Parkland formula paediatrics
Reading File
Finding Sources
Searching PubMed
Parkland formula burns fluid resuscitation pediatric
Finding Sources
Searching PubMed
burns fluid resuscitation pediatric
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have excellent content from both Sabiston and Bailey & Love. I have everything I need for a thorough answer.
Parkland Formula in Paediatrics
The Basic Formula
The modified Parkland (Baxter) formula is:
4 mL x weight (kg) x % TBSA burned = total volume (mL) of Lactated Ringer's over 24 hours
- First half given in the first 8 hours (from time of burn, not time of arrival)
- Second half given over the next 16 hours
Intravenous resuscitation is indicated in children with burns >10% TBSA (vs. >15% in adults).
Key Paediatric Difference: Maintenance Fluids
Unlike adults, children must receive maintenance fluids in addition to the resuscitation volume. This is because:
- Children have a larger surface area to body mass ratio, leading to greater insensible fluid losses
- Their immature kidneys need higher fluid volumes for adequate resuscitation
- Omitting maintenance can cause dangerous hypoglycaemia
Maintenance is calculated using the Holliday-Segar method, typically given as dextrose-saline:
| Weight band | Maintenance rate |
|---|---|
| First 10 kg | 100 mL/kg/24 h |
| Next 10 kg (10-20 kg) | 50 mL/kg/24 h |
| Each kg >20 kg | 20 mL/kg/24 h |
- Bailey and Love's Short Practice of Surgery, 28th Ed.
Limitation of Parkland Formula in Children
Sabiston's Textbook of Surgery notes that the standard adult Parkland formula tends to underresuscitate children with minor burns and overresuscitate large burns because it does not account for TBSA variability as the paediatric patient develops. Two paediatric-specific formulas are preferred in specialist burn centres:
Paediatric-Specific Formulas
Cincinnati Formula
| Age group | Formula |
|---|---|
| Young children | 4 mL/kg/% TBSA burn + 1500 mL/m² total BSA of LR. Half in first 8 h, half in next 16 h. First 8 h: add 50 mEq/L sodium bicarbonate. Third 8 h: add albumin (12.5 g of 25% albumin per litre). Give 5% dextrose as needed. |
| Older children | 4 mL/kg/% TBSA burn + 1500 mL/m² total BSA of LR. Half in first 8 h, remainder in 16 h. 5% dextrose as needed. |
Galveston Formula (body surface area-based)
5000 mL/m² burn area + 2000 mL/m² total BSA of LR
- Half in first 8 h, remainder in 16 h
- Add 12.5 g of 25% albumin per litre of crystalloid
- 5% dextrose as needed
The Galveston formula uses BSA rather than weight, which better accounts for the changing TBSA-to-mass ratio in children.
- Sabiston Textbook of Surgery, 21st Ed. (Table 42.4)
Rule of Nines: Paediatric Modification
The standard adult rule of nines does not apply to children. Because the head is proportionally larger and legs smaller in young children, the Lund and Browder chart should be used. Age-specific TBSA percentages must be applied (see Fig. 42.8 in Sabiston).
Monitoring
Fluid resuscitation is dynamic - rigid adherence to formulae is not appropriate. The primary monitor is urine output:
| Weight | Target urine output |
|---|---|
| <30 kg | 1 mL/kg/h |
| >30 kg | 0.5 mL/kg/h |
If urine output drops with signs of hypoperfusion (tachycardia, cool peripheries, raised lactate), give a bolus of 10 mL/kg. Avoid over-resuscitation, which leads to fluid creep, pulmonary oedema, and abdominal compartment syndrome.
Timing Note
Resuscitation starts from the time of burn, not time of arrival. Any prehospital delay must be accounted for when calculating the rate for the first 8-hour window.
- Bailey and Love's Short Practice of Surgery, 28th Ed.
- Sabiston Textbook of Surgery, 21st Ed.
Teach me ctev with images and mnemonics
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
I now have all the content I need for a comprehensive, image-rich teaching answer. Let me compile it.
CTEV - Congenital Talipes Equinovarus (Clubfoot)
The Master Mnemonic: CAVE
Cavus - Adduction of forefoot - Varus of hindfoot - Equinus
This single word describes all 4 deformities of CTEV AND the order of correction in Ponseti casting.
What Exactly Is CTEV?
CTEV is a complex 3D deformity of the foot and ankle where the foot is:
| Component | What it means | Visual cue |
|---|---|---|
| Cavus | High arch (plantar flexion of forefoot on hindfoot) | "Caved-in" arch |
| Adduction | Forefoot turned inward (medially) | Toes point in |
| Varus | Hindfoot inverted (heel turns in) | Sole faces up |
| Equinus | Plantarflexion at ankle (foot points down) | Like a horse hoof |
The foot is small, stiff, and the sole faces inward/upward.
