AKI
Reading File
Finding Sources
Searching PubMed
"acute kidney injury"[MeSH Terms] AND management
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
I now have excellent, comprehensive content from multiple authoritative textbooks. Let me compile the full AKI overview.
Acute Kidney Injury (AKI)
Definition
AKI (formerly "acute renal failure") is a rapid decline in kidney function resulting in the accumulation of nitrogenous waste products and disruption of fluid, electrolyte, and acid-base homeostasis. The current standard is the 2012 KDIGO definition, which unifies the earlier RIFLE and AKIN criteria:
AKI is diagnosed when any one of the following is met:
- Serum creatinine (sCr) rises by ≥0.3 mg/dL within 48 hours, OR
- sCr rises to ≥1.5× baseline within 7 days, OR
- Urine output (UO) <0.5 mL/kg/h for ≥6 hours
- Sabiston Textbook of Surgery, p. 449
- Washington Manual of Medical Therapeutics, p. 478
RIFLE / AKIN / KDIGO Staging
The three consensus criteria all use the same urine output thresholds but differ slightly in creatinine thresholds. The RIFLE and KDIGO/AKIN staging systems are shown below:
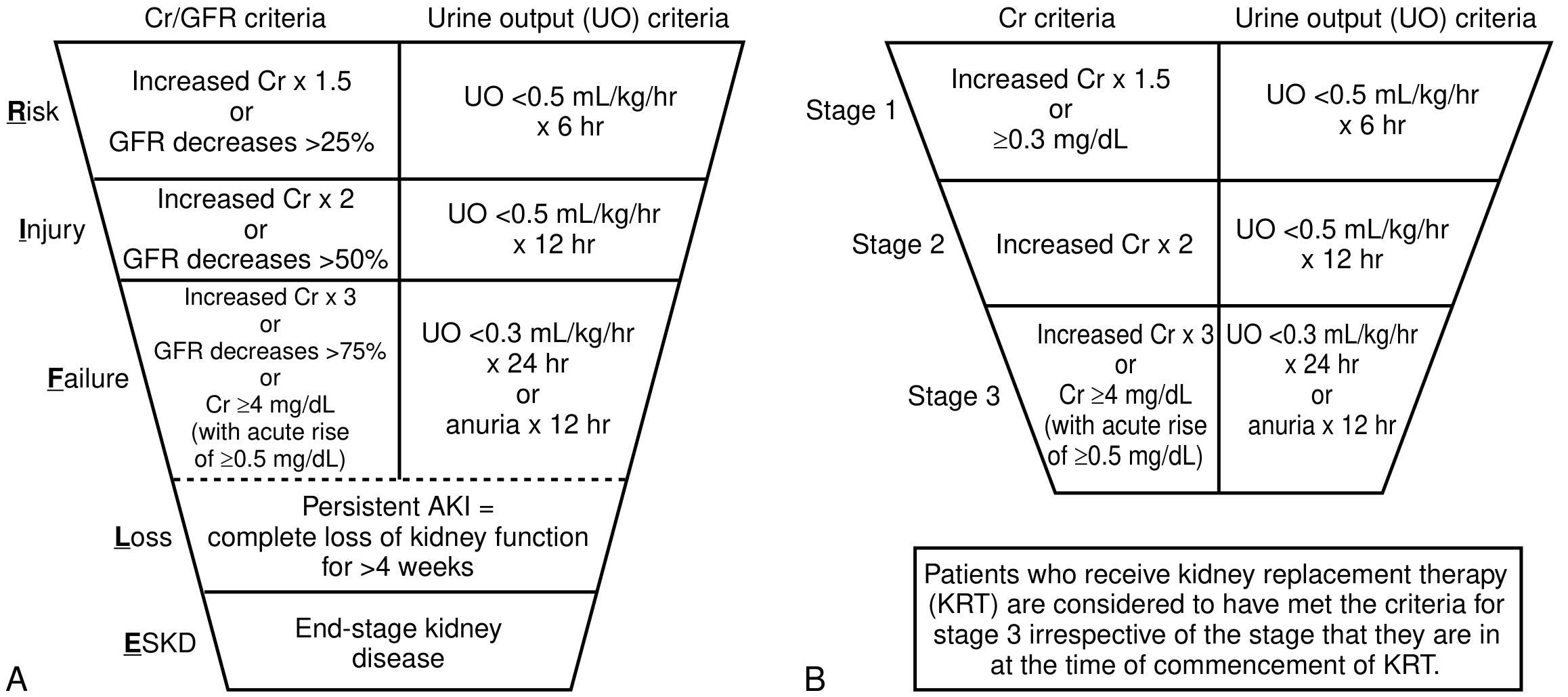
| Stage | Serum Creatinine | Urine Output |
|---|---|---|
| 1 | ≥1.5-1.9× baseline OR ≥0.3 mg/dL increase | <0.5 mL/kg/h for 6-12 h |
| 2 | 2.0-2.9× baseline | <0.5 mL/kg/h for ≥12 h |
| 3 | ≥3× baseline, OR sCr ≥4.0 mg/dL, OR initiation of RRT, OR eGFR <35 in <18 yrs | <0.3 mL/kg/h for ≥24 h OR anuria ≥12 h |
Higher stages = worse outcomes, greater mortality, and higher need for renal replacement therapy (RRT).
- Brenner & Rector's The Kidney, p. 1245
Etiology: Pre-renal / Intrinsic / Post-renal
| Category | Causes |
|---|---|
| Pre-renal | Hypovolemia (hemorrhage, dehydration, burns), hypotension/sepsis, low cardiac output (heart failure), loss of autoregulation (NSAIDs, RAAS blockers), hepatic cirrhosis (splanchnic vasodilation), abdominal compartment syndrome, renal artery stenosis |
| Intrinsic Renal | Tubular: Ischemic ATN, toxic ATN (contrast, aminoglycosides, amphotericin B, myoglobin in rhabdomyolysis, uric acid) - Vascular: Glomerulonephritis, thrombotic microangiopathy (HUS/TTP), atheroembolic disease - Interstitial: Acute interstitial nephritis (drug-induced, infectious), pyelonephritis |
| Post-renal | Urethral obstruction (BPH, stricture), bilateral ureteral obstruction (or unilateral if solitary kidney) |
- Washington Manual of Medical Therapeutics, p. 478
Prerenal azotemia implies preserved intrinsic kidney function in the setting of hypoperfusion. The BUN:Cr ratio is typically >20, urine sodium <20 mEq/L, and FENa <1%.
