Pancytopenia treatment and management
Reading File
Finding Sources
Finding Sources
Searching PubMed
pancytopenia management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
I have comprehensive content from Harrison's treatment section. Now I have all I need to compile a thorough response. Let me synthesize everything.
Pancytopenia: Treatment and Management
Pancytopenia is the simultaneous reduction of all three peripheral blood cell lines (red cells, white cells, and platelets). Treatment is fundamentally etiology-driven - there is no single "pancytopenia treatment." Management follows a structured approach: identify the mechanism, treat the cause, and provide supportive care.
Step 1: Determine the Mechanism and Cause
Before treating, classify by bone marrow findings:
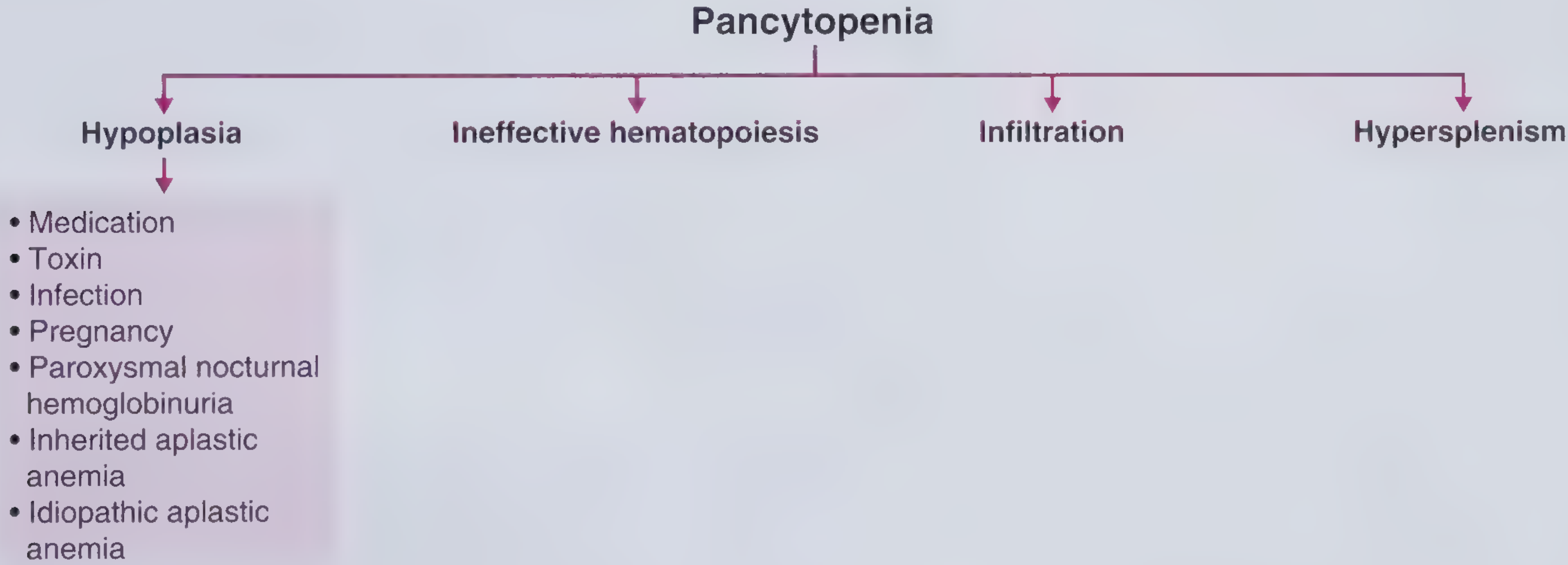
| Mechanism | Bone Marrow | Key Causes |
|---|---|---|
| Hypoplasia | Hypocellular | Aplastic anemia, drugs, toxins, infections (parvovirus, EBV), PNH, Fanconi anemia |
| Ineffective hematopoiesis | Normo/hypercellular | B12/folate deficiency, MDS, copper deficiency |
| Infiltration | Replaced by abnormal cells | Leukemia, lymphoma, myelofibrosis, metastatic cancer, TB, sarcoidosis |
| Hypersplenism | Normal/hypercellular | Cirrhosis/portal hypertension, lymphoma, Felty syndrome, leishmaniasis, Gaucher disease |
Harrison's Principles of Internal Medicine 22E, Table 107-1
Step 2: Treat the Underlying Cause
A. Aplastic Anemia (Immune-mediated, Hypocellular Marrow)
This is the most intensively managed cause. Treatment depends on disease severity and patient age.