Skeletal Anatomy - Side by Side Comparison
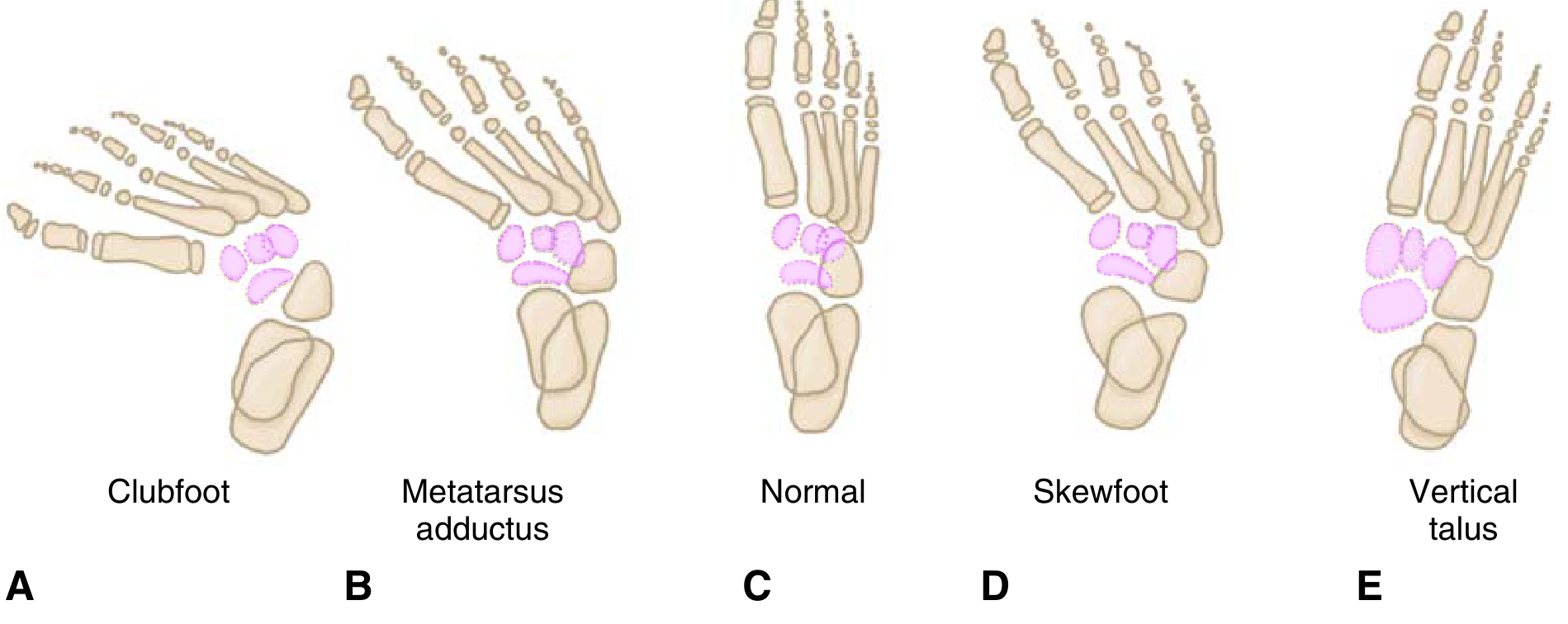
A - Clubfoot: varus hindfoot + adducted forefoot. B - Metatarsus adductus: normal hindfoot, adducted forefoot only. C - Normal foot. D - Skewfoot. E - Congenital vertical talus (rocker-bottom).
The key diagnostic differentiator: in CTEV both the hindfoot (varus) and forefoot (adduction) are abnormal. In metatarsus adductus, only the forefoot is adducted.
