Explain interpretation of thyroid profile in diagnosing hypothyroidism and hyper
Reading File
Finding Sources
Finding Sources
Searching the Web
thyroid profile interpretation TSH T3 T4 hypothyroidism hyperthyroidism diagnosis
Finding Sources
Reading Web Page
https://www.thyroid.org/thyroid-function-tests
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive data from Goldman-Cecil, Robbins Pathology, and the American Thyroid Association. I have enough to write a thorough, well-structured answer. Let me compose it now.
Thyroid Profile Interpretation: Hypothyroidism and Hyperthyroidism
The Hypothalamic-Pituitary-Thyroid (HPT) Axis - Why It Matters
Understanding the feedback loop is the key to reading any thyroid result correctly.
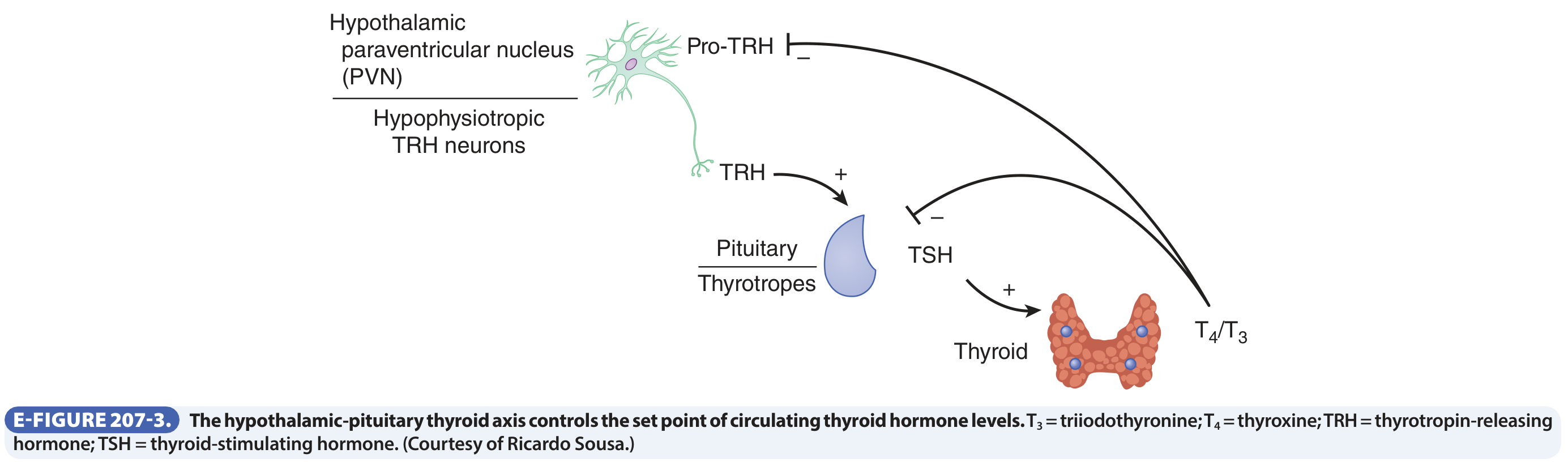
As shown above (Goldman-Cecil Medicine, E-Figure 207-3): TRH (from the hypothalamic paraventricular nucleus) stimulates pituitary thyrotrophs to release TSH, which drives the thyroid to produce T4 and T3. Circulating T4/T3 feeds back negatively at both the hypothalamus and pituitary, suppressing TRH and TSH respectively.
Key implication: TSH behaves as an "early warning system" - it shifts before circulating hormone levels become significantly abnormal. This is why TSH is the single best first-line screening test for thyroid dysfunction. - Goldman-Cecil Medicine
The Tests in the Thyroid Profile
| Test | What It Measures | Reference Range (typical) |
|---|---|---|
| TSH | Pituitary output; indirect reflection of thyroid status | 0.4 - 4.0 mIU/L |
| Free T4 (fT4) | Unbound, biologically active thyroxine (major secretory product) | 0.8 - 1.8 ng/dL |
| Free T3 (fT3) | Unbound triiodothyronine (the most active hormone) | 2.3 - 4.2 pg/mL |
| Total T4 / Total T3 | Bound + free (affected by binding protein changes) | Variable |
| Anti-TPO / Anti-Tg antibodies | Markers of autoimmune thyroid disease | Negative |
| TSH receptor antibodies (TRAb / TSI) | Stimulating Ig in Graves disease | Negative |
Total vs. Free: Total T4/T3 can be misleading because levels change when binding proteins change (e.g., elevated estrogen in pregnancy or on OCPs raises TBG, raising total T4 without true hyperthyroidism). Free T4 and free T3 are preferred because they reflect the biologically active fraction. - American Thyroid Association
Interpreting the Pattern: The Step-by-Step Approach
Step 1 - Check TSH First
TSH is the gateway test:
- High TSH → thyroid is underperforming (hypothyroidism suspected)
- Low TSH → thyroid is overperforming (hyperthyroidism suspected)
- Normal TSH → euthyroid in the vast majority of cases
Step 2 - Check fT4 (and fT3 when needed) to classify severity and localize the defect
Pattern Recognition Table
| TSH | fT4 | fT3 | Interpretation |
|---|---|---|---|
| High | Low | Low/Normal | Overt primary hypothyroidism |
| High | Normal | Normal | Subclinical hypothyroidism |
| Low/Normal | Low | Low | Central (secondary) hypothyroidism - pituitary or hypothalamic failure |
| Low | High | High | Overt primary hyperthyroidism (Graves, toxic MNG, toxic adenoma) |
| Low | Normal | High | T3 toxicosis (early Graves or toxic adenoma) |
| Low | Normal | Normal | Subclinical hyperthyroidism |
| Normal/High | High | High | Central (secondary) hyperthyroidism - TSH-secreting pituitary adenoma |
Hypothyroidism - Detailed Interpretation
Overt Primary Hypothyroidism
- TSH: high + fT4: low
- The most common pattern. The thyroid gland is failing; low T4 removes feedback inhibition from the pituitary, which responds by producing more TSH.
