Anatomy and physiology of respiratory system in children very clearly explain neatly everything
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Searching Images
pediatric respiratory anatomy airway child vs adult comparison
Reading File
Loading Image
Searching Images
lung development alveoli neonatal pediatric surfactant
Anatomy & Physiology of the Respiratory System in Children
Overview
The respiratory system in children is not simply a miniature adult system — it is structurally and functionally distinct, and these differences are most pronounced in neonates and infants. Understanding them is critical for clinical care.
1. Development of the Respiratory System
Prenatal Development
| Stage | Timing | What Happens |
|---|---|---|
| Lung bud formation | 4–8 weeks gestation | Lung buds divide into main-stem bronchi |
| Bronchial tree | By 6 weeks | All subsegmental bronchi present |
| Full airway generations | By 16 weeks | Number of airway generations equals that of adults |
| Alveolar precursors (saccules) | Late fetal | Terminal airways remodel into large saccules for gas exchange |
| Type I & II pneumocytes | ~24 weeks | Alveolar cuboidal epithelium flattens; type II cells manufacture surfactant |
| Surfactant production | 23–24 weeks | Appears in low concentration; increases in final 10 weeks |
| Surfactant release into alveoli | ~36 weeks | Makes normal extrauterine life possible |
Key Point: Premature infants born before 36 weeks lack sufficient surfactant, leading to Respiratory Distress Syndrome (RDS).
Postnatal Lung Growth
- At birth: ~24 million alveoli
- By 8 years: ~300 million alveoli (same as adults)
- After age 8, further lung growth comes mainly from increased alveolar size, not new alveoli
- Elastic tissue is sparse at birth and extends only to the alveolar duct
- By 18 years, elastin reaches the alveolus — lung compliance peaks in adolescence
— Miller's Anesthesia, 10e; Morgan & Mikhail's Clinical Anesthesiology, 7e
2. Anatomy of the Pediatric Upper Airway
The Infant/Child Airway vs. Adult Airway
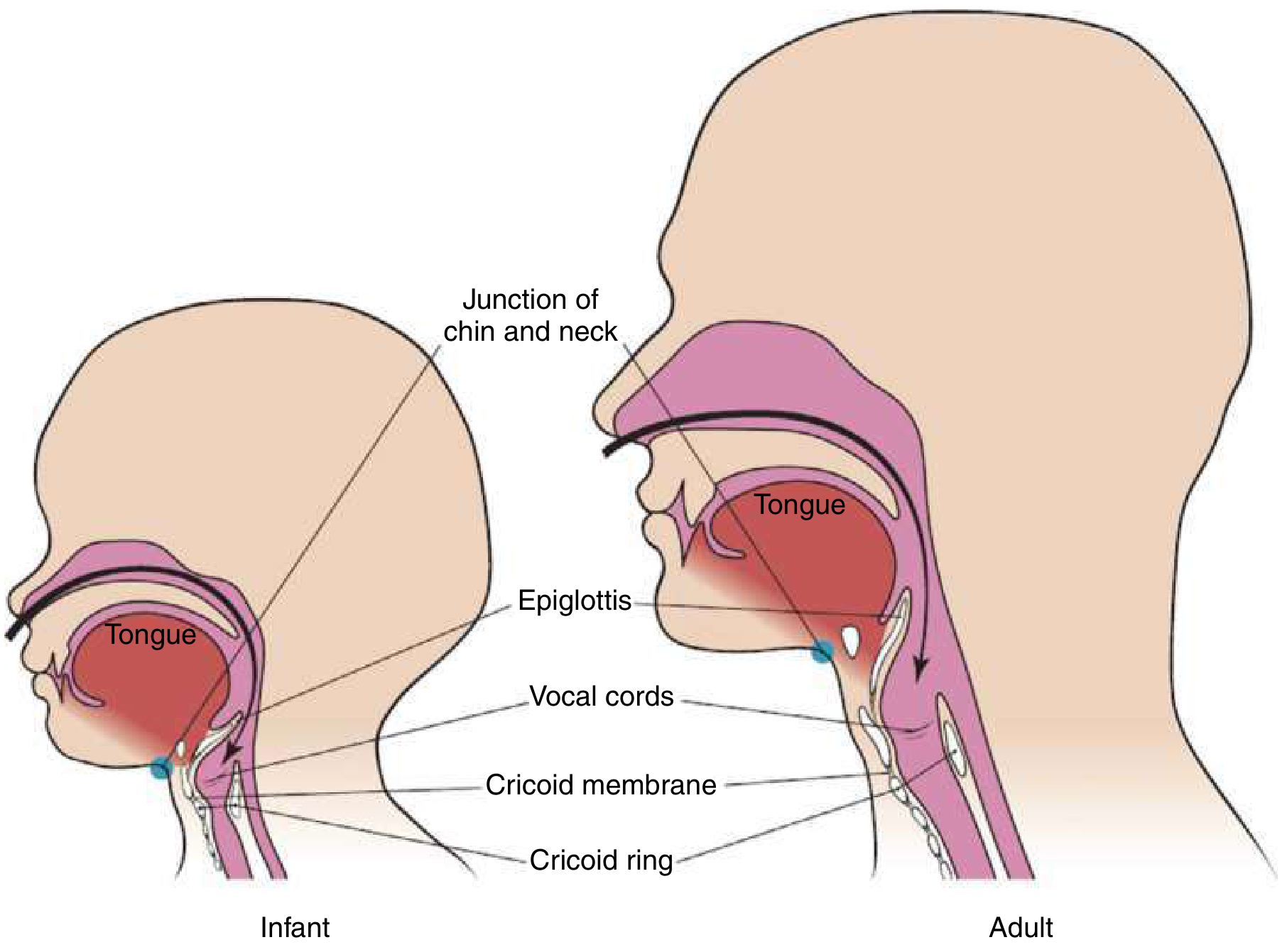
Fig. High, anterior airway of the small child compared with the adult — ROSEN's Emergency Medicine
Key Anatomical Differences
| Feature | Child | Adult | Clinical Implication |
|---|---|---|---|
| Head & Occiput | Disproportionately large | Proportional | Pushes head forward → airway obstruction; use shoulder roll |
| Tongue | Large relative to mouth | Proportional | Occludes airway when sedated/obtunded |
| Nasal passages | Narrower | Wider | Obligate nasal breathing until ~5 months of age |
| Epiglottis | Long, floppy, omega-shaped | Short, stiff | Obscures laryngeal view; may need straight (Miller) blade |
