SLE internal medicine of harrison
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from Harrison's 22nd edition. Let me compile the full answer.
Systemic Lupus Erythematosus (SLE)
Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Chapter 368
Definition, Prevalence, and Epidemiology
SLE is an autoimmune disease in which overactive innate and adaptive immune systems cause tissue damage through the effects of autoantibodies and immune complexes. Many organ systems are affected, with cutaneous, musculoskeletal, and renal systems most involved, followed by pulmonary, hematologic, cardiovascular, serosal, and CNS involvement.
Epidemiology:
- ~90% of affected individuals are women, most of childbearing age
- US prevalence (CDC National Lupus Registry): ~204,295 cases; overall prevalence 9x higher in women vs. men
- Highest prevalence in Black women, then Hispanic, White, and Asian/Pacific Islander women
- Among men, Black men have the highest prevalence
- Autoantibodies can be detected years before clinical diagnosis
Diagnosis and Classification
Diagnosis requires an individualized clinical approach, excluding other entities. Classification criteria (used for clinical trial enrollment, not diagnosis):
| Criteria System | Key Requirements |
|---|---|
| 2019 EULAR/ACR | ANA ≥1:80 required; points scored across clinical domains; ≥10 points needed |
| 2012 SLICC | Alternate validated set for clinical trials |
Special notes:
- Only a renal biopsy showing Class III or IV lupus nephritis alone reaches 10 points in EULAR/ACR
- ~5% of SLE patients are ANA-negative (excluded from most trials)
- Type 1 lupus: classic inflammatory findings (nephritis, arthritis, vasculitis) - responds to immunosuppression
- Type 2 lupus: fatigue, diffuse pain, depression, cognitive dysfunction, brain fog - less responsive to immunosuppressive therapy
Pathogenesis
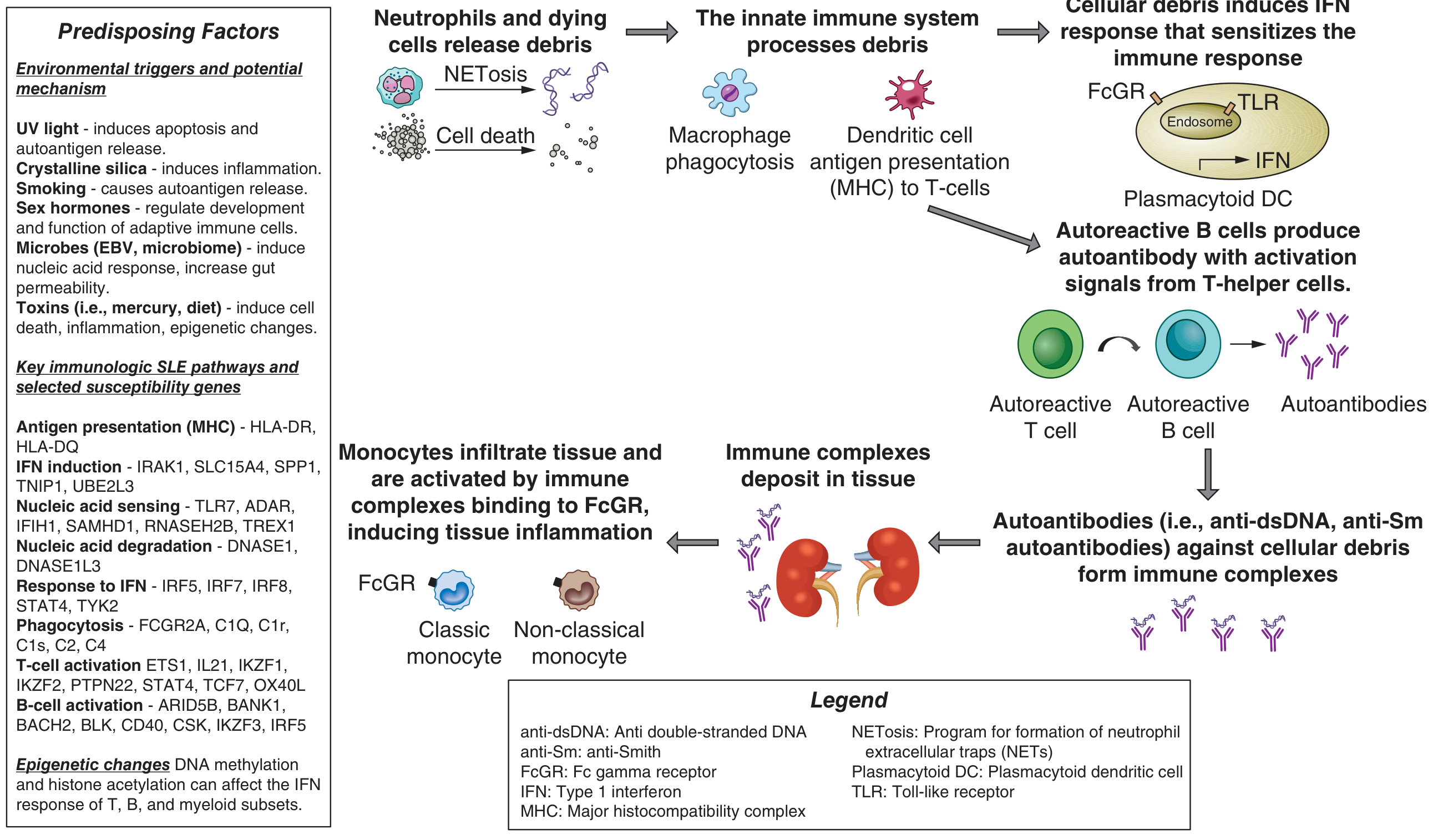
Figure 568-1: Pathogenesis of SLE - environmental triggers, innate immune activation, type 1 IFN, autoantibody formation, and tissue immune complex deposition.
