pleural effusion examination findings in medicine case
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Searching Images
pleural effusion physical examination chest findings
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of pleural effusion examination findings from authoritative medical textbooks:
Pleural Effusion — Examination Findings
Symptoms (History)
- Dyspnea — typically does not develop until fluid volume reaches ≥500 mL
- Pleuritic chest pain — sharp, worse with deep breathing; may be referred to the ipsilateral shoulder (indicates pleural inflammation)
- Small effusions are often clinically silent
- Symptoms of the underlying cause (fever/chills in empyema; signs of anaemia in haemothorax)
Physical Examination — The Four Pillars
1. Inspection
| Finding | Detail |
|---|---|
| Reduced chest wall expansion | Lag or decreased excursion on the affected side on inspiration |
| Bulging intercostal spaces | With large effusions |
| Tracheal/mediastinal shift | Shifted away from a large effusion (contrast with collapse, where shift is toward) |
| Cyanosis / accessory muscle use | With very large or tension effusions |
The examination finding that best correlates with presence of pleural effusion is asymmetric chest wall expansion — Washington Manual of Medical Therapeutics
2. Palpation
| Finding | Detail |
|---|---|
| Decreased tactile (vocal) fremitus | Key distinguishing feature from consolidation, where fremitus is increased |
| Reduced chest expansion | Confirmed by hand placement with thumbs at midline |
| Trachea shifted away | In massive effusions |
| Apex beat displaced | Shifted contralaterally in large effusions |
3. Percussion
| Finding | Detail |
|---|---|
| Stony dullness | The hallmark of pleural fluid — dull/flat note, maximal at the base |
| Shifting dullness | Dullness shifts with patient repositioning |
| Diaphragm immobility | If the diaphragm does not move on percussion, an effusion is likely |
| Fluid level | Small/moderate effusions: dullness at lung base with resonance above; large effusions may opacify the entire hemithorax |
4. Auscultation
| Finding | Detail |
|---|---|
| Diminished/absent breath sounds | Over the effusion — the principal auscultatory sign |
| Egophony ("E-to-A" change) | Heard at the superior border of the effusion, where the underlying compressed (atelectatic) lung transmits sound |
| Bronchial breath sounds | At the upper edge of the effusion (compressed lung) |
| Pleural friction rub | If there is pleuritis without or before significant fluid accumulation; disappears as fluid increases |
| Decreased vocal resonance | Whispered pectoriloquy absent over effusion |
Auscultatory percussion — percussing the chest while listening with the stethoscope — may be more sensitive and specific than conventional percussion alone. — Rosen's Emergency Medicine
Summary Comparison Table (Key Differentiator)
| Feature | Pleural Effusion | Consolidation (Pneumonia) | Pneumothorax |
|---|---|---|---|
| Inspection | Lag on affected side | Possible lag/splinting | Lag on affected side |
| Tactile fremitus | Decreased | Increased | Absent |
| Percussion | Stony dull | Dull | Hyper-resonant/tympanitic |
| Breath sounds | Absent/diminished | Bronchial | Absent |
| Egophony | At superior border only | Present (diffuse over lobe) | Absent |
| Trachea shift | Away from lesion | None or toward | Away (tension) |
Modified from: Textbook of Family Medicine 9e; Murray & Nadel's Textbook of Respiratory Medicine
Special Findings
- Shifting dullness on percussion (≥1.5 L): indicates free-flowing fluid
- Stony dull note: more pronounced than simple consolidation; distinguishes fluid from solid lung
- Friction rub: early pleuritis before fluid accumulates; may reappear as fluid resolves
- In massive effusions (>1.5–2 L): hemodynamic compromise, severe dyspnea, mediastinal shift — most commonly due to malignancy
Radiological Correlation
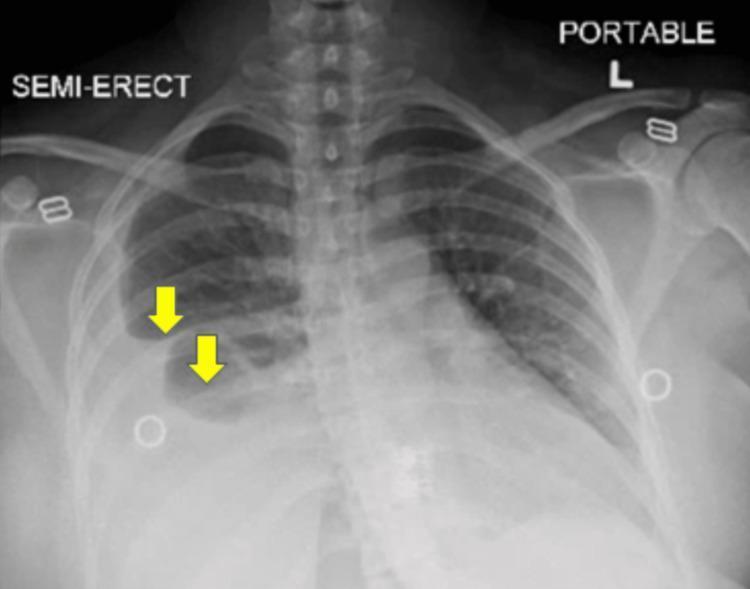
AP chest X-ray showing a large right-sided pleural effusion (yellow arrows) with leftward mediastinal shift — consistent with massive pleural effusion
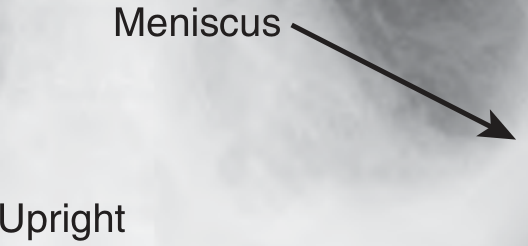
Upright PA chest X-ray showing the classic meniscus sign — curvilinear upper margin concave to the lung, higher laterally than medially — Roberts & Hedges' Clinical Procedures
- CXR: ≥200 mL needed to see blunting of costophrenic angle on upright PA; ≥150 mL on lateral; layering haziness on supine
- Ultrasound: can detect as little as 5 mL; preferred for bedside diagnosis and guidance for thoracentesis
- CT chest: clarifies loculation, underlying lung disease, pleural nodules
Key Clinical Pearl
Decreased breath sounds + dullness to percussion = pleural effusion OR consolidation. The differentiating sign is tactile fremitus: decreased in effusion, increased in consolidation. Egophony is present throughout a consolidated lobe but only at the upper border of an effusion. — Textbook of Family Medicine 9e; Goldman-Cecil Medicine
Sources: Washington Manual of Medical Therapeutics | Rosen's Emergency Medicine | Tintinalli's Emergency Medicine | Textbook of Family Medicine 9e | Murray & Nadel's Textbook of Respiratory Medicine | Goldman-Cecil Medicine | S. Das Manual on Clinical Surgery 13e | Roberts & Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.