Explain about heart function
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
I now have comprehensive information from the medical library. Here is a detailed, well-structured explanation of heart function.
Heart Function
Overview: The Heart as a Double Pump
The heart is essentially two separate pumps working in concert. The right heart pumps deoxygenated blood through the pulmonary circulation (lungs), while the left heart pumps oxygenated blood through the systemic circulation (rest of the body). Each side consists of an atrium (a weak primer pump) and a ventricle (the main pumping chamber).
The heart is enclosed in the pericardium, a two-layer protective sac that also anchors the heart in place.
- Guyton and Hall Textbook of Medical Physiology
1. Cardiac Muscle Structure
The heart contains three types of muscle:
- Atrial muscle - contracts to prime the ventricles
- Ventricular muscle - contracts powerfully to eject blood
- Specialized excitatory and conductive fibers - generate and conduct electrical impulses, enabling the rhythmic beat
Cardiac muscle fibers are arranged in a latticework pattern (dividing, recombining, and spreading), and like skeletal muscle, are striated with actin and myosin filaments. However, cardiac muscle has unique intercalated discs with gap junctions that allow action potentials to spread from one fiber to the next - making the heart muscle act as a functional syncytium (all fibers contract together).
There are actually two syncytia: the atrial syncytium and the ventricular syncytium, separated by fibrous tissue. Impulses pass between them only through the AV bundle (Bundle of His), ensuring the atria contract just before the ventricles.
2. Left Ventricular Torsion (Wringing Motion)
The left ventricular wall has a sophisticated double-helix fiber arrangement:
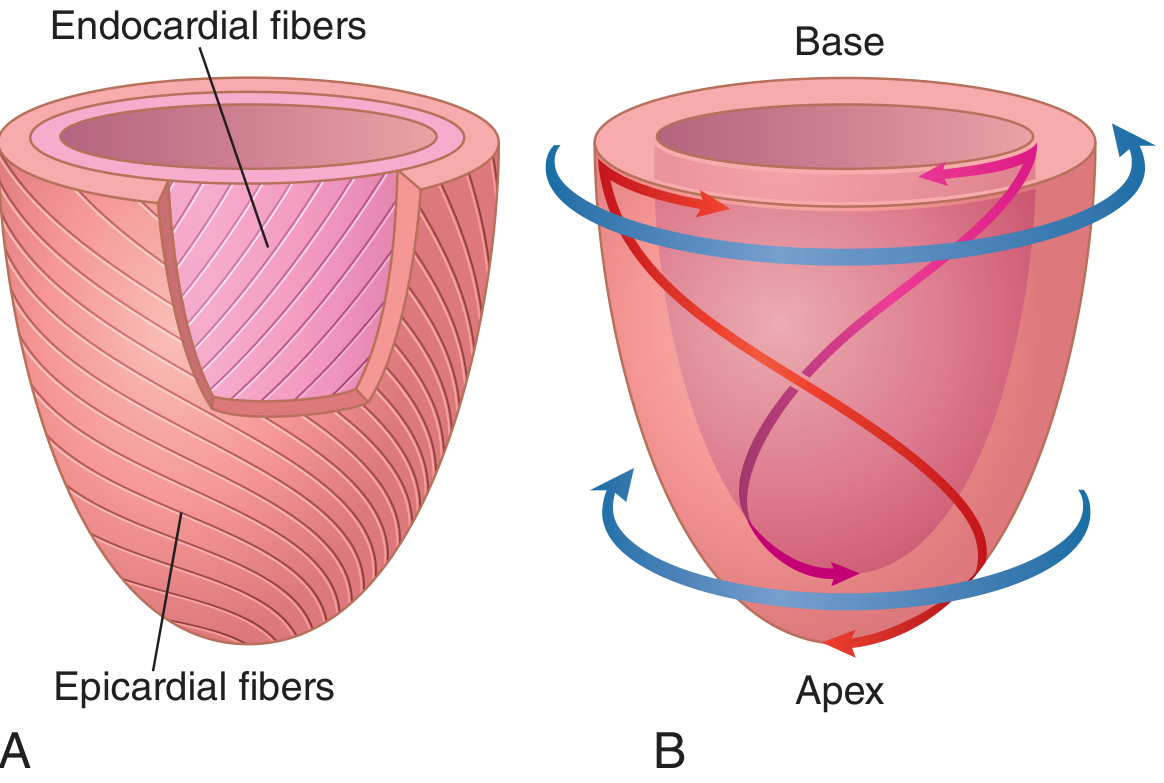
- Subepicardial (outer) fibers spiral in a left-handed helix
- Subendocardial (inner) fibers spiral in a right-handed helix
During contraction, the apex rotates counterclockwise and the base rotates clockwise (viewed from the apex). This creates a "wringing" or twisting motion that:
- Increases ejection efficiency during systole
- Acts like a loaded spring to assist rapid ventricular filling during diastole (suction effect on recoil)
- Guyton and Hall Textbook of Medical Physiology
3. Action Potentials in Cardiac Muscle
The ventricular action potential has a characteristic plateau phase lasting ~0.2-0.3 seconds, caused by prolonged calcium channel opening. This plateau is what makes cardiac contraction last 15 times longer than skeletal muscle contraction - preventing tetanic (sustained) contraction, which would be fatal.
