Thyroid storm
Reading File
Finding Sources
Finding Sources
Searching PubMed
"thyroid storm" management
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, high-quality textbook content and excellent images. Let me compile the full answer.
Thyroid Storm
Thyroid storm (thyrotoxic crisis) is a rare, life-threatening endocrine emergency representing the extreme end of the thyrotoxicosis spectrum. Untreated mortality approaches 100%; with prompt recognition and treatment, it falls to 10-30%.
Definition & Pathophysiology
Thyroid storm is not simply severe hyperthyroidism - it is a state of multiorgan dysfunction triggered by an acute catecholamine-thyroid hormone synergy. The exact mechanism is incompletely understood, but involves:
- Sudden elevation of free thyroid hormones (T3/T4 released from binding proteins during stress)
- Increased adrenergic receptor sensitivity to circulating catecholamines
- Peripheral T4 → T3 conversion surge, amplifying active hormone levels
- T3 enters cell nuclei, binds thyroid hormone-responsive elements, drives widespread gene transcription and metabolic acceleration
The total thyroid hormone level may not be dramatically elevated over uncomplicated hyperthyroidism - the shift is in free hormone levels and receptor hyperresponsiveness.
Precipitating Factors
| Category | Examples |
|---|---|
| Systemic insult | Infection, trauma, general surgery |
| Cardiovascular | Myocardial infarction, pulmonary embolism, stroke |
| Endocrine | Diabetic ketoacidosis, hyperosmolar coma |
| Drug/hormone related | Withdrawal of antithyroid drugs, iodine load, radioactive iodine therapy, exogenous thyroid hormone ingestion |
| Obstetric | Labor and delivery, eclampsia, preeclampsia |
| Iatrogenic | Thyroid gland palpation (vigorous) |
| Unknown | Up to 25% of cases have no identifiable trigger |
The underlying cause is most often Graves disease, though toxic multinodular goiter, destructive thyroiditis, and hCG-secreting hydatidiform mole can also precipitate storm.
Clinical Features
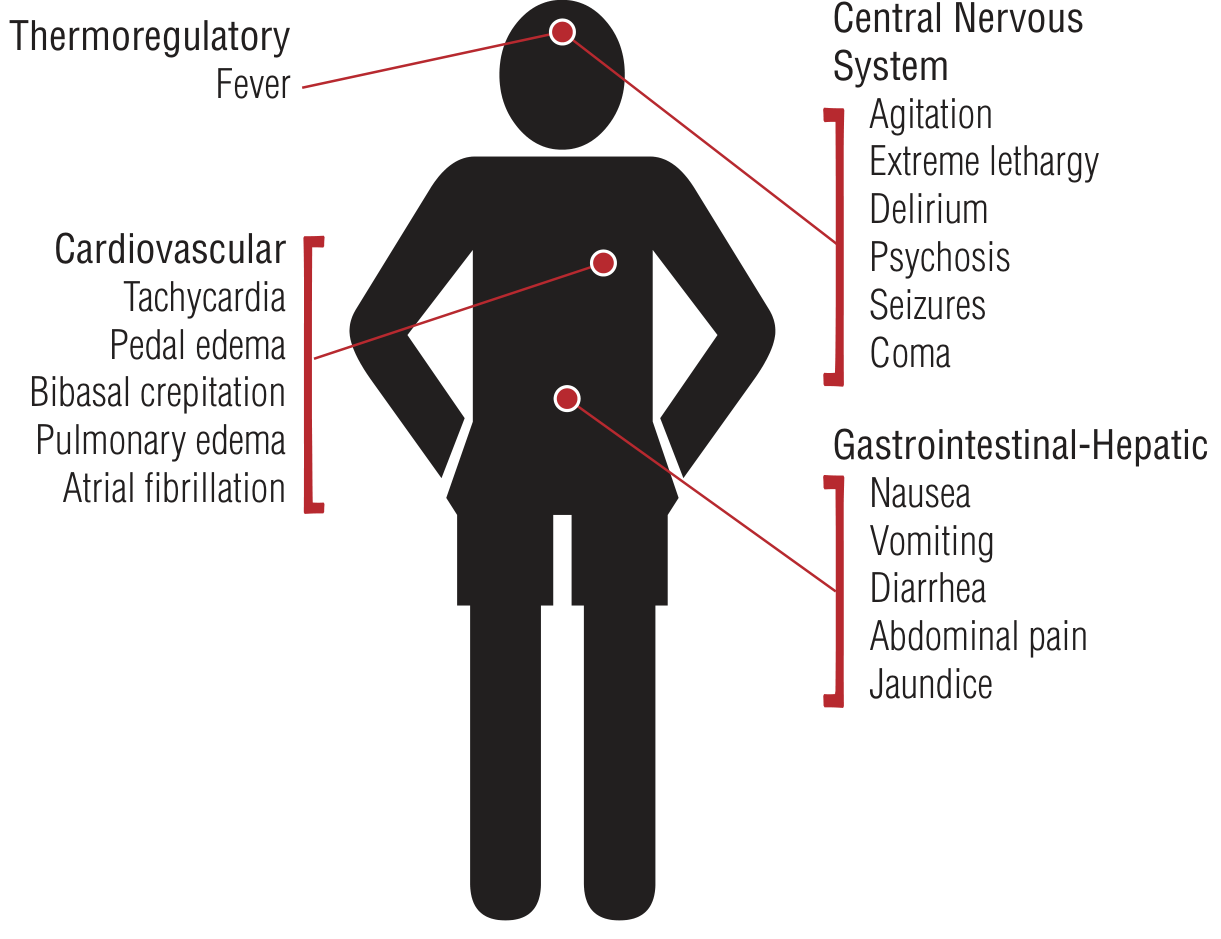
Figure: Clinical features of thyroid storm (Tintinalli's Emergency Medicine)
The cardinal triad is fever + extreme tachycardia + altered mental status, but the full picture spans four organ systems:
Thermoregulatory
- Hyperpyrexia: 104-106°F (40-41°C), often dramatic