Genetics
- Strong genetic component: 24% concordance in monozygotic vs. 2% in dizygotic twins
-
150 susceptibility loci identified by GWAS
- Most common association: MHC region (antigen presentation, complement, cytokines)
- Nearly half of susceptibility loci involve type I interferon (IFN) production or signaling
- Key IFN pathway genes: TLR7, ADAR, IFIH1, SAMHD1, RNASEH2B, TREX1 (nucleic acid sensing/metabolism); DNASE1, DNASE1L3 (nucleic acid degradation); IRF5, IRF7, IRF8, STAT4 (IFN amplification)
- Complement cascade genes (C1Q, C1r, C1s, C2, C4) - deficiency leads to impaired clearance of apoptotic debris and severe SLE
Environmental Triggers
- UV light: alters DNA methylation, generates self-stimulatory nucleic acids, activates keratinocyte immune responses
- Epstein-Barr virus: induces IFN response, activates SLE susceptibility genes
- Gut microbiome: increased gut permeability promotes translocation of microbes into blood, triggering lupus-specific autoantibodies
- Toxins: mercury, pesticides, diet
Innate Immunity
- Defects in innate immune cells lead to increased cellular breakdown and reduced debris clearance
- Plasmacytoid dendritic cells produce large amounts of type I IFN, sensitizing both innate and adaptive immune responses
- Neutrophil NETosis releases autoantigens (nucleic acids, nuclear proteins)
Adaptive Immunity
- Autoreactive T cells activate autoreactive B cells
- B cells produce autoantibodies (anti-dsDNA, anti-Sm) against cellular debris
- Immune complexes deposit in tissues (notably kidneys, skin, joints)
- Monocytes infiltrate tissue, activated by immune complexes via FcgR, inducing local inflammation
Clinical Manifestations
Cutaneous Manifestations

Figure 568-2: A. Jaccoud arthropathy (nonerosive, reversible joint deformity). B. Patchy nonscarring alopecia. C. Patchy scarring alopecia. D. Discoid lupus with scarring alopecia. E. Classic photosensitive malar (butterfly) rash. F. SCLE with widespread photosensitive nonscarring lesions.