- Resting membrane potential: approximately -85 mV
- Peak depolarization: approximately +20 mV
- Atrial contraction duration: ~0.2 seconds
- Ventricular contraction duration: ~0.3 seconds
4. The Cardiac Cycle
The cardiac cycle covers all events from the start of one heartbeat to the next. At a normal heart rate of 72 beats/min, one complete cycle takes about 0.833 seconds.
Each cycle is initiated by a spontaneous action potential in the sinoatrial (SA) node in the right atrium. The impulse spreads across the atria, then pauses >0.1 second at the AV node before spreading to the ventricles - this delay allows atria to finish contracting (priming the ventricles) before ventricular contraction begins.
Seven Phases of the Cardiac Cycle:
| Phase | Event | Valves | Heart Sound |
|---|---|---|---|
| A - Atrial Systole | Atria contract, final ventricular filling | Mitral/tricuspid open | S4 (if present) |
| B - Isovolumetric Ventricular Contraction | Ventricles contract; pressure rises but volume unchanged | All valves closed | S1 ("lub") |
| C - Rapid Ventricular Ejection | Blood rapidly ejected into aorta/pulmonary artery | Aortic/pulmonary valves open | - |
| D - Reduced Ventricular Ejection | Slower ejection; ventricular volume reaches minimum | - | - |
| E - Isovolumetric Ventricular Relaxation | Ventricles relax; pressure drops; volume unchanged | All valves closed | S2 ("dub") |
| F - Rapid Ventricular Filling | Ventricles fill passively from atria | Mitral/tricuspid open | S3 (if present) |
| G - Reduced Ventricular Filling | Continued slow filling; completes ~70-80% of fill before atrial kick | - | - |
- Costanzo Physiology 7th Edition
Systole vs. Diastole
- Systole (contraction): At 72 bpm, occupies about 40% of the cardiac cycle
- Diastole (relaxation/filling): Occupies the remaining ~60%
- As heart rate rises, diastole shortens more than systole - at very high rates, the heart has insufficient time to fill, reducing output
5. Heart Valves
Four valves maintain one-directional blood flow:
| Valve | Location | Opens When | Closes When |
|---|---|---|---|
| Mitral (bicuspid) | Left AV | LV pressure < LA pressure | LV pressure > LA pressure |
| Tricuspid | Right AV | RV pressure < RA pressure | RV pressure > RA pressure |
| Aortic | LV outflow | LV pressure > aortic pressure | LV pressure < aortic pressure |
| Pulmonary | RV outflow | RV pressure > pulmonary artery pressure | RV pressure < pulmonary artery pressure |
Valve closure produces the heart sounds: S1 ("lub") = mitral + tricuspid closure; S2 ("dub") = aortic + pulmonary closure.
6. Cardiac Output and Its Determinants
Cardiac output (CO) = Heart Rate (HR) × Stroke Volume (SV)
At rest: CO ≈ 5 L/min (HR ~72 bpm × SV ~70 mL)
Four major determinants of ventricular function:
| Factor | Definition | Effect |
|---|---|---|
| Preload | End-diastolic ventricular volume/stretch | More stretch → stronger contraction (Frank-Starling) |
| Afterload | Resistance the ventricle must overcome to eject blood | Higher afterload → lower stroke volume |
| Contractility (inotropy) | Intrinsic strength of contraction | Increased by catecholamines; decreased by hypoxia, ischemia |
| Heart rate (chronotropy) | Beats per minute | Increased by sympathetic drive; decreased by vagus nerve |
Frank-Starling Law
The Frank-Starling mechanism states that increasing end-diastolic volume (greater stretch) results in enhanced systolic function. At the cellular level, increased fiber length improves the overlap of actin-myosin filaments and increases calcium sensitivity of the contractile proteins - meaning the heart automatically pumps out what it receives.
- Miller's Anesthesia; Goldman-Cecil Medicine
7. Blood Flow Through the Heart (Summary)
Systemic veins
↓
Right Atrium → Tricuspid Valve → Right Ventricle
↓ (Pulmonary Valve)
Pulmonary Artery → Lungs (gas exchange)
↓
Pulmonary Veins
↓
Left Atrium → Mitral Valve → Left Ventricle
↓ (Aortic Valve)
Aorta → Systemic Circulation
8. Regulation of Heart Rate
- Sympathetic nervous system: Increases heart rate (positive chronotropy) and contractility (positive inotropy) via norepinephrine/epinephrine acting on β1-adrenergic receptors
- Parasympathetic (vagus nerve): Slows heart rate (negative chronotropy) via acetylcholine
- Intrinsic rate of the SA node: ~60-100 beats/min in adults; pacemaker cells spontaneously depolarize without external stimulation
Key Clinical Numbers (Normal)
| Parameter | Normal Value |
|---|---|
| Heart rate | 60-100 bpm |
| Stroke volume | ~70 mL |
| Cardiac output (rest) | ~5 L/min |
| Ejection fraction (EF) | 55-65% |
| End-diastolic volume (EDV) | ~120-130 mL |
| End-systolic volume (ESV) | ~50-60 mL |
Ejection Fraction = SV / EDV × 100
The heart's function integrates electrical initiation, mechanical contraction, valvular regulation, and autonomic control into a precisely coordinated pump that circulates the entire blood volume (~5 L) approximately once per minute at rest, and can increase output 4-5 fold during exercise.
- Guyton and Hall Textbook of Medical Physiology
- Costanzo Physiology 7th Edition
- Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.