Contrast-induced AKI is one of the most common causes in surgical/hospital patients, especially those with pre-existing CKD.
Rhabdomyolysis causes AKI via three mechanisms: renal vasoconstriction, tubular cast formation from myoglobin precipitation, and free radical-mediated tubular cell injury.
Diagnostic Evaluation
Key lab tests distinguishing pre-renal vs. intrinsic vs. post-renal AKI:
| Parameter | Pre-renal | Intrinsic Renal | Post-renal |
|---|---|---|---|
| Urine osmolality | >500 mOsm/L | ~Plasma | Variable |
| Urinary sodium | <20 mEq/L | >50 mEq/L | >50 mEq/L |
| FENa | <1% | >3% | Variable |
| Urine:plasma creatinine | >40 | <20 | <20 |
| BUN:Cr ratio | >20 | <15 | Variable |
FENa limitations: FENa can be falsely LOW in intrinsic conditions such as contrast-induced nephropathy, rhabdomyolysis, and acute glomerulonephritis. In patients on diuretics, FEUrea <35% is a better indicator of pre-renal disease.
- National Kidney Foundation Primer on Kidney Diseases, p. 347
- Sabiston Textbook of Surgery, p. 450
Novel Biomarkers (emerging)
-
NGAL (neutrophil gelatinase-associated lipocalin): rises within 2-4 hours of injury
-
KIM-1 (kidney injury molecule-1): tubular injury marker
-
Cystatin C: sensitive for early GFR decline
-
TIMP-2 × IGFBP-7: urinary cell-cycle arrest markers, approved by FDA for predicting AKI risk
-
α1-microglobulin: proximal tubule dysfunction; urinary cystatin C and α1-microglobulin have AUC ~0.86 for predicting need for RRT in small studies
-
Brenner & Rector's The Kidney, p. 1163
Clinical Features
Early AKI may be asymptomatic, detected only by rising creatinine or falling urine output. As nitrogen waste accumulates and fluid overload develops:
- Symptoms: nausea, vomiting, fatigue, confusion (uremic encephalopathy), asterixis
- Signs: pericardial rub (uremic pericarditis), peripheral edema, pulmonary infiltrates (fluid overload), abnormal bleeding
- Oliguria: UO <400 mL/day; anuria: <100 mL/day (consider obstruction or bilateral cortical necrosis)
Management
Prevention (most effective strategy)
- Identify high-risk patients: age, CKD, diabetes, hypertension, obesity, high ASA class
- Optimize volume status and hemoglobin before surgery
- Maintain MAP >65 mmHg intraoperatively (>75-80 mmHg in hypertensives)
- Avoid/adjust nephrotoxic drugs (aminoglycosides, NSAIDs, contrast)
- Target intraoperative UO ≥0.5 mL/kg/h
General Treatment Once AKI Develops
There is no specific treatment to reverse AKI once established. Goals:
- Restore and maintain renal perfusion - correct hypovolemia, support MAP
- Avoid further injury - stop nephrotoxins, adjust drug doses
- Volume management - avoid both hypovolemia and volume overload; evaluate fluid responsiveness carefully
- Diuretics - use to manage fluid overload, not to prevent or treat AKI per se; do not delay RRT if indicated
Contrast-induced AKI prevention:
- IV volume expansion is the most beneficial intervention (isotonic saline or NaHCO3 solution)
- Start 6-12 hours pre-procedure, continue 4-12 hours post-procedure
- N-acetylcysteine and vitamin C remain controversial
Indications for Renal Replacement Therapy (RRT)
Classic indications ("AEIOU"):
- A - Acidosis (refractory metabolic acidosis)
- E - Electrolytes (refractory hyperkalemia)
- I - Intoxication (dialyzable toxins: lithium, methanol, salicylates)
- O - Overload (refractory pulmonary edema)
- U - Uremia (encephalopathy, pericarditis, bleeding)
The timing of RRT initiation remains debated and there are no universally agreed criteria; clinical judgment based on trajectory and complications guides the decision.
- Sabiston Textbook of Surgery, pp. 449-450
AKI vs. AKD vs. CKD
The KDIGO group proposed Acute Kidney Disease (AKD) for kidney dysfunction lasting >7 days but <3 months - a "gap" between AKI and CKD. CKD requires structural/functional changes persisting >3 months.
Outcomes & Prognosis
- Repeated AKI episodes can lead to permanent kidney function deterioration and progression to CKD
- Stage 3 AKI carries significantly higher mortality than Stage 1
- ICU patients: up to 80% meet AKI criteria when UO criterion is added to sCr; most UO-only cases are Stage 1 with high recovery rates
- AKI is an independent risk factor for long-term cardiovascular events and mortality
Sources: Brenner & Rector's The Kidney | National Kidney Foundation Primer on Kidney Diseases, 8e | Sabiston Textbook of Surgery | Washington Manual of Medical Therapeutics
How to do renal replacement therapy
Reading File
Finding Sources
Searching PubMed
"renal replacement therapy" AND "acute kidney injury"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive, detailed content from multiple authoritative textbooks. Let me compile the full RRT guide.
Renal Replacement Therapy (RRT) in AKI
RRT is the generic term for the multiple modalities of dialysis and hemofiltration used in kidney failure management. It corrects acid-base and electrolyte disturbances, alleviates volume overload, and removes uremic solutes - but it does not hasten renal recovery, and can potentially delay it if applied inappropriately.