Cardiovascular
- Tachycardia (often out of proportion to fever), atrial fibrillation
- Congestive heart failure, pulmonary edema, pedal edema
- Bibasal crepitations, hypotension (from volume depletion or cardiogenic shock)
Central Nervous System
- Agitation, anxiety, tremor
- Delirium, psychosis
- Seizures, extreme lethargy, coma
Gastrointestinal-Hepatic
- Nausea, vomiting, diarrhea
- Abdominal pain
- Hepatic failure with jaundice (poor prognostic sign)
Classic thyroid exam findings (goiter, ophthalmopathy, lid lag, stare) support the diagnosis but may be absent.
Diagnosis
Thyroid storm is a clinical diagnosis. Do not wait for labs to start treatment.
Labs to order: Free T4, Free T3, TSH (will show suppressed/undetectable TSH + elevated free hormones), CBC, metabolic panel, blood cultures, ECG.
Burch-Wartofsky Point Scale (BWPS)
| Parameter | Points |
|---|---|
| Fever | |
| 99-99.9°F | 5 |
| 100-100.9°F | 10 |
| 101-101.9°F | 15 |
| 102-102.9°F | 20 |
| 103-103.9°F | 25 |
| ≥104°F | 30 |
| Heart rate (bpm) | |
| 90-109 | 5 |
| 110-119 | 10 |
| 120-129 | 15 |
| 130-139 | 20 |
| ≥140 | 25 |
| Mental status | |
| Normal | 0 |
| Mild agitation | 10 |
| Delirium/psychosis/extreme lethargy | 20 |
| Seizure or coma | 30 |
| GI-hepatic dysfunction | |
| Absent | 0 |
| Moderate (diarrhea, nausea/vomiting) | 10 |
| Severe (jaundice) | 20 |
| Heart failure | |
| Absent | 0 |
| Mild (pedal edema) | 5 |
| Moderate (bibasal crepitations) | 10 |
| Severe (pulmonary edema) | 15 |
| Atrial fibrillation | 10 |
| Precipitating event identified | 10 |
- Score ≥45: thyroid storm (or impending storm) - treat aggressively
- Score 25-44: impending storm - treat and monitor closely
- Score <25: unlikely thyroid storm
Differential Diagnosis
| Condition | Distinguishing features |
|---|---|
| Heatstroke | No goiter, no thyroid history |
| Neuroleptic malignant syndrome | Recent antipsychotic use, rigidity |
| Serotonin syndrome | Serotonergic drug exposure, hyperreflexia, clonus |
| Anticholinergic crisis | Dry skin, urinary retention, mydriasis |
| Sympathomimetic toxidrome | Drug history, no goiter |
| Sepsis | Cultures positive, may coexist |
| Meningitis | Meningeal signs, CSF abnormalities |
Management
Treatment should be initiated simultaneously across all five pillars. Admit to ICU.