Acute cutaneous LE:
- "Butterfly" malar erythema across nose and cheeks
- Sudden onset, edema, fine scale - correlates with systemic activity
- Histology: hydropic degeneration of basal keratinocytes, dermal edema, perivascular mononuclear infiltrate, dermal mucin
- Direct immunofluorescence: Ig and complement deposits at epidermal basement membrane zone
Subacute cutaneous LE (SCLE):
- Widespread photosensitive, nonscarring eruption
- Two forms: papulosquamous (resembles psoriasis) or annular/polycyclic
- More widespread than discoid LE but less scarring
- Drug-induced SCLE: hydrochlorothiazide, calcium channel blockers, antifungals, proton pump inhibitors
- Most SCLE patients have anti-Ro (SS-A) autoantibodies
Chronic (discoid) LE:
- Scarring plaques predominantly on face, scalp, ears
- Can cause permanent hair loss (scarring alopecia)
Other skin manifestations:
- Photosensitivity, oral/nasal ulcers, Raynaud's phenomenon, livedo reticularis
Musculoskeletal Manifestations
- Arthritis in the majority of patients; most common initial complaint
- Jaccoud arthropathy: nonerosive, reversible joint deformities (unlike RA), caused by joint capsule inflammation and fibrotic retraction, with MCP subluxation
- Myositis and myalgias may also occur
Renal Manifestations (Lupus Nephritis)
Classified by the 2018 ISN/RPS criteria:
| Class | Description |
|---|---|
| I | Minimal mesangial lupus nephritis |
| II | Mesangial proliferative LN |
| III | Focal LN (<50% glomeruli affected) |
| IV | Diffuse LN (≥50% glomeruli; most severe, most common) |
| V | Membranous LN |
| VI | Advanced sclerosing LN |
- Class III/IV LN = most severe; Class IV alone meets EULAR/ACR classification threshold
- Monitoring: urine protein-to-creatinine ratio, urinalysis, serum creatinine, complement levels, anti-dsDNA titers
Vascular/Cardiovascular Manifestations
- Accelerated atherosclerosis: major cause of morbidity/premature death; driven by type 1 IFN and vascular injury
- Antiphospholipid syndrome (APS): occurs commonly in SLE; arterial, venous, or small vessel thrombosis in the presence of antiphospholipid antibodies
- Stroke: reported in up to 19% of SLE patients (from atherosclerosis + APS)
- Libman-Sacks endocarditis: fibrinous sterile endocarditis associated with antiphospholipid antibodies; risk for embolic events
- Pericarditis: most common cardiac manifestation; managed with anti-inflammatories, colchicine, anti-IL-1 therapies
- Myocarditis: rarer; can cause left heart failure/arrhythmia
Pulmonary Manifestations
- Pleuritis (most common): with or without exudative effusions
- Acute pneumonitis (imaging may mimic infection)
- Diffuse alveolar hemorrhage with capillaritis
- Interstitial lung disease
- Shrinking lung syndrome: restrictive defect from reduced lung volumes (uncommon)