Indications for RRT
Absolute Indications ("AEIOU")
| Indication | Detail |
|---|---|
| Volume Overload | Pulmonary edema unresponsive to diuretic therapy |
| Electrolytes | Persistent hyperkalemia despite maximal medical management |
| Acidosis | Severe metabolic acidosis refractory to treatment |
| Uremia (Overt) | Encephalopathy, uremic pericarditis, uremic bleeding diathesis |
| Ingestions/Toxins | Dialyzable drugs: lithium, methanol, salicylates, ethylene glycol |
Relative Indications
- Progressive azotemia without overt uremic symptoms
- Persistent oliguria without response to optimization
- Impending acute respiratory failure from fluid overload
Timing debate: Three large RCTs (IDEAL-ICU, AKIKI, STARRT-AKI) showed no mortality benefit from early vs. delayed RRT in critically ill patients. A significant proportion of patients in the "delayed" arms (up to 29% in IDEAL-ICU) recovered and never required RRT at all. However, waiting until BUN >140 mg/dL was associated with increased mortality (HR 1.60) in AKIKI-2 - so overly delayed initiation is also harmful.
- Brenner & Rector's The Kidney, pp. 1245-1248
- Miller's Anesthesia, 10e, pp. 5702-5703
Principles of Solute Clearance
Two fundamental mechanisms drive solute removal:
- Diffusion: Concentration gradient across a semipermeable membrane - best for small molecules (<1 kDa). This is the basis of hemodialysis.
- Convection (ultrafiltration): Hydrostatic pressure-driven solvent drag - clears molecules up to 50 kDa, ideal for fluid removal and middle molecule clearance. This is the basis of hemofiltration.
- Hemodiafiltration combines both mechanisms.
RRT Modalities
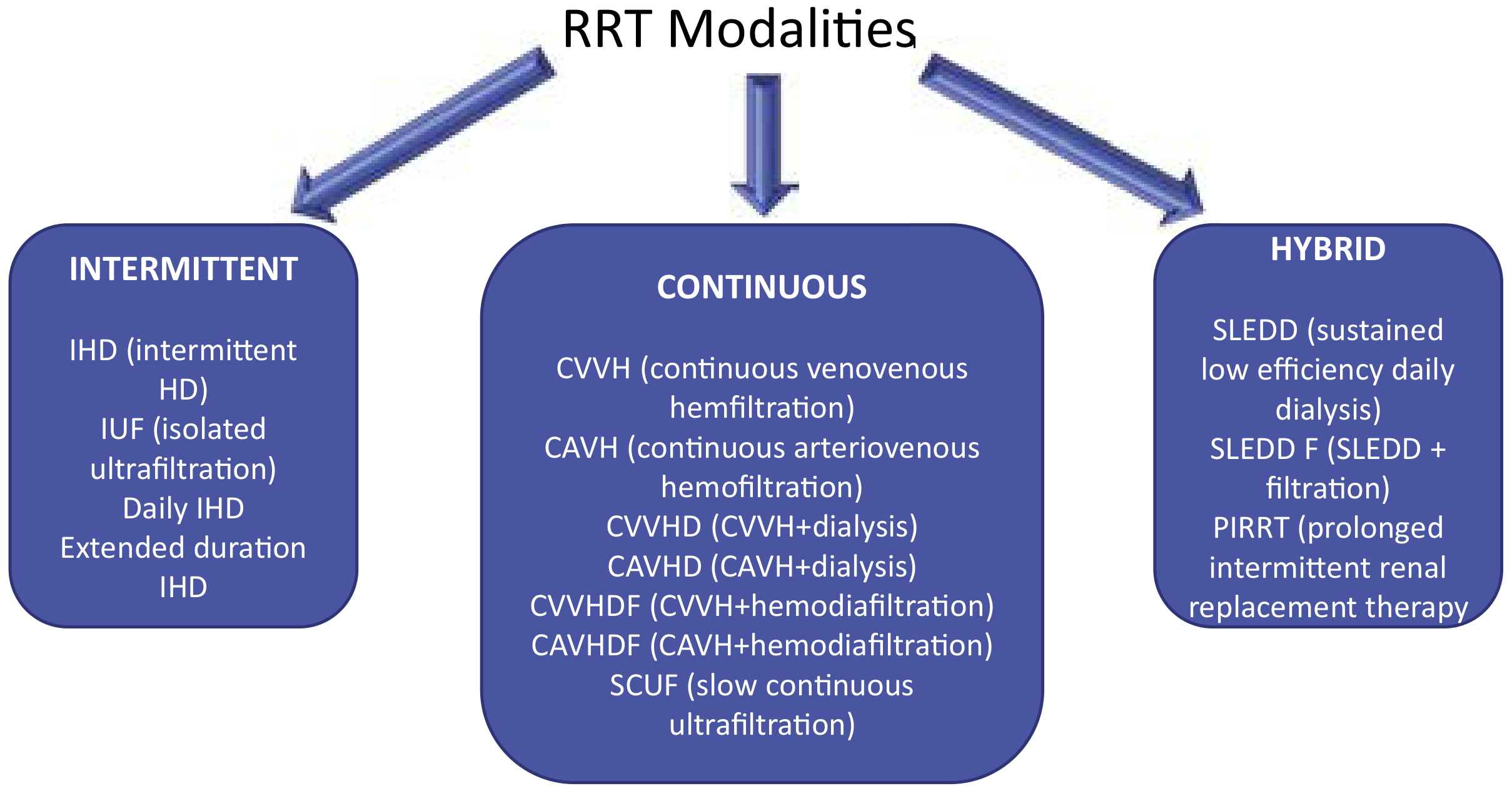
1. Intermittent Hemodialysis (IHD)
- Schedule: 3-6 sessions/week, 3-6 hours per session
- Mechanism: Diffusive clearance - blood and dialysate flow in opposite directions across a semipermeable membrane (countercurrent)
- Increasing clearance: Raise blood flow rate OR dialysate flow rate
- Best for: Hemodynamically stable patients
- Advantage: Time-efficient, allows scheduled patient mobility
- Disadvantage: Rapid fluid/solute shifts - risk of intradialytic hypotension (can prolong AKI and delay recovery)
2. Continuous RRT (CRRT)
Performed 24 hours/day. Preferred for hemodynamically unstable patients on vasopressors.