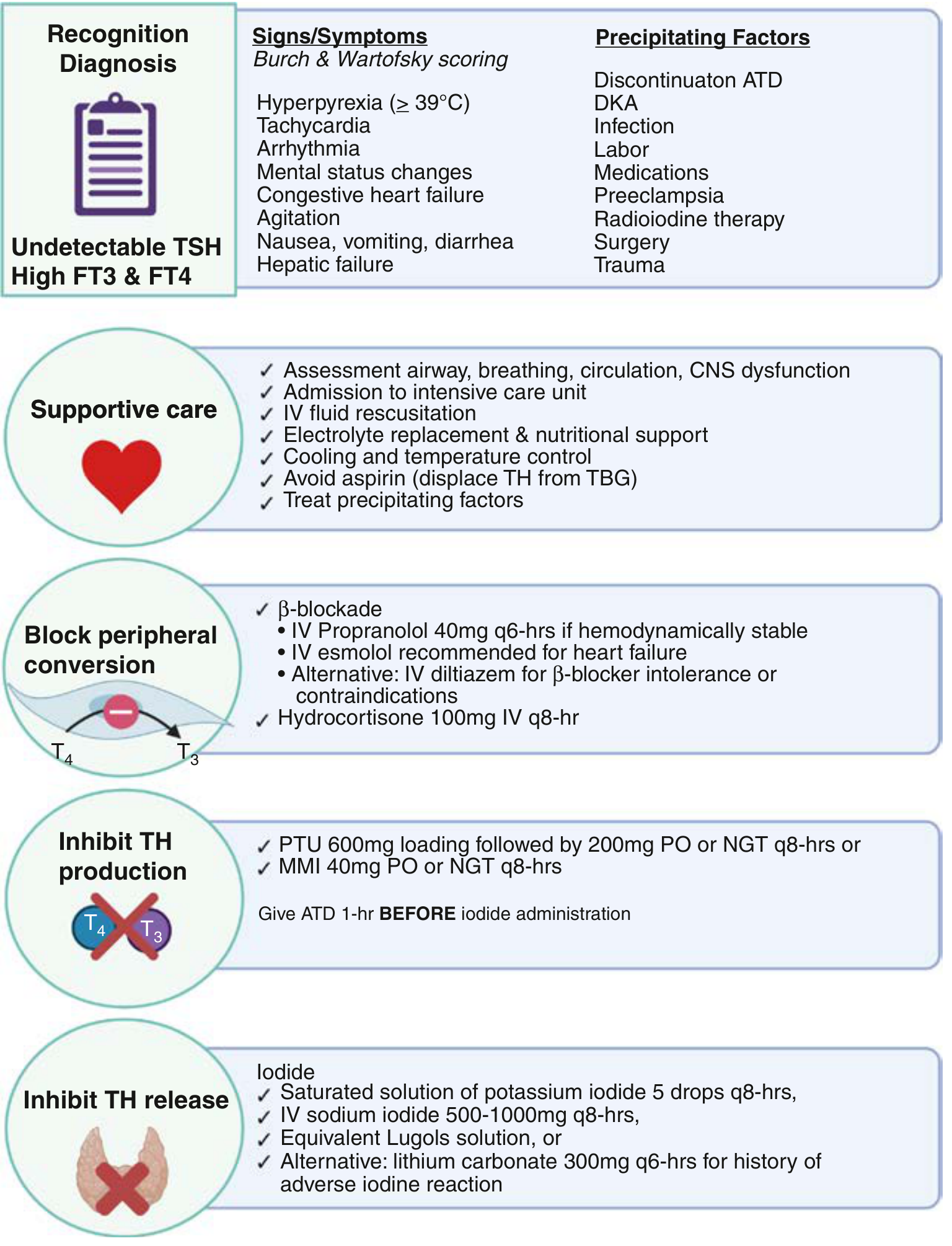
Figure: Thyroid storm recognition, diagnosis, and management algorithm (Creasy & Resnik's Maternal-Fetal Medicine)
Step 1 - Block peripheral T4 → T3 conversion (immediate)
Beta-blockers (reduce adrenergic symptoms AND slightly block T4→T3 conversion):
- Propranolol 60-80 mg PO q4h OR 0.5-1.0 mg IV slow push test dose, then 1-2 mg IV q15 min until controlled, then 1-2 mg IV q3h
- Esmolol 50-100 mcg/kg/min IV infusion (preferred in heart failure - titratable)
- Metoprolol 25-50 mg PO q6h (alternative)
- If beta-blockers strictly contraindicated: reserpine 2.5-5 mg IM q4h OR diltiazem IV
Corticosteroids (block T4→T3 + treat relative adrenal insufficiency):
- Hydrocortisone 300 mg IV loading dose, then 100 mg IV q8h
- OR Dexamethasone 2-4 mg IV q6h
Step 2 - Inhibit thyroid hormone synthesis (give 1 hour BEFORE iodide)
Antithyroid drugs (ATDs):
- PTU (propylthiouracil) 500-1000 mg loading dose PO/NG, then 250 mg q4h - preferred in storm because it also blocks peripheral T4→T3 conversion
- OR Methimazole 60-80 mg/day in divided doses
- Can be given PO, nasogastric, or PR (rectal enema prepared by pharmacy) - same dosing for all routes
Critical rule: ATD must be given at least 1 hour before iodide - otherwise iodide provides substrate for synthesis of even more thyroid hormone.