Radiographic Findings
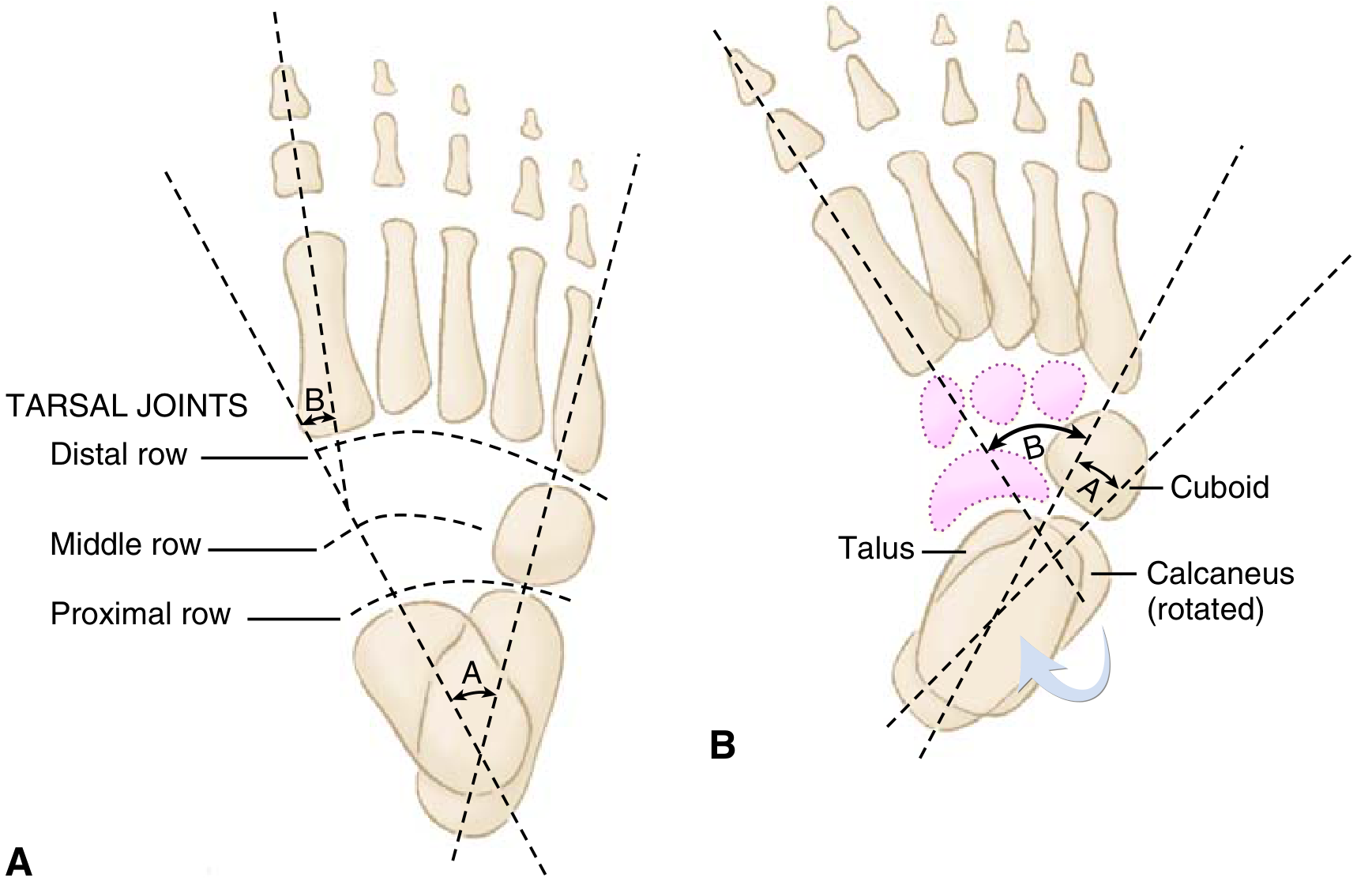
A - Normal foot: talus and calcaneus diverge (angle A normal = 20-40° on AP). B - Clubfoot: talus and calcaneus are PARALLEL (talocalcaneal angle <20°). The talus-1st metatarsal angle (B) is negative in clubfoot.
Radiographic Angles (Mnemonic: "Small angles, big problem")
| View | Angle | Normal | Clubfoot |
|---|---|---|---|
| AP (Kite angle) | Talocalcaneal angle | 20-40° | <20° |
| Lateral (Turco) | Talocalcaneal angle | ~35° | <35° |
| AP | Talus-1st metatarsal angle | 0-20° | Negative |
The "parallelism" of talus and calcaneus on X-ray is the hallmark - they normally diverge like a V, but in CTEV they run parallel.
Note: X-rays are rarely used in infants due to minimal ossification - mainly used when diagnosis is unclear or in older patients.