- Pulmonary arterial hypertension, pulmonary embolism (with or without APS)
Hematologic Manifestations
- Anemia (most common, >50% of cases): mainly anemia of chronic disease
- Also: autoimmune hemolytic anemia (Coombs-positive)
- Leukopenia, lymphopenia
- Thrombocytopenia (immune-mediated)
- All cytopenias may be multifactorial (disease activity, medications, infection)
Neuropsychiatric SLE (NPSLE)
- Seizures, transverse myelitis (linked to APS)
- Cognitive dysfunction, brain fog, depression, anxiety (type 2 lupus features)
- Cerebritis (severe, organ-threatening)
- CNS manifestations are not a recommended indication for belimumab or anifrolumab
Key Autoantibodies in SLE
| Antibody | Specificity / Clinical Relevance |
|---|---|
| Anti-dsDNA | Highly specific for SLE; correlates with disease activity, especially nephritis |
| Anti-Sm (Smith) | Highly specific for SLE; less sensitive |
| Anti-Ro (SS-A) | Associated with SCLE, photosensitivity, neonatal lupus, congenital heart block |
| Anti-La (SS-B) | Associated with anti-Ro; neonatal lupus |
| Antiphospholipid antibodies | Associated with APS, thrombosis, pregnancy morbidity |
| Anti-histone | Drug-induced lupus |
| ANA | Sensitive (not specific); required for EULAR/ACR criteria (≥1:80) |
| Low complement (C3, C4) | Marker of active disease, especially nephritis |
Pregnancy in SLE
- SLE pregnancies are high risk; disease can flare any trimester
- Higher rates of: pregnancy loss, preterm birth, preeclampsia, IUGR, cesarean section, maternal death
- Highest risk for maternal death: pulmonary arterial hypertension, prior arterial thrombosis, severe end-organ damage - should strongly consider avoiding pregnancy
Safe in pregnancy: HCQ (standard of care for all SLE pregnancies), azathioprine, tacrolimus, low-dose aspirin (preeclampsia prevention), prednisone (lowest effective dose)
Contraindicated/avoid in pregnancy: MMF (teratogenic), methotrexate (teratogenic), warfarin (teratogenic - use LMWH instead), belimumab, anifrolumab, voclosporin (insufficient safety data)
Neonatal Lupus
- Anti-Ro (SS-A) antibodies cross the placenta and can cause:
- Transient cutaneous rash or lab abnormalities (resolves)
- Congenital heart block (can be irreversible if complete)
- Management: fetal echocardiography to screen; fluorinated steroids if 1st- or 2nd-degree heart block detected
- HCQ significantly reduces risk of recurrent congenital heart block
Treatment
General Measures (All Patients)
- Daily sunscreen on sun-exposed areas
- Healthy diet, maintain normal weight
- Avoid smoking (impairs antimalarial efficacy)
- Regular exercise
- Up-to-date vaccinations
- Control of blood pressure, lipids, glucose
Pharmacotherapy
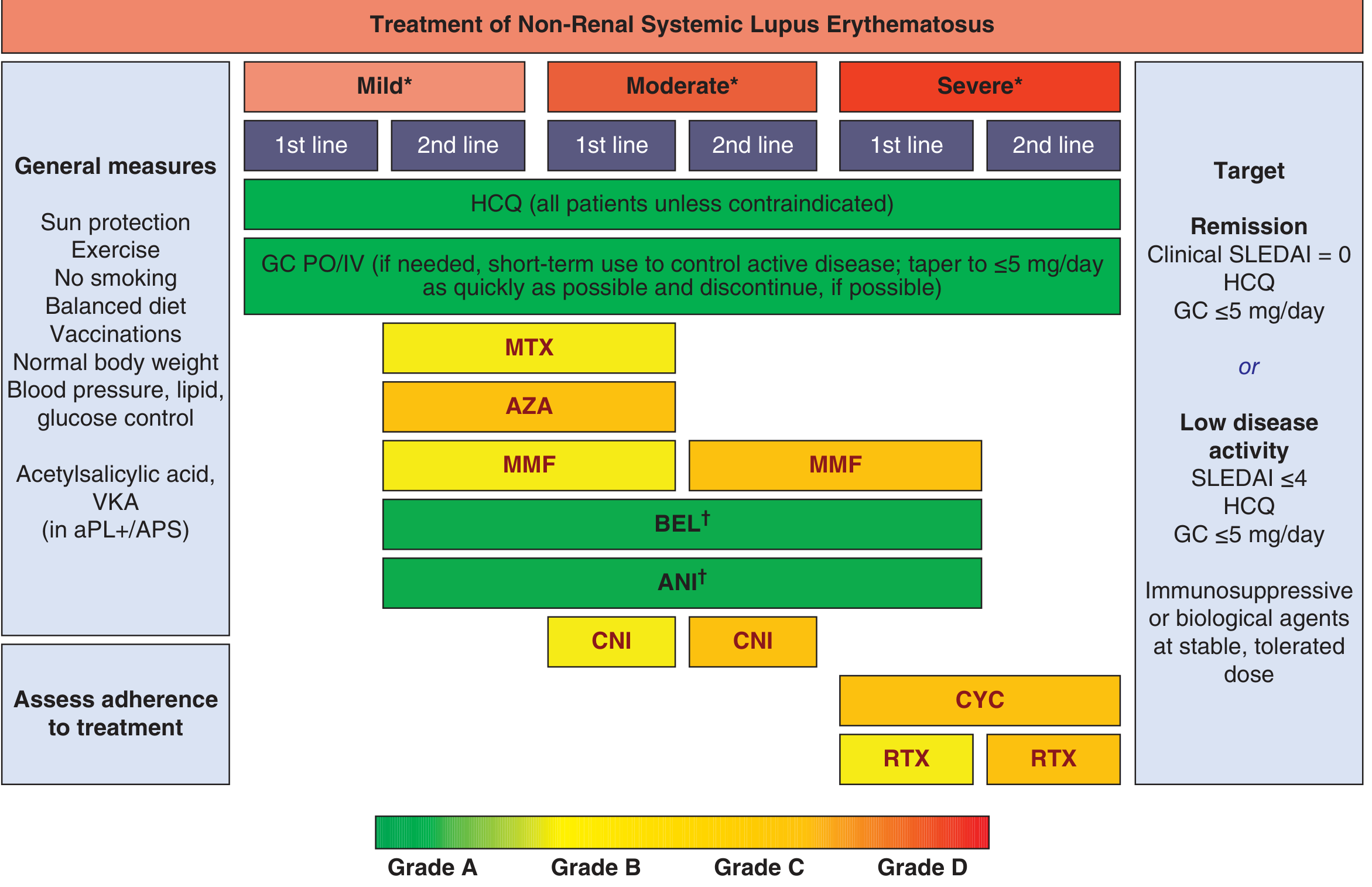
Figure 368-4: Treatment algorithm for non-renal SLE by disease severity (mild/moderate/severe). HCQ is the backbone for all patients.