Step 3 - Inhibit thyroid hormone release (give AFTER ATD)
Iodide solutions (Wolff-Chaikoff effect - block organification and hormone release):
- SSKI (saturated solution of KI, 50 mg iodide/drop): 1-2 drops PO/PR three times daily
- OR Lugol's solution (8 mg iodide/drop): 5-7 drops PO/PR three times daily
- OR Sodium iodide IV per endocrinology guidance
- If iodine allergy: Lithium carbonate 300 mg PO/NG q6h (blocks hormone release)
- Cholestyramine 1-4 g PO twice daily - blocks enterohepatic recirculation of thyroid hormone (useful in refractory cases)
Step 4 - Supportive care
- IV fluids: D5/0.9NS for volume resuscitation and glycogen replacement (thyroid hormone depletes glycogen)
- Fever control: Acetaminophen (NOT aspirin - aspirin displaces T4 from thyroid-binding globulin, worsening free hormone levels), cooling blankets, ice packs, fans, ice lavage
- Electrolyte replacement and nutritional support
- Lorazepam or diazepam for agitation/seizures and to reduce central sympathetic outflow
- Supplemental oxygen, cardiac monitoring
Step 5 - Identify and treat the precipitating event
- Empirical broad-spectrum antibiotics if infection cannot be ruled out
- Treat concurrent DKA, pulmonary embolism, MI as indicated
Refractory/Escalation Options
If no clinical improvement after 24-48 hours of aggressive management:
- Plasma exchange (plasmapheresis) - directly removes circulating T3/T4 and TSH-receptor antibodies (TRAbs)
- Dialysis - transient reduction of thyroid hormone levels
- Near-total thyroidectomy - only if ATDs are contraindicated (e.g., agranulocytosis), requires stabilization first
Special Population: Pregnancy
- PTU is preferred over methimazole in the first trimester (methimazole has teratogenic risk - aplasia cutis, choanal atresia)
- Avoid aspirin - displaces thyroid hormones from TBG
- Short-acting beta-blockers preferred (e.g., esmolol, labetalol)
- Avoid delivery during active thyroid storm - fetal status typically improves as maternal status stabilizes
- Hydrocortisone is preferred over dexamethasone in pregnancy (largely inactivated by placental 11β-HSD to cortisone, reducing fetal exposure)
Causes of Death
- Multiorgan dysfunction syndrome
- Congestive heart failure / high-output cardiac failure
- Cardiac arrhythmias
- Respiratory failure
- Disseminated intravascular coagulation (DIC)
- Hypoxic brain injury
- Sepsis
- Hepatic failure (jaundice = poor prognosis)
Key Pearls
- Clinical diagnosis - never delay treatment waiting for thyroid function tests
- ATD before iodide - giving iodide first causes a surge in hormone synthesis
- Avoid aspirin for fever - use acetaminophen only
- PTU preferred over MMI in storm - dual benefit of synthesis inhibition AND peripheral conversion block
- Burch-Wartofsky ≥45 = treat as storm regardless of lab values
- Mortality is 10-30% even with treatment; unrecognized storm carries up to 75% mortality
- Esmolol preferred over propranolol in heart failure (short-acting, easily titrated, reversed)
Sources: Rosen's Emergency Medicine (9e), Tintinalli's Emergency Medicine (9e), Creasy & Resnik's Maternal-Fetal Medicine, Braunwald's Heart Disease, Miller's Anesthesia (10e)
This is a shared conversation. Sign in to Orris to start your own chat.