Epidemiology
Mnemonic: "Boys get it Twice, Half get it on Both sides"
- Incidence: ~1-2 per 1000 live births
- Sex: Boys affected twice as often as girls (2:1 M:F)
- Bilateral: 50% of cases are bilateral
- Idiopathic: majority, though PITX1-TBX4 transcriptional pathway implicated
Aetiology - Mnemonic: "MAGIC"
Myelomeningocele - Arthrogryposis - Genetic (idiopathic) - Intrauterine positional - Chromosomal/syndromic
| Category | Examples |
|---|---|
| Idiopathic (most common) | PITX1-TBX4 pathway; genetic predisposition |
| Neuromuscular | Myelomeningocele, spina bifida |
| Syndromic | Arthrogryposis, diastrophic dwarfism, prune-belly syndrome |
| Structural | Tibial hemimelia, Streeter dysplasia |
| Positional | Intrauterine compression (resolves spontaneously - ~10%) |
90% of prenatally detected cases have structural defects needing treatment; 10% are positional and resolve on their own.
Pathoanatomy
The primary bony deformity is at the talus:
- Talar neck has medial and plantar deviation
- Calcaneus rotates medially
- Navicular and cuboid displace medially
This drives contractures of:
- Medial structures: tibialis posterior, flexor hallucis longus, flexor digitorum longus
- Posterior structures: Achilles tendon
- Fascial structures: plantar fascia, joint capsules, ligaments
Associated finding: absence or diminution of the anterior tibial artery (important for surgical planning - the posterior tibial artery must be protected during posteromedial release).
Severity Scoring
Two systems are used postnatally:
Pirani Score (0-6)
- 6 signs scored 0/0.5/1 each
- Hindfoot score (3 signs): equinus, empty heel, posterior crease
- Midfoot score (3 signs): medial crease, curved lateral border, talar head coverage
- Higher score = more severe; predicts number of casts needed
Dimeglio Classification (0-20)
- Grades equinus, varus, derotation, adduction
- Grade I (benign) to Grade IV (very severe/teratologic)
Treatment
Primary Treatment: Ponseti Method (>90% success)
Mnemonic for correction order: CAVE (same as the deformities, corrected in this sequence)
| Step | Correction | How |
|---|---|---|
| 1. Cavus | First | Supinate forefoot, dorsiflex 1st ray |
| 2. Adductus | Second | Lateral pressure on distal talar head as fulcrum |
| 3. Varus | Simultaneous with adductus | Same lateral pressure manoeuvre |
| 4. Equinus | Last | Gradual dorsiflexion after above corrected |
Key rule: Never try to correct equinus before varus is corrected - this creates a rocker-bottom deformity.
The process:
- Serial weekly manipulations + long-leg plaster casts (usually 4-7 casts)
- 90% of patients undergo percutaneous Achilles tenotomy at the end to address equinus
- Final cast in 70 degrees of abduction
- Foot abduction brace (Denis Browne splint): full-time for 3 months, then night/nap use for 3 years
- Brace non-compliance is the #1 cause of recurrence
Complications of Ponseti
- Recurrence (most common) - re-cast, may need tibialis anterior transfer
- Rocker-bottom deformity - from correcting equinus before varus
- Flat-top talus - from aggressive dorsiflexion causing talar dome flattening
Operative Treatment (only ~5% of idiopathic CTEV)
Reserved for resistant/refractory cases:
| Age | Procedure |
|---|---|
| <1 year (failed Ponseti) | Posteromedial soft tissue release (PMR/Cincinnati approach) - tendon lengthening + subtalar, tibiotalar, talonavicular release |
| 3-10 years | Medial opening-wedge osteotomy, lateral column-shortening osteotomy, or cuboid decancellation |
| Late presentation / older child | Triple arthrodesis (subtalar + talonavicular + calcaneocuboid fusion) |
Surgical caution: protect the posterior tibial artery - the dorsalis pedis is often absent or inadequate in CTEV.
Prenatal Diagnosis
- Diagnosed on antenatal ultrasound (18-24 weeks)
- Look for fixed position of foot with toes pointing medially
- Bilateral clubfoot increases risk of aneuploidy/genetic syndrome
- Amniocentesis NOT recommended for isolated clubfoot
- 75% of complex clubfoot cases diagnosed at 18-24 weeks
Quick Summary Card
CTEV = CAVE deformities
(Cavus + Adduction + Varus + Equinus)
Epidemiology:
2:1 males | 50% bilateral | 1-2/1000 births
X-ray:
Parallelism of talus + calcaneus
Talocalcaneal angle <20° (AP)
Treatment:
Ponseti casting → order = CAVE
90% need Achilles tenotomy
Brace 3 years post-casting
Only 5% need surgery
Never correct E before V → rocker-bottom!
- Miller's Review of Orthopaedics, 9th Ed.
- Schwartz's Principles of Surgery, 11th Ed.
- Creasy & Resnik's Maternal-Fetal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.