| Larynx position | C1–C2 in neonate, drops to C3–C4 by age 7, C6 in adolescence | C6 | Airway appears "high and anterior" — harder to visualize |
| Glottic angle | Angled anteriorly | More straight | Vocal cords harder to visualize |
| Narrowest point of airway | Cricoid ring (subglottic, <8 yrs) | Glottis (vocal cords) | Edema here is functionally most dangerous |
| Trachea | Short, flexible, prone to collapse | Long, more rigid | Risk of dynamic collapse; accidental extubation |
| Adenoids & tonsils | Relatively large | Smaller | Can obstruct airway; prone to bleeding |
| Cricothyroid membrane | Very small | Larger | Needle cricothyrotomy preferred over surgical in young children |
| Neck | Short | Long | Difficult to identify landmarks |
— Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Sabiston Textbook of Surgery
The "1 mm Rule"
1 mm of mucosal edema in a child's 4 mm trachea reduces cross-sectional area by 50% and increases airway resistance by 200%. In an adult's 8 mm trachea, the same edema reduces area by only 25%.
This explains why croup and epiglottitis are so dangerous in young children.
3. Anatomy of the Lower Airway and Lungs
Trachea & Bronchi
- The trachea is shorter and more flexible than in adults — prone to dynamic collapse
- All airway generations are established by 16 weeks gestation; no new airway branching occurs after birth
- The right main bronchus is more vertical (similar to adults) → right-sided preferential intubation
Chest Wall
- Ribs are cartilaginous and horizontal (rather than oblique as in adults)
- Chest wall is highly compliant — tends to collapse inward during respiratory distress
- Because of this, children rely almost entirely on diaphragmatic breathing
- Intercostal muscles are weak — less contribution to tidal volume
- Abdominal distension (e.g., from gas swallowing) directly compromises breathing
Alveoli & Lung Parenchyma
- Neonates have fewer, smaller alveoli → reduced lung compliance
- Less elastic tissue → reduced elastic recoil
- Airways close within the tidal volume range until about 5 years of age → predisposes to air trapping and atelectasis
4. Respiratory Physiology in Children
Respiratory Rate (Normal Values)
| Age | Normal Respiratory Rate (breaths/min) |
|---|---|
| Neonate (0–1 month) | 40–60 |
| Infant (1–12 months) | 30–50 |
| Toddler (1–2 years) | 24–40 |
| Child (3–5 years) | 22–34 |
| Child (6–12 years) | 18–30 |
| Adolescent (>12 years) | 12–18 (approaching adult) |
Respiratory rate gradually decreases with age toward adult values. Tachypnea is the first and most sensitive sign of respiratory distress in children.