| CRRT Subtype | Mechanism | Access | Notes |
|---|---|---|---|
| CVVH (continuous venovenous hemofiltration) | Convection only | Venovenous | No dialysate; replacement fluid used |
| CVVHD (CVVH + dialysis) | Diffusion + convection | Venovenous | Dialysate added |
| CVVHDF (CVVH + hemodiafiltration) | Both | Venovenous | Highest clearance |
| SCUF (slow continuous ultrafiltration) | Convection, low rate | Venovenous | Primarily for fluid removal |
| CAVH/CAVHD | Arteriovenous approaches | Arteriovenous | Rare - bleeding risk from arterial access |
- Replacement fluid is infused either pre-filter (predilution - reduces clotting, reduces efficiency slightly) or post-filter (postdilution - higher efficiency but more clotting risk)
- Dose: Target effluent flow rate of 20-25 mL/kg/h (prescribed dose should be ~25 mL/kg/h to account for downtime). Intensive dosing at 35 mL/kg/h showed no mortality benefit over 20 mL/kg/h in the ATN trial.
3. Hybrid / Prolonged Intermittent RRT (PIRRT / SLED)
- Also called SLEDD (Sustained Low Efficiency Daily Dialysis) or SLEDD-F (+ filtration)
- Schedule: 6-18 hours/day, daily or every other day
- Mechanism: Slower flow rates than IHD, longer treatment time
- Advantage: More hemodynamically stable than IHD, less resource-intensive than CRRT; when done daily it approaches CRRT in clearance
- No standard machine - protocols vary by center
4. Peritoneal Dialysis (PD)
- Catheter placed intra-abdominally (laparoscopic or bedside)
- Dextrose-containing dialysate infused and drained via osmotic gradient
- Clears solutes and fluid without extracorporeal circuit
- Limitations in AKI: Cannot achieve adequate clearance in the hypermetabolism of critical illness; contraindicated after recent abdominal surgery
- Role: Primarily outpatient ESRD; important in low/middle-income settings where CRRT is unavailable
Vascular Access for Acute RRT
All extracorporeal modalities (IHD, CRRT, PIRRT) require a dedicated dual-lumen central venous catheter.
Preferred access sites (KDIGO order of preference):
- Right internal jugular vein - most direct path to superior vena cava, lowest dysfunction rate
- Femoral veins - easy bedside insertion; acceptable if BMI is normal (infection risk increases in high BMI patients)
- Left internal jugular vein - higher dysfunction rate due to tortuosity
- Subclavian vein - last resort only (risk of pneumothorax on mechanical ventilation, high rate of central vein stenosis - this can preclude future AV fistula creation in the ipsilateral arm)
Catheter specifications:
-
Internal jugular: 15-20 cm length; tip at atriocaval junction
-
Femoral: ≥20-25 cm length; tip must reach inferior vena cava
-
Ultrasound guidance for insertion - reduces mechanical complications
-
Noncuffed temporary catheters preferred in acute/critically ill
-
Replace with cuffed tunneled catheter if prolonged RRT anticipated (lower infection risk)
-
Brenner & Rector's The Kidney, p. 2820
Anticoagulation for the Extracorporeal Circuit
Anticoagulation is needed to prevent filter/circuit clotting.
| Method | Details | Preferred When |
|---|---|---|
| Regional citrate | Infused pre-filter; chelates ionized Ca²⁺ (required cofactor for coagulation cascade); reversed by Ca²⁺ infusion post-filter | First-line recommended by KDIGO; preferred for all patients (especially those with or at risk of bleeding) |
| Low-dose unfractionated heparin (UFH) | 100-500 units/h pre-filter; goal is circuit anticoagulation with minimal systemic effect | Widely available; small risk of increased systemic bleeding |
| Regional heparinization | Heparin pre-filter + protamine in return line | Largely replaced by low-dose heparin protocols |
| LMWH | Alternative to UFH; monitoring more difficult; half-life prolonged in AKI | Generally not preferred |
| No anticoagulation | For patients with active bleeding or high coagulopathy | Reduces circuit life significantly |
Citrate caution: Can accumulate causing metabolic alkalosis and hypocalcemia if hepatic metabolism is impaired (liver failure). Monitor ionized calcium closely.