Severity Classification (severe aplastic anemia = 2 of 3):
- Absolute neutrophil count (ANC) < 500/μL
- Platelets < 20,000/μL
- Corrected reticulocyte count < 1% (or absolute reticulocytes < 60,000/μL)
Definitive Therapy
1. Hematopoietic Stem Cell Transplant (HSCT)
- Treatment of choice for severe aplastic anemia in patients <40 years with a matched sibling donor
- Cure rate approaches 80-90% with matched sibling transplant
- Preferred over immunosuppression in younger patients due to superior long-term outcomes and avoidance of relapse/clonal evolution
- Conditioning uses cyclophosphamide ± anti-thymocyte globulin (ATG)
2. Immunosuppressive Therapy (IST)
- For patients who are not transplant candidates (older age, no matched donor, comorbidities)
- Standard regimen: horse ATG (hATG) + cyclosporine + eltrombopag
- hATG is preferred over rabbit ATG for treatment-naive patients
- Cyclosporine continued for at least 2 years to prevent relapse
- Eltrombopag (thrombopoietin receptor agonist) added to standard IST significantly improves response rates
- Response is assessed at 3-6 months; non-responders may receive a second course of IST or proceed to alternative donor transplant
Note: Glucocorticoids alone are NOT appropriate as primary therapy for aplastic anemia and increase susceptibility to fungal infection.
Harrison's Principles of Internal Medicine 22E, Chapter 107
B. Nutritional Deficiencies (B12/Folate - Megaloblastic Pancytopenia)
- Most common cause of pancytopenia in the developing world
- Characterized by macrocytosis, hypersegmented neutrophils, hypercellular marrow with nuclear-cytoplasmic dissociation
- Treatment: Replace the deficient nutrient
- Vitamin B12 deficiency: Parenteral cyanocobalamin (1000 mcg IM) - monthly maintenance injections; intranasal formulations also available. Recovery of counts is rapid (reticulocyte peak ~20-25% in 5-7 days)
- Folate deficiency: Oral folic acid supplementation
- If neurologic involvement, high-frequency B12 administration is important as neurologic recovery is slow
- Liver stores B12 well - several years for relapse even after stopping treatment
Textbook of Family Medicine 9e; Frameworks for Internal Medicine
C. Drug/Toxin-Induced Pancytopenia
- Remove the offending agent - this is always the first step
- Examples: chloramphenicol, linezolid, chemotherapy, NSAIDs (indomethacin), antithyroid agents (methimazole, PTU), anticonvulsants (carbamazepine), lithium, alcohol
- For alcohol-related: Typically reversible upon cessation; thrombocytopenia resolves quickly; sideroblastic changes resolve more slowly
- For dose-related chemotherapy: Myeloid growth factors (G-CSF, GM-CSF) can shorten neutropenia duration
- For idiosyncratic drug reactions causing aplastic anemia: treat as aplastic anemia (IST or transplant)
Textbook of Family Medicine 9e
D. Myelodysplastic Syndrome (MDS)
- Clonal stem cell disorder with ineffective hematopoiesis, normo/hypercellular marrow
- Treatment is risk-stratified (IPSS-R score):
- Low/intermediate risk: Erythropoiesis-stimulating agents (ESAs), lenalidomide (for del 5q), transfusion support
- High/very-high risk: Hypomethylating agents - azacitidine or decitabine (prolong survival, delay AML progression); allogeneic HSCT for eligible patients is the only potentially curative option
- Luspatercept for ESA-refractory lower-risk MDS with ring sideroblasts
E. Hypersplenism
- Treat the underlying cause of splenomegaly (e.g., antiviral therapy for hepatitis C cirrhosis, chemotherapy for lymphoma, enzyme replacement therapy for Gaucher disease)
- Splenectomy may be curative when hypersplenism is the sole driver of pancytopenia
- Splenomegaly can sequester up to 90% of platelets, 65% of granulocytes, and 30% of red cells
Frameworks for Internal Medicine
F. Bone Marrow Infiltration (Myelophthisis)
- Treat the infiltrating disease: chemotherapy for leukemia/lymphoma, anti-TB treatment for tuberculosis, etc.