Lung Volumes
| Parameter | Child vs. Adult |
|---|---|
| Tidal volume (mL/kg) | ~7 mL/kg — constant throughout life |
| Dead space (mL/kg) | ~2 mL/kg — constant throughout life |
| Functional Residual Capacity (FRC) | Lower — smaller oxygen reserve |
| Total Lung Capacity | Lower (absolute), proportional per kg |
| Oxygen consumption | 6–8 mL/kg/min (vs. 3–4 mL/kg/min in adults) |
— Morgan & Mikhail's Clinical Anesthesiology, 7e; Tintinalli's EM
Why Children Desaturate So Rapidly
Three factors combine dangerously:
- Low FRC → small oxygen reservoir
- High O₂ consumption (6–8 mL/kg/min vs 3–4 in adults)
- Rapid respiratory rate → any obstruction causes quick decompensation
A fully preoxygenated healthy adult may not desaturate below 90% for ~6 minutes during apnea. A normal 10-kg child may fall below 90% in ~3 minutes. A sick infant may desaturate in under 1 minute.
— Rosen's Emergency Medicine
Compliance and Resistance
- Lung compliance is low (few alveoli, less elastic tissue)
- Chest wall compliance is high (cartilaginous ribs)
- Airway resistance is high because of small airway diameter (Poiseuille's Law: resistance ∝ 1/r⁴)
- Work of breathing is increased, and respiratory muscles fatigue more easily
Control of Ventilation
- Hypoxic and hypercapnic ventilatory drives are not fully developed in neonates and infants
- In contrast to adults, hypoxia may paradoxically depress breathing in neonates (biphasic response: brief increase then depression)
- This is one reason premature infants are at risk for apnea of prematurity
Pulmonary Circulation
| Feature | At Birth | Postnatal Development |
|---|---|---|
| Pulmonary vascular resistance | High (fetal vessels constricted) | Drops dramatically at birth with first breath and O₂ exposure |
| Pulmonary blood flow | Only 7% of combined ventricular output near term | Increases to near-adult levels within hours of birth |
| Arterial wall thickness | Thick muscularized walls | Thins to adult levels in first year of life |
| New artery formation | Ongoing | Continues until ~19 months |
| Supernumerary arteries | Growing | Complete by 8 years |
At birth, as the baby takes its first breath, O₂ causes pulmonary vasodilation. Combined with closure of the ductus arteriosus and foramen ovale, circulation converts from parallel (fetal) to series (adult) within hours.
Surfactant & Surface Tension
- Produced by Type II pneumocytes
- Reduces surface tension in alveoli (prevents collapse at end-expiration)
- Ensures smaller alveoli don't empty into larger ones (LaPlace's Law)
- Deficiency → Respiratory Distress Syndrome (RDS) in premature infants
5. Age-Specific Summary Table
| Feature | Neonate | Infant (1–12 mo) | Child (1–8 yr) | Older Child/Adolescent |
|---|---|---|---|---|
| Alveoli count | 24 million | Rapidly increasing | Reaches 300 million by 8 yrs | 300 million (adult-equivalent) |
| Obligate nasal breathing | Yes (until ~5 months) | Yes (early infancy) | No | No |
| Narrowest airway | Cricoid | Cricoid | Cricoid | Glottis (like adult) |
| Larynx level | C1–C2 | C2–C3 | C3–C4 by age 7 | C6 (adult) |
| Respiratory rate | 40–60 | 30–50 | 22–34 | 12–18 |
| Lung compliance | Very low | Low | Improving | Near-adult (peaks ~adolescence) |
| Hypoxic ventilatory drive | Immature/paradoxical | Developing | Present | Mature |
6. Clinical Pearls — Why Anatomy Matters
| Anatomy/Physiology | Clinical Consequence |
|---|---|
| Large occiput | Neck flexion → need shoulder roll for airway alignment |
| Obligate nasal breathing (neonates) | Even mild nasal congestion can cause significant distress |
| High anterior larynx | Straight (Miller) blade preferred for intubation in infants |
| Cricoid = narrowest point | Use correct ETT size; avoid mucosal trauma causing subglottic edema |
| Short trachea | Right main-stem intubation risk; tape tube carefully |
| Diaphragm-dependent breathing | Abdominal distension (gastric air) directly impairs ventilation |
| Small FRC + high O₂ demand | Always pre-oxygenate; have bag-mask ready before intubating |
| Compliant chest wall | Retractions (intercostal, subcostal, sternal) are reliable signs of respiratory distress |
| Low gastroesophageal sphincter tone | Children swallow air under distress → gastric distension → impaired breathing |
Summary
The pediatric respiratory system differs from the adult in virtually every dimension:
- Anatomically: smaller, more anterior, more compliant, more vulnerable to obstruction
- Physiologically: higher respiratory rates, lower FRC, higher O₂ demand, immature ventilatory control
- Developmentally: alveoli and vasculature mature progressively through childhood, reaching adult equivalence around 8 years of age
These differences mean that children compensate poorly and decompensate rapidly — respiratory failure is the most common cause of cardiac arrest in children, not primary cardiac disease.
Sources: Tintinalli's Emergency Medicine (9e) · Rosen's Emergency Medicine · Miller's Anesthesia (10e) · Morgan & Mikhail's Clinical Anesthesiology (7e) · Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.