- Common causes: Hashimoto's thyroiditis (autoimmune - most common cause worldwide in iodine-sufficient regions), post-thyroidectomy, post-radioiodine therapy, iodine deficiency, drugs (lithium, amiodarone).
Subclinical Hypothyroidism
- TSH: mildly elevated (4.0-10 mIU/L) + fT4: normal
- The gland is compensating; T4 is maintained at the cost of elevated TSH. Patients may be asymptomatic or have non-specific symptoms.
- Treatment is considered when TSH > 10, or if symptoms present, or in pregnancy.
Central (Secondary/Tertiary) Hypothyroidism
- TSH: low or normal + fT4: low
- Paradoxical - looks like hyperthyroidism (low TSH) but fT4 is also low.
- Cause: pituitary failure (hypopituitarism) or hypothalamic disease reducing TRH.
- This is why you must always check fT4 alongside TSH - a low TSH alone does not confirm hyperthyroidism without checking fT4.
T3 in Hypothyroidism
As the American Thyroid Association notes, T3 is the last test to become abnormal in hypothyroidism. Even in severe hypothyroidism with high TSH and low fT4, T3 may be normal. T3 measurement is therefore rarely helpful for diagnosing hypothyroidism.
Hyperthyroidism - Detailed Interpretation
Overt Primary Hyperthyroidism
- TSH: low (usually < 0.1 mIU/L) + fT4: elevated ± fT3: elevated
- Excess thyroid hormone suppresses the pituitary, driving TSH to near-undetectable levels.
- Causes: Graves disease (~85% of cases), toxic multinodular goiter, toxic (hyperfunctioning) adenoma. - Robbins & Kumar Basic Pathology
T3 Toxicosis
- TSH: low + fT4: normal + fT3: elevated
- Some patients (particularly with early Graves or autonomous nodules) overproduce T3 disproportionately. A low TSH with normal fT4 should prompt free T3 measurement to avoid missing this diagnosis.
Subclinical Hyperthyroidism
- TSH: low + fT4: normal + fT3: normal
- The thyroid is marginally overactive, enough to suppress the pituitary but not raise peripheral hormones above the reference range.
- Important to recognize because it carries risk of atrial fibrillation and bone loss.
Secondary (Central) Hyperthyroidism
- TSH: normal or elevated + fT4: elevated + fT3: elevated
- Rare - caused by a TSH-secreting pituitary adenoma. The inappropriate "normal" or high TSH in the face of high thyroid hormones is the diagnostic clue.
Antibody Tests - Localizing the Cause
Once a thyroid function abnormality is confirmed, antibodies help find the cause:
| Antibody | Positive in | Clinical Use |
|---|---|---|
| Anti-TPO (anti-thyroid peroxidase) | Hashimoto's thyroiditis, Graves | Confirms autoimmune cause of hypothyroidism |
| Anti-thyroglobulin (anti-Tg) | Hashimoto's thyroiditis | Often co-positive with anti-TPO |
| TSH receptor antibodies (TRAb) / TSI | Graves disease | Distinguishes Graves from other causes of hyperthyroidism; also used in pregnancy to predict neonatal Graves |
Common Pitfalls and Confounders
- Biotin supplements artificially falsify results (usually falsely low TSH and falsely high fT4). Patients should stop biotin for at least 2 days before testing.
- Pregnancy / oral contraceptives elevate TBG, raising total T4/T3 without true hyperthyroidism. Always use free hormone levels in these contexts.
- Non-thyroidal illness (sick euthyroid syndrome): Severe illness lowers T3 (decreased peripheral conversion), may lower TSH and fT4. Interpret thyroid tests cautiously in acutely ill patients.
- Amiodarone: Rich in iodine and structurally similar to T4. It can cause both hypo- and hyperthyroidism, and raises total T4 even in euthyroid patients.
- Reverse T3 (rT3): Produced in states of illness/stress; biologically inactive. Measurement is not routinely useful.
- Interference with "free" assays: Some assay platforms can be affected by heterophile antibodies or abnormal binding proteins, giving spuriously abnormal results.
Summary Diagnostic Algorithm
START: Measure TSH
|
─────────────────────────────────
| |
HIGH TSH LOW TSH
| |
Measure fT4 Measure fT4 + fT3
| |
fT4 low → OVERT PRIMARY HYPOTHYROIDISM fT4 high or fT3 high → OVERT HYPERTHYROIDISM
fT4 normal → SUBCLINICAL HYPOTHYROIDISM fT4 + fT3 normal → SUBCLINICAL HYPERTHYROIDISM
fT4 low → CENTRAL HYPOTHYROIDISM
|
If TSH low/normal AND fT4 low → CENTRAL (secondary) HYPOTHYROIDISM
Then, if thyroid dysfunction confirmed:
- Add anti-TPO to confirm autoimmune cause
- Add TRAb/TSI if hyperthyroidism (to confirm or exclude Graves)
- Consider radioactive iodine uptake scan or thyroid ultrasound for structural evaluation
Sources: Goldman-Cecil Medicine (p. 2429-2432, Ch. 207), Robbins & Kumar Basic Pathology (p. 729-733, Ch. 18), American Thyroid Association - Thyroid Function Tests, NHS Hypothyroidism/Hyperthyroidism Diagnosis
This is a shared conversation. Sign in to Orris to start your own chat.