Hydroxychloroquine (HCQ) - Backbone of all SLE therapy:
- First-line for ALL patients unless contraindicated
- Prevents flares, increases survival, decreases renal disease, reduces atherosclerosis
- First-line for skin and joint manifestations; most useful drug for fatigue
- Safe in pregnancy and breastfeeding
- Dosing: up to 5 mg/kg/day (actual body weight)
- Monitoring: baseline and annual retinal exams (risk of macular toxicity with long-term use)
- Risk factors for retinal toxicity: higher dose, longer duration
Glucocorticoids:
- Short-term use to control acute flares
- Taper to ≤5 mg/day prednisone as quickly as possible
- Discontinue if possible; long-term high-dose use associated with damage accrual
Mild-to-Moderate Disease (second-line immunosuppressants):
- Methotrexate (MTX)
- Azathioprine (AZA)
- Mycophenolate mofetil (MMF)
- Calcineurin inhibitors (CNI: tacrolimus, cyclosporine)
Biologics:
- Belimumab (anti-BLYS/BLyS): FDA-approved for active SLE; reduces flares, protects against organ damage; not recommended in severe neuropsychiatric disease
- Anifrolumab (anti-IFNAR1, type I IFN receptor blocker): FDA-approved; particularly effective for severe skin disease as add-on; not recommended in severe neuropsychiatric disease
Severe/Organ-Threatening Disease:
- IV cyclophosphamide (CYC): for cerebritis, myelitis, pneumonitis, mesenteric vasculitis, severe thrombocytopenia
- Rituximab (RTX): anti-CD20; used for refractory disease; can be continued in organ-threatening pregnancy
- High-dose IV glucocorticoids (pulse methylprednisolone)
Lupus Nephritis Treatment:
- Class III/IV: MMF or cyclophosphamide as induction + glucocorticoids; then maintenance MMF or AZA
- Voclosporin (calcineurin inhibitor): FDA-approved for lupus nephritis in combination with MMF
- Belimumab: approved as add-on therapy for active lupus nephritis
- Class V (membranous): MMF is preferred
Antiphospholipid Syndrome in SLE:
- Long-term anticoagulation with warfarin or LMWH for thrombotic APS
- Low-dose aspirin + hydroxychloroquine for primary prevention
- Avoid DOACs in APS with triple-positive antibodies
Treat-to-Target Goals
- Remission: Clinical SLEDAI = 0, on HCQ, glucocorticoids ≤5 mg/day
- Lupus Low Disease Activity State (LLDAS): SLEDAI ≤4, HCQ, glucocorticoids ≤5 mg/day, immunosuppressives at stable dose
Drug-Induced Lupus
Distinct from SLE:
- Associated with anti-histone antibodies
- Common drugs: hydralazine, procainamide, isoniazid, minocycline, TNF-alpha inhibitors
- Typically resolves on discontinuation of the offending drug
- Renal and CNS involvement rare (unlike SLE)
Monitoring Disease Activity
Key tools:
- SLEDAI (Systemic Lupus Erythematosus Disease Activity Index): widely used clinical score
- BILAG: British Isles Lupus Assessment Group
- Laboratory: CBC, urinalysis, urine protein:creatinine ratio, serum creatinine, complement (C3/C4), anti-dsDNA titers
- CLASI: Cutaneous Lupus Disease Area and Severity Index (for skin disease in trials)
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 368 - Systemic Lupus Erythematosus (Smith, Hoover, Kalunian)
This is a shared conversation. Sign in to Orris to start your own chat.