTABILITY (pre-necrosis):
IMA → Myeloperoxidase → Copeptin (adjunctive)
[None currently recommended for routine ED use]
Sources: Tintinalli's Emergency Medicine | Fuster and Hurst's The Heart 15th Ed. | Rosen's Emergency Medicine | MDPI Int. J. Mol. Sci. 2025 (PMC11989402)
nornal value of these markers
Finding Sources
Finding Sources
Searching the Web
normal reference values cardiac biomarkers troponin CK-MB BNP myoglobin LDH laboratory 2024
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading Web Page
https://alliedhealth.lsuhsc.edu/cl/docs/Fall2025CardiacMarke…
Finding Sources
Searching the Web
normal reference range BNP NT-proBNP CRP myoglobin AST LDH cardiac markers laboratory values
I now have enough data from textbooks and authoritative sources. Here is the complete normal values reference:
Normal Reference Values of All Cardiac Markers
Important note: Reference ranges vary by laboratory, assay manufacturer, patient sex, age, and renal function. Always interpret results in relation to your specific laboratory's reference range. The values below represent widely accepted standard ranges.
MARKERS OF MYOCARDIAL NECROSIS
1. Cardiac Troponin I (cTnI)
| Parameter | Value |
|---|---|
| Normal (conventional assay) | < 0.04 ng/mL (< 0.04 µg/L) |
| Borderline (unstable angina) | 0.04 - 0.1 ng/mL |
| Positive for MI | > 0.1 ng/mL |
| Key threshold | > 99th percentile of upper reference limit (URL) |
2. Cardiac Troponin T (cTnT)
| Parameter | Value |
|---|---|
| Normal (conventional assay) | < 0.01 ng/mL (< 0.01 µg/L) |
| Elevated | > 0.1 ng/mL (strongly suggests MI) |
| Key threshold | > 99th percentile of URL |
3. High-Sensitivity Troponin (hs-cTn)
| Parameter | Value |
|---|---|
| hs-cTnI normal | < 0.014 ng/mL (< 14 ng/L) |
| hs-cTnT normal | < 0.014 ng/mL (varies by manufacturer; Roche Elecsys: < 14 ng/L) |
| Rule-out threshold (0h) | < 5 ng/L (ESC 0h/1h algorithm) |
| Rule-in threshold | > 52 ng/L at 0h OR delta rise ≥ 5 ng/L at 1h |
The ESC/ACC criteria for MI: at least one value above the 99th percentile URL plus a rising and/or falling pattern on serial testing.
4. CK-MB (Creatine Kinase-MB)
| Parameter | Value |
|---|---|
| Normal (mass assay) | < 5 ng/mL (< 5 µg/L) |
| Normal (activity) | < 25 IU/L |
| CK-MB relative index | < 2.5% of total CK (if ≥ 2.5% = suggests cardiac origin) |
| CK-MB fraction | < 6% of total CK |
| Positive for MI | CK-MB ≥ 6% of total CK + absolute elevation |
5. Total CK (Creatine Kinase)
| Parameter | Value |
|---|---|
| Normal - Males | 55 - 170 IU/L |
| Normal - Females | 30 - 135 IU/L |
| Note | Varies with race, muscle mass; African-Americans may have higher baseline values |
6. Myoglobin
| Parameter | Value |
|---|---|
| Normal - Males | < 90 ng/mL (some labs: 28-72 ng/mL) |
| Normal - Females | < 75 ng/mL (some labs: 25-58 ng/mL) |
| General cutoff | < 85 - 90 ng/mL |
| Normally | Nearly absent from serum; detectable presence = muscle injury |
| Early MI positive | > 110 ng/mL (rises within 1-2 h of MI) |
7. LDH (Lactate Dehydrogenase) - Total
| Parameter | Value |
|---|---|
| Normal total LDH | 140 - 280 IU/L (some labs: 100 - 190 U/L) |
| Elevated in MI | > 480 IU/L (marked elevation) |
| LDH-1 (cardiac isoform) | 14 - 26% of total LDH |
| LDH-2 | 29 - 39% of total LDH |
| Flipped pattern (MI indicator) | LDH-1 > LDH-2 (ratio > 1.0) |
8. AST (Aspartate Aminotransferase)
| Parameter | Value |
|---|---|
| Normal - Males | 10 - 40 IU/L |
| Normal - Females | 10 - 30 IU/L |
| General range | 8 - 33 U/L |
| Note | Non-specific; primarily used today as a liver marker |
MARKERS OF HEMODYNAMIC STRESS / HEART FAILURE
9. BNP (B-type Natriuretic Peptide)
| BNP Level | Interpretation |
|---|---|
| < 100 pg/mL | Heart failure unlikely |
| 100 - 400 pg/mL | Indeterminate - consider other causes |
| > 400 pg/mL | Heart failure likely |
| > 1000 pg/mL | Severe heart failure / high mortality risk |
BNP < 100 pg/mL has a high negative predictive value for ruling out HF in an acutely dyspneic patient.