- Extramedullary hematopoiesis with teardrop cells and leukoerythroblastosis on smear are characteristic
G. Paroxysmal Nocturnal Hemoglobinuria (PNH)
- Eculizumab (anti-C5 complement inhibitor) - dramatically reduces hemolysis and thrombosis
- Ravulizumab - longer-acting alternative
- HSCT for patients with aplastic anemia/PNH overlap
Step 3: Supportive Care (All Causes)
Supportive care is critical regardless of the underlying etiology, especially while awaiting treatment response.
| Support | Indication | Details |
|---|---|---|
| RBC transfusions | Symptomatic anemia (Hb <7-8 g/dL) | Use leukoreduced, irradiated products in transplant candidates |
| Platelet transfusions | Platelets <10,000/μL or <20,000/μL with active bleeding | Prophylactic threshold in aplastic anemia |
| G-CSF / GM-CSF | Severe neutropenia (ANC <500) | Especially post-chemotherapy; limited role in aplastic anemia |
| Antibiotics | Febrile neutropenia | Broad-spectrum empiric coverage (e.g., piperacillin-tazobactam or cefepime); add antifungals if unresponsive |
| Antifungal prophylaxis | ANC <500 for >7 days | Fluconazole or posaconazole |
| Iron chelation | Chronic transfusion-dependent patients (>20 units RBC) | Deferasirox, deferoxamine to prevent hemosiderosis |
| Avoid immunizations | Live vaccines contraindicated | During immunosuppression |
Step 4: Monitoring
- Bone marrow biopsy and aspiration with cytogenetics is essential in most cases - especially when malignancy is suspected
- Flow cytometry and chromosomal analysis significantly improve diagnostic precision
- Abdominal ultrasound for spleen size assessment is cost-effective and important
- In aplastic anemia treated with IST: monitor for clonal evolution to MDS or AML (occurs in ~15% at 10 years), and monitor for PNH clone expansion
- Telomere length testing helps identify telomere biology disorders (dyskeratosis congenita)
Special Considerations
Pediatric / Fanconi Anemia:
- Inherited causes (Fanconi anemia, Shwachman-Diamond, telomere disorders) require genetic testing
- HSCT is the only curative option; androgens (oxymetholone) can temporarily improve counts
- Fanconi anemia requires modified conditioning (hypersensitive to alkylating agents and radiation)
Pregnancy-associated:
- Mild pancytopenia can occur in normal pregnancy
- PNH can worsen; aplastic anemia may flare
- IST with cyclosporine may be used; avoid teratogenic agents
PNH overlap:
- Even small PNH clones in aplastic anemia indicate immune pathophysiology and suggest likely responsiveness to IST
Key Clinical Principle
"It is important that the internist and general practitioner recognize the marrow failure syndromes because quality of life and prognosis is poor if the patient is untreated; effective therapies are often available but sufficiently complicated in their choice and delivery so as to warrant the care of a hematologist or oncologist."
- Harrison's Principles of Internal Medicine 22E, Chapter 107
Pancytopenia always warrants hematology referral. Empiric treatment without a diagnosis risks missing a treatable or curable condition.
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 107 - Bone Marrow Failure Syndromes
- Frameworks for Internal Medicine - Chapters on Hypoplasia, Ineffective Hematopoiesis, Hypersplenism
- Textbook of Family Medicine 9e - Pancytopenia
This is a shared conversation. Sign in to Orris to start your own chat.