Dialysis Dose & Adequacy
-
IHD: Measure Kt/V per session; target at minimum Kt/V of 1.2-1.4 per session (3×/week)
-
CRRT: Effluent volume (mL/kg/h) is the surrogate for dose. Target ≥20 mL/kg/h delivered (prescribe 25-30 mL/kg/h to account for downtime)
-
Higher dose does NOT improve outcomes: The ATN trial (1124 patients) showed no difference in 60-day mortality between 35 mL/kg/h vs. 20 mL/kg/h CRRT (53.6% vs. 51.5%, P = 0.47)
-
Membrane choice: Modern synthetic membranes are all relatively biocompatible; no single membrane has shown superiority in outcomes
-
Brenner & Rector's The Kidney, p. 1245-3200
Drug Dosing on RRT
Three key concerns when prescribing medications in AKI patients on RRT:
- Nephrotoxins - avoid/minimize (aminoglycosides, amphotericin B, contrast, NSAIDs, hydroxyethyl starches)
- Drug accumulation - renally-cleared drugs accumulate rapidly; dose-reduce or extend intervals
- Drug clearance by RRT - vital drugs (e.g., antibiotics, antivirals) may be removed by the filter; supplemental dosing required. CRRT clears drugs more continuously than IHD - consult pharmacokinetic references for each drug
Modality Selection Summary
| Clinical Situation | Preferred Modality |
|---|---|
| Hemodynamically stable | IHD or PIRRT |
| Hemodynamically unstable (vasopressors) | CRRT |
| Primarily fluid removal needed | SCUF or isolated ultrafiltration |
| Recent abdominal surgery | Avoid peritoneal dialysis |
| Resource-limited settings | Peritoneal dialysis |
| Drug/toxin removal (rapidly) | IHD (intermittent, efficient) |
Complications of RRT
| Complication | Modality | Details |
|---|---|---|
| Intradialytic hypotension | IHD (most) | Rapid fluid/solute shifts; can worsen and prolong AKI |
| Infection (catheter-related bacteremia) | All extracorporeal | Use strict aseptic technique; ultrasound-guided insertion |
| Bleeding | All (anticoagulation) | Risk from heparin; citrate preferred if bleeding risk high |
| Filter clotting | CRRT > IHD | Anticoagulate circuit; monitor post-filter ionized Ca²⁺ (citrate) |
| Peritonitis | Peritoneal dialysis | Major limiting complication |
| Citrate toxicity/accumulation | CRRT (citrate anticoag) | Monitor in liver failure; causes metabolic alkalosis + hypocalcemia |
| Drug underdosing | CRRT | Continuous drug clearance - supplement antibiotics/antivirals |
Sources: Brenner & Rector's The Kidney | Current Surgical Therapy 14e | Miller's Anesthesia, 10e | National Kidney Foundation Primer on Kidney Diseases, 8e



1000268412.jpg
+2 more
Peripheral pitting edema at both ankles and severe legs pains since 25 days , what is the diagnosis and how to manage
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have all the information needed for a comprehensive clinical analysis. Let me synthesize.
⚠️ Important Disclaimer
This is a clinical educational analysis based on the lab reports provided. It is not a substitute for a consultation with a treating physician who can examine the patient. Miss Chinthi Rala Vineela (23F) must be evaluated in person.
Clinical Analysis: 23-Year-Old Female with Bilateral Ankle Pitting Edema + Severe Leg Pain × 25 Days
Lab Results Summary
| Test | Result | Reference | Interpretation |
|---|---|---|---|
| ASO (Antistreptolysin O) | 130 IU/mL | 0-200 IU/mL | Upper-normal / borderline elevated |
| Urine Protein/Creatinine Ratio (UPCR) | 0.7 | Normal <0.2; Nephrosis >3.5 | Mildly elevated - significant proteinuria |
| Urine Spot Protein | 47.4 mg/dL | 15-20 mg/dL | Elevated |
| Urine Dipstick Protein | Nil | - | Discrepancy with biochemistry (see below) |
| Urine pH | 6.0 | Normal | Normal |
| Urine Specific Gravity | 1.015 | Normal | Normal |
| Urine Pus Cells | 2-4/hpf | 0-5/hpf | Within normal limits |
| No casts, no RBCs, no glucose | - | - | No nephritic sediment on routine |
Key finding: Dipstick protein is "Nil" but urine protein/creatinine ratio is 0.7 (significantly elevated). This discrepancy occurs because dipstick primarily detects albumin - if the proteinuria is tubular (non-albumin proteins like globulins, Tamm-Horsfall), dipstick can be falsely negative. The biochemical UPCR of 0.7 is the more reliable result.
Differential Diagnosis
Given: 23F, India, bilateral ankle pitting edema, severe leg pain × 25 days, ASO 130 IU/mL, UPCR 0.7, no hematuria, no casts
1. Poststreptococcal Reactive Arthritis (PSRA) - Most Likely
The clinical picture fits very well:
-
History of Group A Streptococcal (GAS) throat/skin infection 10-14 days prior (ask specifically)
-
ASO 130 IU/mL - evidence of recent streptococcal exposure (streptozyme panel including anti-DNAse B, ASKase, anti-NAD is positive in 80-95% of PSGN cases; ASO alone may be less sensitive)
-
Bilateral lower limb arthritis/arthralgia is the hallmark - non-migratory, severe, prolonged, resistant to salicylates (unlike ARF)
-
Edema can occur secondary to joint inflammation and dependent positioning
-
Proteinuria (UPCR 0.7) may represent a subclinical poststreptococcal glomerulonephritis component
-
Tintinalli's Emergency Medicine
2. Acute Rheumatic Fever (ARF) - Must Rule Out (High priority in India = high-risk population)
ARF is endemic in India. The 2015 revised Jones Criteria for high/moderate-risk populations (which includes India/Asia) include:
- Major criteria: Carditis (clinical or subclinical), arthritis (mono or polyarthritis OR polyarthralgia), chorea, subcutaneous nodules, erythema marginatum
- Minor criteria: Fever ≥38.5°C, elevated ESR ≥60 mm/h or CRP ≥3 mg/dL, prolonged PR interval
For diagnosis in a high-risk area: 2 major OR 1 major + 2 minor criteria + evidence of preceding GAS infection (elevated ASO/anti-DNAse B, positive throat culture, or rapid antigen)
This patient has leg pain + edema (possible arthritis) + borderline ASO. She is from a high-risk region. Echocardiogram is mandatory to rule out subclinical carditis.