10. NT-proBNP (N-terminal Pro-BNP)
| Age Group | Rule-Out HF Threshold | Rule-In HF Threshold |
|---|---|---|
| < 50 years | < 300 pg/mL | > 450 pg/mL |
| 50 - 75 years | < 300 pg/mL | > 900 pg/mL |
| > 75 years | < 300 pg/mL | > 1800 pg/mL |
NT-proBNP has a longer half-life (~120 min) than BNP (~20 min), so levels are generally higher. Adjust for renal function (eGFR < 60 mL/min raises values significantly).
INFLAMMATORY / RISK MARKERS
11. hs-CRP (High-Sensitivity C-Reactive Protein)
| hs-CRP Level | Cardiovascular Risk |
|---|---|
| < 1.0 mg/L | Low risk |
| 1.0 - 3.0 mg/L | Intermediate risk |
| > 3.0 mg/L | High risk |
| > 10 mg/L | Likely acute infection/inflammation (not useful for cardiac risk) |
EMERGING MARKERS (Reference Ranges Where Available)
12. Myeloperoxidase (MPO)
| Parameter | Value |
|---|---|
| Normal serum MPO | < 470 pmol/L (varies by assay) |
| Elevated | Associated with increased short-term ACS risk even with negative troponin |
13. Copeptin
| Parameter | Value |
|---|---|
| Normal | < 10 pmol/L |
| Rule-out MI (copeptin + troponin at 0h) | Both normal = very high NPV for MI |
14. H-FABP (Heart-type Fatty Acid-Binding Protein)
| Parameter | Value |
|---|---|
| Normal | < 6 ng/mL (serum) |
| Elevated in MI | > 6 - 7 ng/mL (rises within 1-2 hours) |
15. IMA (Ischemia-Modified Albumin)
| Parameter | Value |
|---|---|
| Normal ABSU (albumin cobalt binding) | < 85 U/mL |
| Elevated (ischemia) | > 85 U/mL |
Quick Reference Summary Card
| Marker | Normal Value | Unit | Abnormal (MI) |
|---|---|---|---|
| cTnI | < 0.04 | ng/mL | > 0.04 |
| cTnT | < 0.01 | ng/mL | > 0.01 |
| hs-cTn | < 14 | ng/L | > 14 (use delta) |
| CK-MB (mass) | < 5 | ng/mL | > 5 |
| CK-MB (activity) | < 25 | IU/L | > 25 |
| CK-MB fraction | < 6% | % of total CK | ≥ 6% |
| Total CK (M) | 55-170 | IU/L | > 170 |
| Total CK (F) | 30-135 | IU/L | > 135 |
| Myoglobin (M) | < 90 | ng/mL | > 90 |
| Myoglobin (F) | < 75 | ng/mL | > 75 |
| LDH (total) | 140-280 | IU/L | > 280 |
| LDH-1/LDH-2 ratio | < 1.0 | ratio | > 1.0 = "flipped" = MI |
| AST (M) | 10-40 | IU/L | > 40 |
| AST (F) | 10-30 | IU/L | > 30 |
| BNP | < 100 | pg/mL | > 400 = HF likely |
| NT-proBNP | < 300 | pg/mL | Age-adjusted (see above) |
| hs-CRP | < 1.0 | mg/L | > 3.0 = high CV risk |
| Copeptin | < 10 | pmol/L | > 10 |
| H-FABP | < 6 | ng/mL | > 6-7 |
| IMA | < 85 | U/mL | > 85 |
Key Clinical Notes on Interpretation
- Troponin is the only biomarker for diagnosing MI per current ESC/ACC/AHA guidelines - a value above the 99th percentile URL with a rise-and-fall pattern is required.
- BNP/NT-proBNP are affected by age, sex, BMI, and renal function - always use age-adjusted cutoffs for NT-proBNP.
- CK-MB relative index ≥ 2.5% (CK-MB/total CK × 100) improves specificity for cardiac vs. skeletal muscle source.
- LDH flipped pattern (LDH-1 > LDH-2) is historically significant but no longer used in modern practice.
- Myoglobin is essentially absent from normal serum - any detectable level suggests muscle injury (cardiac or skeletal).
- In ESRD/dialysis patients: baseline troponin, BNP, and NT-proBNP are chronically elevated - a delta rise ≥ 20% is required to diagnose acute MI.
- hs-CRP > 10 mg/L more likely reflects active infection or inflammation and loses its value for cardiac risk stratification in that setting.
Sources: Harrison's Principles of Internal Medicine 22nd Ed. | Tintinalli's Emergency Medicine | Henry's Clinical Diagnosis and Management by Laboratory Methods | LSU School of Allied Health (2025) | Medscape Reference
This is a shared conversation. Sign in to Orris to start your own chat.