- Red Book 2021, Jones Criteria Table 3.58
3. Poststreptococcal Glomerulonephritis (PSGN) with nephrotic features
- Mild proteinuria (UPCR 0.7) with edema is possible
- Classic PSGN presents with hematuria, casts, hypertension - none seen here
- Subclinical PSGN (no hematuria, low-level proteinuria, low C3) is 4-5× more common than clinical disease
- Check serum C3, C4, and creatinine urgently
4. Other causes to consider
| Condition | Clue |
|---|---|
| Deep Vein Thrombosis (DVT) | Usually unilateral; bilateral possible with IVC/iliac involvement or May-Thurner (L iliac compression) - do venous Doppler ultrasound |
| Lymphedema praecox | Onset at puberty/young adulthood in females; bilateral; non-pitting initially; no ASO elevation |
| Filariasis | Endemic in Andhra Pradesh/coastal India - bilateral lymphedema + pain; check peripheral blood smear for microfilariae |
| Nephrotic syndrome | UPCR 0.7 is below nephrotic range (>3.5); 24h urine protein <3.5g/day; but must exclude |
| Hypothyroidism | Myxedema - bilateral edema + myalgia; check TSH |
| Heart failure / hypoalbuminemia | Check serum albumin, LFT, echo |
Immediate Investigations Required
These tests are urgent and must be done now:
Blood Tests
| Test | Why |
|---|---|
| CBC with ESR | Inflammation, anemia of infection |
| CRP | Acute phase reactant for ARF diagnosis |
| Serum Creatinine + BUN | Renal function - is there kidney injury? |
| Serum Albumin | If low → nephrotic/hepatic cause of edema |
| Serum Complement C3, C4 | C3 low (C4 normal) strongly suggests PSGN |
| Anti-DNAse B | More sensitive than ASO for poststreptococcal disease (especially after skin infections) |
| Throat swab for GAS culture | Evidence of active streptococcal infection |
| LFT, TSH | Rule out hepatic and thyroid causes |
| Serum electrolytes | K, Na - baseline |
Imaging & Other
| Test | Why |
|---|---|
| ECG | PR interval prolongation (minor Jones criterion) |
| Echocardiogram (ECHO) | Critical - rule out subclinical carditis/rheumatic heart disease |
| Bilateral venous Doppler ultrasound | Rule out DVT |
| 24-hour urine protein | Better quantification of proteinuria |
| Peripheral blood smear (night) | Rule out filariasis microfilariae (endemic in AP) |
Management
Immediate General Measures
- Rest with limb elevation - reduces edema
- Avoid NSAIDs initially until ARF is ruled out (in PSRA, NSAIDs are treatment; in ARF, aspirin is used with specific dosing)
- Do NOT start empiric steroids without diagnosis
- Salt restriction and fluid monitoring
Once Diagnosis Confirmed
If Poststreptococcal Reactive Arthritis (PSRA):
- Eradication of streptococcal infection: Oral penicillin V or amoxicillin × 10 days (benzathine penicillin 1.2 MU IM single dose is equally effective)
- NSAIDs for arthritis pain: Naproxen or diclofenac (PSRA arthritis is often salicylate-resistant)
- Short-term antibiotic prophylaxis (monthly benzathine penicillin) for 1 year while monitoring for late carditis
- Monitor for development of ARF features over follow-up
If Acute Rheumatic Fever (ARF):
- Penicillin to eradicate GAS (as above)
- Aspirin 50-100 mg/kg/day (max 4-6 g/day) for arthritis/carditis
- If carditis with heart failure: Corticosteroids (prednisone 1-2 mg/kg/day × 2-4 weeks, then taper)
- Long-term secondary prophylaxis (benzathine penicillin 1.2 MU IM every 4 weeks for years, per risk stratification) - mandatory to prevent recurrence and rheumatic heart disease
- Echocardiographic follow-up
If PSGN (mild/subclinical):
- Supportive - no specific treatment; no immunosuppressants
- Control hypertension (if present) with antihypertensives
- Salt/fluid restriction if edematous
- Treat active streptococcal infection with antibiotics
- Monitor renal function - most children/young adults recover fully in 3-6 weeks
Clinical Bottom Line
This 23-year-old from India presents with:
- Bilateral ankle pitting edema + severe leg pain × 25 days
- Borderline ASO 130 IU/mL (evidence of recent streptococcal exposure)
- Mild proteinuria (UPCR 0.7) with no hematuria or casts
The most likely diagnosis is Poststreptococcal Reactive Arthritis, possibly with a subclinical poststreptococcal glomerulonephritis component.
Acute Rheumatic Fever must be urgently excluded given her age, region (India = high risk), and joint symptoms. An echocardiogram is non-negotiable - subclinical carditis can be present even without clinical signs and missing it leads to permanent valvular damage.
Filariasis is also in the differential given the endemic region (Andhra Pradesh coastal belt) - a nocturnal peripheral blood smear should be checked.
She needs urgent referral to a physician / rheumatologist / nephrologist for complete evaluation.
Sources: Harrison's Principles of Internal Medicine 22e | Red Book 2021 (AAP) | Tintinalli's Emergency Medicine | Symptom to Diagnosis, 4e | Brenner & Rector's The Kidney
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the information needed. Let me provide the updated, definitive clinical analysis with the new Echo and ECG data.
Updated Clinical Analysis - New Reports Received
Echo Report Summary (16 July 2026 - CH. VINEELA, 23F)
| Parameter | Result | Interpretation |
|---|---|---|
| EF | 64% | Normal (≥55%) |
| LV Diastolic function | Normal | Normal E/A ratio 1.5 - Grade 0 diastolic dysfunction |
| All 4 valves | Normal | No mitral/aortic/tricuspid/pulmonary regurgitation |
| No MR, No AR, No TR, No PR | Confirmed | No rheumatic valvular disease |
| IVS | Intact | No septal defect |
| Pericardium | Normal/No effusion | No pericarditis |
| RVSP | 25 mmHg | Normal (No pulmonary arterial hypertension) |
| No vegetation | Confirmed | No infective endocarditis |
| No Regional Wall Motion Abnormality | Confirmed | No ischemia/infarct |
Echo conclusion: Normal cardiac structure and function. No carditis. No rheumatic heart disease.
ECG Summary
| Parameter | Result | Interpretation |
|---|---|---|
| HR | 98 bpm | Upper normal sinus rate |
| PR interval | 140 ms | Normal (<200 ms = no first-degree heart block) |
| QRS | 76 ms | Normal |
| QTc | 416 ms | Normal |
| Rhythm | Sinus rhythm | Normal |
| Axis | -16° | Normal/borderline left - clinically insignificant |
| Machine diagnosis | Normal ECG | Confirmed |
ECG conclusion: Normal sinus rhythm. No PR prolongation. No arrhythmia. No conduction defect.
✅ Key Conclusions from New Data
1. Acute Rheumatic Fever is NOW DEFINITIVELY EXCLUDED
ARF requires evidence of carditis (clinical or subclinical) as a major criterion in most presentations. The echo shows:
- No mitral regurgitation (most sensitive marker of rheumatic carditis)
- No aortic regurgitation
- All valves morphologically normal
- No pericardial effusion
- PR interval 140 ms - normal (no Jones minor criterion met)
ARF is ruled out with high confidence.
2. Cardiac Cause of Edema Excluded
- EF 64%, normal LV function, no pulmonary hypertension (RVSP 25 mmHg normal)
- Congestive heart failure and cor pulmonale are excluded as causes of the bilateral leg edema
Revised Diagnosis
Most Likely: Poststreptococcal Reactive Arthritis (PSRA)
All findings now converge on this diagnosis:
| Evidence | Finding |
|---|---|
| Age/sex | 23-year-old female |
| Geography | Andhra Pradesh, India - endemic for GAS throat infections |
| Symptoms | Bilateral lower limb arthritis/arthralgia + edema × 25 days (prolonged > typical ARF) |
| ASO 130 IU/mL | Evidence of recent Group A Streptococcal infection |
| Echo NORMAL | No carditis - distinguishes from ARF |
| ECG NORMAL | No PR prolongation - another minor Jones criterion absent |
| Urine UPCR 0.7 | Mild proteinuria - possible subclinical PSGN component |
| No hematuria | Against overt nephritis |
| Urine no casts | Against active glomerulonephritis |
| Duration 25 days | PSRA arthritis is more prolonged and severe than ARF |
Key differentiating point: In India (high-risk ARF region), Braunwald's Heart Disease explicitly states: "In populations where RF is common, the distinction between PSRA and RF is unclear, and many would recommend that a diagnosis of PSRA not be made [as a separate entity]; it is appropriate to offer secondary prophylaxis with penicillin, as for episodes of acute RF."
This is critical - even though ARF carditis is excluded by echo, she still requires prophylaxis.
Co-diagnosis to Consider: Subclinical Poststreptococcal Glomerulonephritis (PSGN)
The mild proteinuria (UPCR 0.7, urine spot protein 47.4 mg/dL) with:
- No hematuria, no RBC casts (against active nephritic PSGN)
- No nephrotic-range proteinuria (UPCR <3.5)
- Normal dipstick (suggests non-albumin proteinuria - possibly tubular)
- Prior streptococcal infection
Subclinical PSGN is 4-5× more common than clinical PSGN. A low serum C3 with normal C4 would confirm this. Check serum C3, C4 urgently.
Management Plan (Definitive)
Step 1: Eradicate Residual Streptococcal Infection
Benzathine Penicillin G 1.2 MU IM - single dose (preferred in India for compliance)OR oral Amoxicillin 500 mg TID × 10 days / Penicillin V 500 mg BD × 10 daysIf penicillin allergic: Azithromycin 500 mg Day 1, then 250 mg × 4 days
Step 2: Treat Arthritis and Pain
Naproxen 500 mg BD (preferred NSAID for poststreptococcal arthritis - note PSRA is often salicylate-resistant and partially NSAID-resistant)Add Pantoprazole 40 mg OD for gastroprotection while on NSAIDsShort courses only - review in 2-4 weeks
Step 3: Secondary Prophylaxis with Penicillin
This is mandatory in India (high-ARF-risk region), even with normal echo:
Benzathine Penicillin G 1.2 MU IM every 4 weeksDuration: Minimum 1 year, with repeat echocardiogram at the end. If echo remains normal and no recurrence, prophylaxis may be stopped. If any valvular changes develop - continue for 5-10 years.
Braunwald's Heart Disease is explicit: patients from high-risk regions with PSRA should receive penicillin prophylaxis as they would for ARF.
Step 4: Monitor Renal Function (Subclinical PSGN)
| Test | Timing |
|---|---|
| Serum C3, C4 | Now - if C3 low with normal C4 → confirms PSGN |
| Serum creatinine + BUN | Now and repeat in 2-4 weeks |
| 24-hour urine protein | Better quantification |
| Urine microscopy | Repeat - check for RBC casts |
| Anti-DNAse B titre | More sensitive than ASO for PSGN (especially skin-origin GAS) |
For subclinical PSGN: Management is supportive only - no steroids, no immunosuppressants. Most cases resolve spontaneously in 3-6 weeks. Monitor BP carefully.
Step 5: Supportive Measures
- Leg elevation (above heart level) for 20-30 min 3× daily - reduces dependent edema
- Compression stockings (Class I, 15-20 mmHg) for ankle edema
- Moderate salt restriction (no added salt diet, <5g NaCl/day)
- Adequate hydration - do not restrict fluids unless hypertensive
- Rest during acute phase, then gradual activity resumption
Step 6: Rule Out Filariasis (Still Pending)
- Andhra Pradesh coastal belt is endemic for lymphatic filariasis
- Order nocturnal peripheral blood smear (taken between 10 PM - 2 AM for microfilariae)
- If positive → Diethylcarbamazine (DEC) 6 mg/kg/day × 12 days ± albendazole
Follow-Up Plan
| Timeline | Action |
|---|---|
| Immediately | Serum C3/C4, creatinine, albumin, anti-DNAse B, ESR, CRP, nocturnal blood smear |
| 2 weeks | Review response to NSAIDs/penicillin; reassess edema and pain |
| 1 month | BP check, urine protein, renal function |
| 3 months | Repeat urine protein, renal function |
| 12 months | Repeat echocardiogram to confirm no valvular changes; review need for ongoing prophylaxis |
Summary
| Before New Reports | After Echo + ECG | |
|---|---|---|
| ARF | Must exclude | Definitively excluded - normal echo, normal PR |
| Cardiac cause of edema | Must exclude | Excluded - EF 64%, no PAH |
| Likely diagnosis | PSRA / ARF / PSGN | PSRA + subclinical PSGN |
| Need prophylaxis? | Pending | Yes - mandatory in India |
This 23-year-old female has Poststreptococcal Reactive Arthritis with likely subclinical PSGN as the etiology of her bilateral ankle edema and leg pain. Cardiac involvement has been excluded. She needs penicillin eradication therapy, NSAIDs, secondary prophylaxis with monthly benzathine penicillin, and renal monitoring.
Sources: Braunwald's Heart Disease 12e | Harrison's Principles of Internal Medicine 22e | Red Book 2021 (AAP) | Tintinalli's Emergency Medicine
Does this patient really need renal biopsy
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have definitive, multi-source textbook guidance. Here is the complete answer:
Does This Patient Need a Renal Biopsy?
The Short Answer: No - not at this stage
Three major nephrology and emergency medicine textbooks are unanimous and explicit:
"The diagnosis of poststreptococcal glomerulonephritis rarely requires a kidney biopsy."
- Harrison's Principles of Internal Medicine 22e
"Renal biopsy is not indicated for diagnosis, unless atypical clinical features are present."
- Tintinalli's Emergency Medicine
"Kidney biopsy is not routinely indicated in PSGN but may be required for confirmation when clinical features are atypical."
- Comprehensive Clinical Nephrology, 7th Edition
Why This Patient Specifically Does NOT Need Biopsy Right Now
Apply the atypical features checklist to Miss Chinthi Rala Vineela, 23F:
| Indication for Biopsy | This Patient | Verdict |
|---|---|---|
| Nephrotic-range proteinuria (UPCR >3.5) | UPCR 0.7 - well below nephrotic range | ❌ Not present |
| Nephrotic syndrome (edema + heavy proteinuria + hypoalbuminemia) | Mild proteinuria only; serum albumin not yet checked | ❌ Not confirmed |
| Worsening kidney dysfunction / AKI | Serum creatinine not reported - needs checking | ⚠️ Check first |
| C3 depressed for >1 month (suggests C3 glomerulopathy transformation) | C3 not yet checked; symptom duration is 25 days = <1 month | ❌ Too early to invoke this |
| Hematuria / RBC casts | Urine shows no blood, no casts | ❌ Not present |
| Hypertension | Not reported | ❌ Not confirmed |
| No streptococcal evidence (ASO, anti-DNAse B negative) | ASO 130 IU/mL positive | ❌ Evidence present |
| No clinical improvement after 4-6 weeks | Too early - only 25 days | ⚠️ Reassess at 6 weeks |
None of the established indications for biopsy are currently met.
When Would Biopsy Become Necessary? (Watchful Waiting Triggers)
If any of these develop, revisit the biopsy decision:
| Trigger | Timing | What It Suggests |
|---|---|---|
| C3 remains low after 8-12 weeks | At 8-week review | Transformation to C3 glomerulopathy (not PSGN) |
| Proteinuria does not resolve in 6 months | At 6-month review | Underlying IgA nephropathy, FSGS, or membranous GN |
| Nephrotic-range proteinuria develops (UPCR >3.5) | Any time | Rules out PSGN; consider lupus, minimal change, FSGS |
| Rapid worsening of kidney function / oliguria | Any time | Crescentic GN / RPGN - emergency biopsy |
| Hematuria + hypertension persist beyond 3 months | At 3-month review | Atypical course - another GN must be excluded |
| Young woman, no streptococcal evidence | If serology comes back negative | Could be lupus nephritis - ANCA, ANA, anti-dsDNA needed |
What She Needs Instead of Biopsy
PSGN is a clinical and serological diagnosis. The following tests will confirm it without any invasive procedure:
| Test | Expected in PSGN | Clinical Use |
|---|---|---|
| Serum C3 | Low | Single most useful test; low C3 + streptococcal evidence = PSGN confirmed |
| Serum C4 | Normal | C3↓ + C4 normal = alternate pathway activation (PSGN pattern) |
| Anti-DNAse B | Elevated | More sensitive than ASO, especially for skin-source GAS |
| Streptozyme test | Positive 80-95% | Combination of ASO + anti-DNAse + others |
| Serum creatinine | Elevated or normal | Assess kidney function |
| Serum albumin | Normal or mildly low | Excludes nephrotic syndrome |
If C3 is low + ASO/anti-DNAse positive + mild proteinuria + streptococcal exposure history = PSGN confirmed. No biopsy needed.
Important Note Specific to This Patient's Age
Comprehensive Clinical Nephrology flags "adult age" as a relative indication for biopsy in PSGN - because in adults (vs. children), atypical presentations and co-existing renal diseases are more common. At 23 years, she sits at the younger end of adulthood. This means:
- She does not need biopsy right now given her mild, non-nephrotic presentation
- But she needs closer follow-up than a child would
- If her proteinuria does not fully resolve by 3-6 months, biopsy should be reconsidered to exclude an underlying GN (IgA nephropathy or lupus nephritis are important differentials in a young Indian woman)
Summary
| Question | Answer |
|---|---|
| Does she need biopsy now? | No - classic/subclinical PSGN presentation, no atypical features currently |
| What confirms PSGN? | Low C3 + normal C4 + elevated ASO/anti-DNAse B - no biopsy needed |
| What to do instead? | Serum C3/C4, creatinine, albumin, anti-DNAse B |
| When to reconsider biopsy? | If C3 stays low >8 weeks, proteinuria persists >6 months, worsening renal function, or nephrotic syndrome develops |
Sources: Harrison's Principles of Internal Medicine 22e | Tintinalli's Emergency Medicine | Comprehensive Clinical Nephrology 7e
This is a shared conversation. Sign in to Orris to start your own chat.